- Finger & Thumb
- Foot & Toe
- Thigh & Groin
- All Plus Size
- Plus Size Knee Braces
- Plus Size Back Braces
- Hernia Belts
- Hip Supports
- Night Splints
- Pediatric / Kid's
- Plantar Fasciitis
- Posture Correctors
- Walker Boots
- Accessories
- View All Braces
- View Clearance Braces
- Shop Gift Cards
- Abdominal Pain & Injury Treatment
- Ankle Pain & Injury Treatment
- Back Pain & Injury Treatment
- Elbow Pain & Injury Treatment
- Finger & Thumb Pain Treatment
- Foot Pain & Toe Injury Treatment
- Knee Pain & Injury Treatment
- Neck Pain & Injury Treatment
- Shoulder Pain & Injury Treatment
- Wrist Pain & Injury Treatment
- Plus Size Supports for Obesity & Weight-Related Pain
- Knee Supports for Sports Injuries
- Court Comfort Collection for Racket Sports Support
- Brace Finder
- Customer Help Center
Frequently Bought Together
- Shop by Brace --> Abdominal --> Ankle Back Elbow Finger & Thumb Foot & Toe Knee Shoulder Thigh & Groin Wrist --> All Plus Size Supports --> Plus Size Knee Braces Plus Size Back Braces Hernia Belts Hip Supports Night Splints Pediatric / Kid's Plantar Fasciitis Posture Correctors Walker Boots Accessories --> View All Braces --> Shop Sale Braces Final-Sale Clearance Braces Shop Gift Cards
- Shop by Injury/Condition --> Abdominal Pain & Injury Treatment --> Ankle Pain & Injury Treatment Back Pain & Injury Treatment Elbow Pain & Injury Treatment --> Finger & Thumb Pain Treatment --> Foot Pain & Toe Injury Treatment Knee Pain & Injury Treatment Neck Pain & Injury Treatment Shoulder Pain & Injury Treatment --> Wrist Pain & Injury Treatment --> --> Plus Size Supports for Obesity & Weight-Related Pain --> --> Knee Supports for Sports Injuries --> --> Court Comfort Collection for Racket Sports Support -->
Oct 05, 2023

Spondylolisthesis Grading: How to Diagnose and Treat Grades 1, 2, 3, 4 and 5
What grade of spondylolisthesis do i have.
Like many other conditions, spondylolisthesis can be measured using a grading system, where your spondylolisthesis grade is based on the degree of displacement of your vertebrae. Grades of spondylolisthesis influence what symptoms you might experience as well as what treatment you will likely receive.
Wondering what might be the cause of your spondylolisthesis? Read more about the causes and symptoms .
The grade of your condition is based on the distance from the posterior edge of the superior body of the vertebrae to the same edge of the inferior vertebral body. The ratings range from spondylolisthesis grade 1 to spondylolisthesis grade 5: grade 1 spondylolisthesis being least severe and grade 5 most severe. To diagnose this condition, your doctor will take X-rays in order to see if any of the bones in your vertebrae have slipped or are misaligned. They may order a CT scan or MRI to figure out how severe your slippage may be.
Do I Have Grade 1 Spondylolisthesis?

Grade I, or grade 1 spondylolisthesis is the least severe case. The degree of slippage for spondylolisthesis grade 1 ranges from 0%-25%. Grade 1 anterior spondylolisthesis usually occurs in the l4 on the l5 segment of the spine, which is connected, to your facet joints. Fortunately, spondylolisthesis conditions are typically not very severe, leaving grade 1 and grade 2 being the most frequent gradings.
Spondylolisthesis grade 1 treatment is typically using conservative methods since the slippage isn’t very severe. For starters, bed rest can help relieve your pain and take the extra stress off of your spine and back. In addition, try avoiding activities that may further your injury and slippage such as high contact sports.
Do I Have Grade 2 Spondylolisthesis?

Similar to grade 1, grade 2 is a low-grade spondylolisthesis. Grade ii spondylolisthesis degree of slippage is between 26% to 50%.
Spondylolisthesis grade 2 treatment is similar to grade 1, it starts with conservative methods such as resting, anti-inflammatory medications, and reducing the number of daily activities that may harm your back. Exercises and stretches for spondylolisthesis help strengthen the muscles surrounding your spine and is another great conservative treatment option.
Physical therapy works similarly. It helps to improve the strength and flexibility of your back and other parts of the core, which can reduce the amount of pressure the spine, endures. This ultimately relieves discomfort associated with grade 1 spondylolysis or spondylolisthesis grade 2 and helps slow additional slippage.
For those whose grade 2 spondylolisthesis condition doesn’t respond to such methods above or if you feel as though your condition is worsening, try bracing to help immobilize your spine. Such braces are usually used for individuals with 50% slippage or less.

Do I Have Grade 3 Spondylolisthesis?

Grade 3 spondylolisthesis tends to be on the more serious side of the spectrum. Grade iii spondylolisthesis slippage is between 51% to 75%.
Grade 3 spondylolisthesis treatment typically involves the same conservative methods mentioned above, but if your condition persists or get worse, surgery for spondylolisthesis is an option for this grade.
Before considering surgery for spondylolisthesis grade 3, it’s important to take in consideration:
- If your pain from spondylolisthesis has lasted for 6-12 months and has not improved
- If your slip is progressing
- If you are having trouble walking, sleeping, etc.
- If you are an obese individual, you may have a higher risk for surgery complications
Do I Have Grade 4 Spondylolisthesis?
Grade 4 spondylolisthesis goes along with grade 3 but is more severe. Spondylolisthesis grade 4 slippage is between 76% to 100%.
Treatment options for spondylolisthesis more commonly involve isthmic and degenerative surgery . Surgery for spondylolisthesis can help the instability in your spine as well as relieve compression that is being placed on your nerve roots.
Do I Have Grade 5 Spondylolisthesis or Spondyloptosis?

For grade 5 spondylolisthesis, your vertebra has completely fallen off the next vertebra. When the vertebra slides completely off the vertebra that is supposed to be beneath it, this is known as spondyloptosis.
For this rare condition, surgery is the only way to completely fix or heal spondylolisthesis of grade 5. Your surgeon may perform a vertebrectomy, which is an alternative procedure to help align your vertebra.
Related Articles

Have an L4-L5 Pars Defect in Your Spine? It Might be Spondylolisthesis

Intervertebral Disc Disease (IVDD) in Dogs: What to Expect

Quick Fixes & Tips for Better Posture Without Looking Silly
Join Our Community
Subscribe to our email list for exclusive offers and tips on healthy healing.
An Overview of Spondylolisthesis

What Is Spondylolisthesis?
Spondylolisthesis (pronounced spahn-duh-low-liss-thee-sus) is a condition in which one of the bones in your spine (the vertebrae) slips out of place and moves on top of the vertebra next to it.
It usually happens at the base of your spine (lumbar spondylolisthesis). When the slipped vertebra puts pressure on a nerve, it can cause pain in your lower back or legs.
Spondylolisthesis Symptoms
Sometimes, people with this condition don't notice anything is wrong. But you can have symptoms that include:
- Lower back pain
- Muscle tightness and stiffness
- Pain in your buttocks
- Pain that spreads down your legs (due to pressure on nerve roots)
- Pain that gets worse when you move around
- Tight hamstrings (muscles in the back of your thighs)
- Trouble standing or walking
Spondylolisthesis vs. Spondylolysis
Spondylolysis (pronounced spahn-duh-loll-iss-us) and spondylolisthesis are different conditions of the spine, though they're sometimes related. Both conditions cause pain in your lower back .
Spondylolysis is a weakness or small fracture (crack) in one of your vertebrae. This usually affects your lower back, but it can also happen in the middle of your back or your neck. It's most often found in kids and teens, especially those involved in sports that repeatedly overstretch the lower spine, like football or gymnastics.
It's not uncommon for people with spondylolysis to also have spondylolisthesis. That's because the weakness or fracture in your vertebra may cause it to move out of place.
Types of Spondylolisthesis
Doctors divide this condition into six main types, determined by cause.
Degenerative spondylolisthesis: This is the most common type. As people age, the disks that cushion vertebrae can become worn, dry out, and get thinner. This makes it easier for the vertebra to slip out of place.
Isthmic spondylolisthesis: This type is caused by spondylosis. A crack in the vertebra can lead it to slip backward, forward, or over a bone below. It may affect kids and teens who do gymnastics, do weightlifting, or play football because they repeatedly overextend their lower backs. But it also sometimes happens when you're born with vertebrae whose bone is thinner than usual.
Congenital spondylolisthesis: Also known as dysplastic spondylolisthesis, this happens when your vertebrae are aligned incorrectly due to a birth defect.
Traumatic spondylolisthesis: In this type, an injury (trauma) to the spine causes the vertebra to move out of place.
Pathological spondylolisthesis: This type is caused by another spine condition, such as osteoporosis or a spinal tumor.
Postsurgical spondylolisthesis: Also called iatrogenic spondylolisthesis, this happens when a vertebra slips out of place after spinal surgery.
Grades of Spondylolisthesis
Your doctor may give your spondylolisthesis a grade based on how serious it is. The most common grading system is called Meyerding's classification and includes:
- Grade I : The most common grade, this is defined as 1%-25% slippage of the vertebra
- Grade II : Up to 50% slippage of the vertebra
- Grade III : Up to 75% slippage
- Grade IV : 76%-100% slippage
- Grade V : More than 100% slippage, also known as spondyloptosis
Grades I and II are considered low grade. Grades III and up are considered high grade.
Spondylolisthesis Causes and Risk Factors
Causes of spondylolisthesis include:
- Wear and tear with age
- Birth defects
- Spondylolysis
- Injury to the spine
- Another condition such as a spinal tumor or osteoporosis
- Spinal surgery
You're more likely to get this condition if you:
- Take part in sports that put stress on your spine
- Were born with thinner areas of vertebrae that are prone to breaking and slipping
- Are 50 or older
- Have a degenerative spinal condition
Spondylolisthesis Diagnosis
If your doctor thinks you might have this condition, they'll ask about your symptoms and run imaging tests to see if a vertebra is out of place. These tests may include:
These tests can also help your doctor determine a grade for your spondylolisthesis.
Spondylolisthesis Treatments
The treatment you'll need depends on what grade of spondylolisthesis you have, as well as your age, symptoms, and your medical history. Low grade can usually be treated with physical therapy or medications. With high grade, you may need surgery, especially if you're in a lot of pain.
Nonsurgical treatment options include:
- Rest : You may need to take some time off from sports and other vigorous activities.
- Medications : Your doctor may recommend over-the-counter anti-inflammatory medicines to relieve your pain, such as ibuprofen or naproxen.
- Injections : Steroid shots in the area where you have pain can bring relief.
- Physical therapy : Daily exercises that stretch and strengthen your supportive abdominal and lower back muscles can lower your pain.
- Braces : For children with fractures in the vertebrae (spondylolysis), a back brace can restrict movement so the fractures can heal.
Spondylolisthesis Surgery
If you have high-grade spondylolisthesis or if you still have serious pain and disability after nonsurgical treatments, you may need surgery. This usually means spinal decompression, often along with spinal fusion.
Spinal surgery is always done under general anesthesia , which means you're asleep during the operation.
Spinal decompression: Decompression lessens the pressure on the nerves in your spine to relieve pain. There are several techniques your surgeon can use to give your nerves more room. They may remove bone from your spine, take out part or all of a disk, or make the opening in your spinal canal larger. Your surgeon might need to use all these methods during your surgery.
Spinal fusion: In spinal fusion, the doctor joins, or fuses, the affected vertebrae together to prevent them from slipping again. After this surgery, you may have a bit less flexibility in your spine.
Pars repair: This surgery repairs fractures in the vertebrae using small wires or screws. Sometimes, a bone graft is used to reinforce the fracture so it can heal better.
After spinal surgery, you'll likely need to stay in the hospital for at least a day. Most people can go home within a week. You may be able to stand or even walk the day after the operation. You may go home with pain medication to ensure that your recovery is as easy as possible.
You'll need to limit physical activity for 8-10 weeks after your surgery so your spine can heal. But you should still move around and even walk every day. This can make your recovery go faster and help keep complications at bay.
Around 10-12 weeks after your surgery, you'll start physical therapy to stretch and strengthen your muscles and help you move more easily. Ideally, you should have physical therapy for a year.
For the first year after your surgery, you'll need to see your surgeon about every 3 months. You'll likely have X-rays taken at these follow-ups to make sure your spine is healing well.
Spondylolisthesis Complications
Serious spondylolisthesis sometimes leads to another condition called cauda equina syndrome . This is a serious condition in which nerve roots in part of your lower back called the cauda equina get compressed. It can cause you to lose feeling in your legs. It also can affect your bladder.
This is a medical emergency. If left untreated, cauda equina syndrome can lead to a loss of bladder control and paralysis.
See your doctor if you:
- Have trouble controlling your bladder or bowels
- Notice numbness or a strange sensation between your legs or on your buttocks, inner thighs, backs of your legs, feet, or heels
- Have pain or weakness in a leg or both legs that may cause stumbling
The symptoms may come on slowly and vary in how serious they are.
Spondylolisthesis Outlook
For most people, rest and nonsurgical treatments bring long-term relief within several weeks. But sometimes, spondylolisthesis comes back again after treatment. This happens more often when it was a higher grade.
If you've had surgery, you'll most likely do well afterward. Most people get back to normal activities within a few months. But your spine may not be as flexible as it was before.
Spondylolisthesis is when one of your vertebrae moves out of place. This sometimes leads to back pain and other symptoms. It can be usually treated with rest, medication, and/or physical therapy. But serious cases may require surgery.
Spondylolisthesis FAQs
What is the main cause of spondylolisthesis?
In adults, it most often happens when cartilage and bones in the spine become worn from conditions such as arthritis. It's more common in people age 50 and older. In kids and teens, the most common causes are either a spinal birth defect or injury to the spine.
Is spondylolisthesis a serious condition?
For most people, it's not serious. Many people have few symptoms or no symptoms at all. It's only a problem when it causes pain or limits your ability to move. If that happens, you'll need to see a doctor for treatment.

Top doctors in ,
Find more top doctors on, related links.
- Back Pain News
- Back Pain Reference
- Back Pain Slideshows
- Back Pain Quizzes
- Back Pain Videos
- Back Pain Medications
- Find a Neurologist
- Find a Pain Medicine Specialist
- WebMDRx Savings Card
- Ankylosing Spondylitis
- Drug Interaction Checker
- Osteoporosis
- Pain Management
- Pill Identifier
- Second Opinions
- SI Joint Pain
- More Related Topics
Spondylolisthesis: Definition, Causes, Symptoms, and Treatment
by Dave Harrison, MD • Last updated November 26, 2022
- Click to share on Twitter (Opens in new window)
- Click to share on Facebook (Opens in new window)
- Click to share on LinkedIn (Opens in new window)
- Click to share on Pinterest (Opens in new window)
- Click to share on Reddit (Opens in new window)

What is Spondylolisthesis?
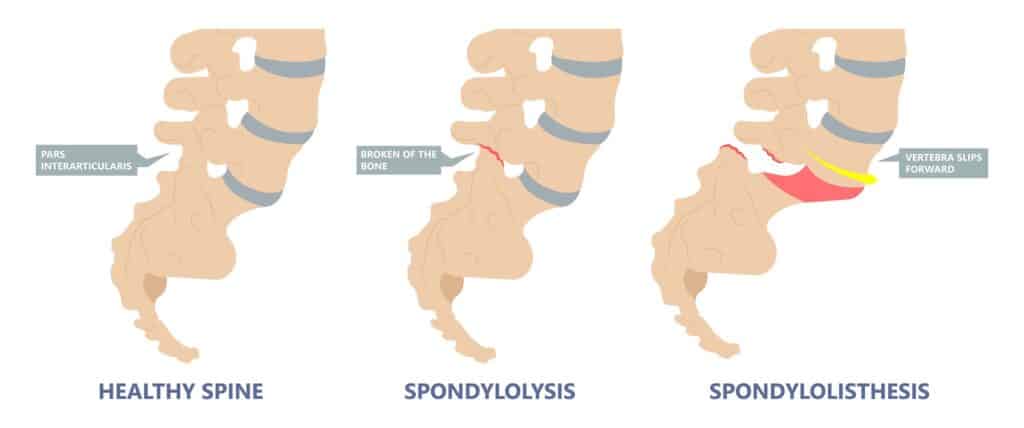
The spine is comprised of 33 bones, called vertebra , stacked on top of each other interspaced by discs . Spondylolisthesis is a condition where one vertebra slips forward or backwards relative to the vertebra below. More specifically, retrolisthesis is when the vertebra slips posteriorly or backwards, and anterolisthesis is when the vertebra slips anteriorly or forward.
Spondylosis vs Spondylolisthesis
Spondylosis and Spondylolisthesis are different conditions. They can be related but are not the same. Spondylosis refers to a fracture of a small bone, called the pars interarticularis, which connects the facet joint of the vertebra to the one below. This may lead to instability and ultimately slippage of the vertebra. Spondylolisthesis, on the other hand, refers to slippage of the vertebra in relation to the one below.
Types and Causes of Spondylolisthesis
There are several types of spondylolisthesis, often classified by their underlying cause:
Degenerative Spondylolisthesis
Degenerative spondylolisthesis is the most common cause, and is due to general wear and tear on the spine. Overtime, the bones and ligaments which hold the spine together may become weak and unstable.
Isthmic Spondylolisthesis
Isthmic spondylolisthesis is the result of another condition, called “ spondylosis “. Spondylosis refers to a fracture of a small bone, called the pars interarticularis, which connects the facet joint of the vertebra to the one below. If this interconnecting bone is broken, it can lead to slippage of the vertebra. This can sometimes occur during childhood or adolsence but go unnoticed until adulthood when degenerative changes cause worsening slippage.
Congenital Spondylolisthesis
Congenital spondylolisthesis occurs when the bones do not form correctly during fetal development
Traumatic Spondylolisthesis
Traumatic spondylolisthesis is the result of an injury such as a motor vehicle crash
Pathologic Spondyloslisthesis
Pathologic spondylolisthesis is when other disorders weaken the points of attachment in the spine. This includes osteoporosis, tumors, or infection that affect the bones and ligaments causing them to slip.
Iatrogenic Spondylolisthesis
Iatrogenic spondylolisthesis is the result of a prior surgery. Some operations of the spine, such as a laminectomy, may lead to instability. This can cause the vertebra to slip post operatively.
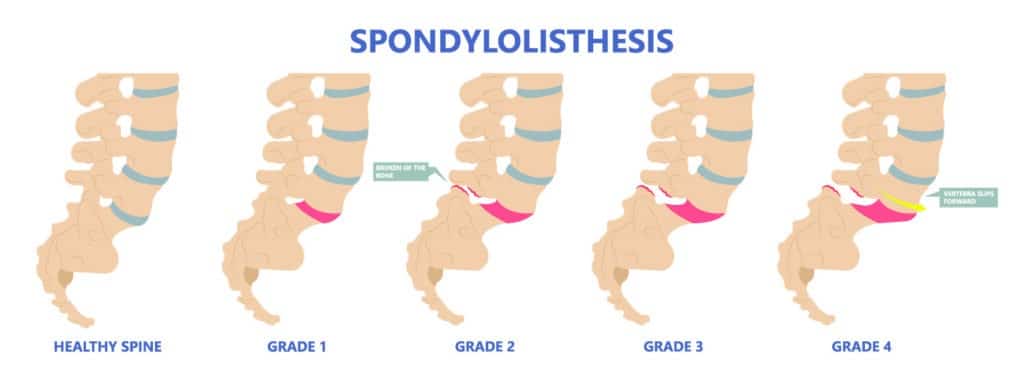
Spondylolisthesis Grades
Spondylolisthesis is classified based on the degree of slippage relative to the vertebra below
- Grade 1 : 1 – 25 % forward slip. This degree of slippage is usually asymptomatic.
- Grade 2: 26 – 50 % forward slip. May cause mild symptoms such as stiffness and pain in your lower back after physical activity, but it’s not severe enough to affect your everyday activities.
- Grade 3 : 51 – 75 % forward slip. May cause moderate symptoms such as pain after physical activity or sitting for long periods.
- Grade 4: 76 – 99% forward slip. May cause moderate to severe symptoms.
- Grade 5: Is when the vertebra has slipped completely of the spinal column. This is a severe condition known as “spondyloptysis”.
Symptoms of Spondylolisthesis
Spondylolisthesis can cause compression of spinal nerves and in severe cases, the spinal cord. The symptoms will depend on which vertebra is affected.
Cervical Spondylolisthesis (neck)
- Arm numbness or tingling
- Arm weakness
Lumbar Spondylolisthesis (low back)
- Buttock pain
- Leg numbness or tingling
- Leg weakness
Diagnosing Spondylolisthesis
Your doctor may order imaging tests to confirm the diagnosis and determine the severity of your spondylolisthesis. The most common imaging tests used include:
- X-rays : X-rays can show the alignment of the vertebrae and any signs of slippage.
- CT scan: A CT scan can provide detailed images of the bones and soft tissues in your back, allowing your doctor to see any damage or abnormalities.
- MRI: An MRI can show the spinal cord and nerves, as well as any herniated discs or other soft tissue abnormalities.
Treatments for Spondylolisthesis
Medications.
For those experiencing pain, oral medications are first line treatments. This includes non-steroidal anti-inflammatory medications (NSAIDs) such as ibuprofen, acetaminophen, or in severe cases opioids or muscle relaxants (with extreme caution). Topical medications such as lidocaine patches are also sometimes used.
Physical Therapy
Physical therapy can help improve mobility and strengthen muscles around your spine to stabilize your neck and lower back. You may also receive stretching exercises to improve flexibility and balance exercises to improve coordination.
Surgery is reserved for severe cases of spondylolisthesis in which there is a high degree of instability and symptoms of nerve compression.
In these cases a spinal fusion may be necessary. This surgery joins two or more vertebra together using rods and screws, in order to improve stability.
Reference s
- Alfieri A, Gazzeri R, Prell J, Röllinghoff M. The current management of lumbar spondylolisthesis. J Neurosurg Sci. 2013 Jun;57(2):103-13. PMID: 23676859.
- Stillerman CB, Schneider JH, Gruen JP. Evaluation and management of spondylolysis and spondylolisthesis. Clin Neurosurg. 1993;40:384-415. PMID: 8111991.
About the Author
Dave Harrison, MD
Dr. Harrison is a board certified Emergency Physician with a part time appointment at San Francisco General Medical Center and is an Assistant Clinical Professor-Volunteer at the UCSF School of Medicine. Dr. Harrison attended medical school at Tufts University and completed his Emergency Medicine residency at the University of Southern California. Dr. Harrison manages the editorial process for SpineInfo.com.
- Our Reviews
- Our Hospitals and Treatment Centers
- Interventional Pain Management
- Orthopedic Spine Surgery
- Atypical Face Pain
- Carpal Tunnel Syndrome
- Complex Regional Pain Syndrome
- Degenerative Disc Disease
- Failed Back Surgery
- Fibromyalgia
- Headaches and Migraines
- Minimally Invasive Spine Surgery
- Muscle Spasms
- Pancreatitis
- Pelvic Pain
- Peripheral Neuropathy
- Peripheral Vascular Disease
- Phantom Limb Pain
- Post-Operative Pain
- Anterior Cervical Discectomy And Fusion
- Caudal Epidural With Lysis Of Adhesions
- Electroencephalography
- Electromyography and Nerve Conduction Velocity Studies
- Epidural Steroid Injections
- Facet Injections
- IFuse Implant System
- Intrathecal Pump
- Kyphoplasty
- Laminectomy And Fusion
- Medial Branch Blocks and Neurotomies
- Microdiscectomy
- Pain Management
- Peripheral Field Stimulators
- Selective Nerve Root Blocks
- Small And Large Joint Injections
- Patient Portal
- Accepted Insurance
- Data Breach Notification
- Notice of Privacy Practices
Spondylolisthesis: Understanding Causes, Symptoms & Treatment
Are you experiencing lower back pain that won't go away? Have you or a loved one recently been diagnosed with spondylolisthesis? If so, you're not alone. Spondylolisthesis is a common condition that affects the spine, and understanding its causes, symptoms, and treatment is crucial for managing and improving your quality of life.
This blog post will explore everything you need about spondylolisthesis, including its various forms, underlying causes, and effective treatment options. So, whether you're dealing with this condition or simply looking to educate yourself on this joint spine issue, keep reading to understand better spondylolisthesis and how to address it effectively.

What is Spondylolisthesis?
Spondylolisthesis is a common condition that affects the spine and can cause discomfort and pain for those with it. It occurs when one vertebra (bone in the spine) slips forward over another vertebra, causing the spinal column to become misaligned. This condition can affect people of all ages, but it is most commonly seen in adults over 50 .
What is the root cause of Spondylolisthesis?
The most common cause of spondylolisthesis is a fracture or defect in the pars interarticularis , a small bony section of the vertebra. This fracture can be caused by repetitive stress due to sports or activities that pressure the spine, such as weightlifting, gymnastics, or football. It can also happen due to congenital conditions or degenerative diseases like arthritis. Sometimes, spondylolisthesis can be caused by sudden trauma, such as a car accident or a fall.
What are the signs and symptoms of Spondylolisthesis?

The symptoms of spondylolisthesis vary depending on the severity of the condition. In mild cases, there may be no noticeable symptoms, but as the condition progresses, symptoms may include:
- Lower back pain
- Muscle spasms in the back
- Stiffness in the back
- Numbness or tingling in the legs
- Difficulty standing or walking
- Decreased range of motion in the back
- Weakness in the legs
How do you stop spondylolisthesis from progressing?
How exactly do you stop spondylolisthesis from worsening? There are practical strategies for managing and halting the progression of spondylolisthesis. Get ready to take control of your spinal health and stop spondylolisthesis in its tracks.
- Exercise regularly – Regular exercise helps to strengthen the muscles in your back and abdomen, providing better support for your spine. However, if you have spondylolisthesis, some exercises may be harmful. Consult a physical therapist to create a safe, individualized exercise plan for your condition.
- Avoid high-impact activities – Jumping and landing on the feet, such as running or basketball, can put additional stress on the spine. Instead, opt for low-impact exercises like swimming or cycling.
- Practice good posture – Poor posture can contribute to spondylolisthesis. Make a conscious effort to maintain good posture throughout the day, whether sitting, standing, or bending over. Consider using a lumbar support cushion if you spend much time sitting.
- Lose weigh t – Being overweight stresses the spine, which can worsen spondylolisthesis. Maintaining a healthy weight can help ease symptoms and stop the condition from progressing.
- Avoid lifting heavy objects – Putting strain on the lower back can worsen spondylolisthesis. If you need to lift heavy objects, use proper lifting techniques, such as bending your knees and keeping your back straight.
- Consider chiropractic care – Chiropractic manipulation and adjustments can help improve joint function and decrease pain in spondylolisthesis patients.
- Seek medical treatment – If you have persistent symptoms of spondylolisthesis, it's crucial to seek medical treatment. Your doctor may recommend physical therapy, pain medication, or in severe cases, surgery.
What are the 5 stages of spondylolisthesis?
Understanding the stages of spondylolisthesis is essential to identify its severity and manage it effectively. These are the five stages of spondylolisthesis and the accompanying symptoms.
Stage 1: Grade 1 Spondylolisthesis
The first stage of spondylolisthesis is also known as mild spondylolisthesis and is characterized by the slippage of less than 25% of one vertebra over another. In this stage, the symptoms may be minimal, and most people may not experience any. However, some common symptoms of grade 1 spondylolisthesis include mild back pain, stiffness, and muscle tightness in the lower back.
Stage 2: Grade 2 Spondylolisthesis
Grade 2 spondylolisthesis is characterized by the slippage of 26% to 50% of one vertebra over another. At this stage, the symptoms can become more noticeable, including increased back pain, numbness or tingling in the legs or feet, and difficulty standing or walking for extended periods. This stage may also lead to changes in posture and decreased flexibility in the lower back.
Stage 3: Grade 3 Spondylolisthesis
In this stage, the slippage increases to 51% to 75% of one vertebra over another. At this point, the spinal deformity may become apparent. Patients may experience severe back pain that radiates to the hips and legs, making it difficult to perform daily activities. Nerve compression is also standard in this stage, leading to symptoms like weakness, numbness, and tingling in the legs.
Stage 4: Grade 4 Spondylolisthesis
Grade 4 spondylolisthesis is characterized by the slippage of more than 75% of one vertebra over another. This stage can be severely debilitating, causing extreme back pain, nerve compression, and even difficulty in controlling bladder and bowel movements. Patients may also experience weakness and numbness in the legs, making it challenging to walk or stand for extended periods.
Stage 5: Grade 5 Spondylolisthesis
The final stage of spondylolisthesis, grade 5, is also known as spondyloptosis. In this stage, the slippage is more than 100% of one vertebra over another, meaning the vertebra has completely slipped off the one below it. At this point, the spinal deformity is severe and can lead to life-altering symptoms, including severe back pain, nerve damage, and loss of motor control in the legs.
Treatment options for Spondylolisthesis
Various treatment options for spondylolisthesis can help manage and relieve its symptoms. Let’s explore these treatment options and how they can help those with spondylolisthesis.
- Physical therapy:
Physical therapy is often the first line of treatment for spondylolisthesis. A physical therapist will work with the patient to strengthen the muscles in the back and abdomen, which can help stabilize the spine and prevent further slippage. They will also teach the patient proper posture and body mechanics to reduce pressure on the affected area. Physical therapy can also include exercises to increase flexibility and range of motion, which can help alleviate pain and stiffness.
- Medications:
Over-the-counter pain relievers such as ibuprofen and acetaminophen can help manage the pain caused by spondylolisthesis. Sometimes, a doctor may prescribe more vital pain medication or muscle relaxants if the pain is severe. However, these medications should only be used under the supervision of a doctor and are not a long-term solution for managing the condition.
- Bracing:
In some cases, a back brace may be recommended to provide support and stability to the affected area. This can help alleviate pain and prevent further slippage. It is crucial to work with a physical therapist to ensure the proper fit and usage of the brace.
- Steroid injections:
If other treatment options do not provide enough relief, a doctor may recommend steroid injections. These injections can help reduce inflammation and pain in the affected area. They are generally used as a short-term solution and may need to be repeated periodically.
- Surgery:
In severe cases of spondylolisthesis, surgery may be required. The most common surgery for this condition is spinal fusion, where the affected vertebrae are fused together to prevent slippage. This surgery can help alleviate pain and prevent further damage to the spine and nerves.
Get lasting relief from Spondylolisthesis!
Ready to take control of your Spondylolisthesis and find lasting relief? Look no further than Neuro Spine & Pain Center - your top choice for comprehensive treatment and expert care for Miami pain management .
Our team of renowned spine specialists in Miami understands the complexity of Spondylolisthesis and is dedicated to creating personalized treatment plans to address its underlying causes. From advanced imaging techniques to cutting-edge therapies, we have the tools to help you overcome this condition and live your life to the fullest.
Don't let Spondylolisthesis hold you back any longer, schedule a consultation with our experts today and let us guide you towards a pain-free and active lifestyle.

The material on this site is for informational purposes only and DOES NOT CONSTITUTE THE PROVIDING OF MEDICAL ADVICE, and is not intended to be a substitute for independent professional medical judgment, advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare provider with any questions or concerns you may have regarding your health.
Patient center
FAQ Notice of Privacy Practices Data Breach Notification Accepted Insurance
Usefull Links
Home Referring Providers About Us Contact Us
Copyright © 2023 Neuro Spine and Pain Center
Spondylolisthesis
Spondylolisthesis is where one of the bones in your spine, called a vertebra, slips forward. It can be painful, but there are treatments that can help.
It may happen anywhere along the spine, but is most common in the lower back.
Check if you have spondylolisthesis
The main symptoms of spondylolisthesis include:
- pain in your lower back, often worse when standing or walking and relieved when sitting or bending forward
- pain spreading to your bottom or thighs
- tight hamstrings (the muscles in the back of your thighs)
- pain, numbness or tingling spreading from your lower back down 1 leg ( sciatica )
Spondylolisthesis does not always cause symptoms.
Spondylolisthesis is not the same as a slipped disc . This is when the tissue between the bones in your spine pushes out.
Non-urgent advice: See a GP if:
- you have lower back pain that does not go away after 3 to 4 weeks
- you have pain in your thighs or bottom that does not go away after 3 to 4 weeks
- you're finding it difficult to walk or stand up straight
- you're worried about the pain or you're struggling to cope
- you have pain, numbness and tingling down 1 leg for more than 3 or 4 weeks
What happens at your GP appointment
If you have symptoms of spondylolisthesis, the GP may examine your back.
They may also ask you to lie down and raise 1 leg straight up in the air. This is painful if you have tight hamstrings or sciatica caused by spondylolisthesis.
The GP may arrange an X-ray to see if a bone in your spine has slipped forward.
You may have other scans, such as an MRI scan , if you have pain, numbness or weakness in your legs.
Treatments for spondylolisthesis
Treatments for spondylolisthesis depend on the symptoms you have and how severe they are.
Common treatments include:
- avoiding activities that make symptoms worse, such as bending, lifting, athletics and gymnastics
- taking anti-inflammatory painkillers such as ibuprofen or stronger painkillers on prescription
- steroid injections in your back to relieve pain, numbness and tingling in your leg
- physiotherapy to strengthen and stretch the muscles in your lower back, tummy and legs
The GP may refer you to a physiotherapist, or you can refer yourself in some areas.
Waiting times for physiotherapy on the NHS can be long. You can also get it privately.
Surgery for spondylolisthesis
The GP may refer you to a specialist for back surgery if other treatments do not work.
Types of surgery include:
- spinal fusion – the slipped bone (vertebra) is joined to the bone below with metal rods, screws and a bone graft
- lumbar decompression – a procedure to relieve pressure on the compressed spinal nerves
The operation is done under general anaesthetic , which means you will not be awake.
Recovery from surgery can take several weeks, but if often improves many of the symptoms of spondylolisthesis.
Talk to your surgeon about the risks and benefits of spinal surgery.
Causes of spondylolisthesis
Spondylolisthesis can:
- happen as you get older – the bones of the spine can weaken with age
- run in families
- be caused by a tiny crack in a bone (stress fracture) – this is more common in athletes and gymnasts
Page last reviewed: 01 June 2022 Next review due: 01 June 2025
- See All Locations
- Primary Care
- Urgent Care Facilities
- Emergency Rooms
- Surgery Centers
- Medical Offices
- Imaging Facilities
- Neurology & Neurosurgery
- Obstetrics & Gynecology
- Orthopaedics
- Pediatrics at Guerin Children's
- Urgent Care
- Medical Records Request
- Insurance & Billing
- Pay Your Bill
- Advanced Healthcare Directive
- Initiate a Request
- Help Paying Your Bill
Spondylolisthesis
Spondylolisthesis is a displacement of a vertebra in which the bone slides out of its proper position onto the bone below it. Most often, this displacement occurs following a break or fracture.
Surgery may be necessary to correct the condition if too much movement occurs and the bones begin to press on nerves.
Other complications may include:
- Chronic back pain
- Sensation changes
- Weakness of the legs
- Temporary or permanent damage of spinal nerve roots
- Loss of bladder control
When a vertebra slips out of proper alignment, discs can be damaged. To surgically correct this condition, a spinal surgeon removes the damaged disc. The slipped vertebra is then brought back into line, relieving pressure on the spinal nerve.
Types of spondylolisthesis include:
- Dysplastic spondylolisthesis , caused by a defect in part of the vertebra
- Isthmic spondylolisthesis , may be caused by repetitive trauma and is more common in athletes exposed to hyperextension motions
- Degenerative spondylolisthesis , occurs with cartilage degeneration because of arthritic changes in the joints
- Traumatic spondylolisthesis , caused by a fracture of the pedicle, lamina or facet joints as a result of direct trauma or injury to the vertebrae
- Pathologic spondylolisthesis , caused by a bone defect or abnormality, such as a tumor
Symptoms may vary from mild to severe. In some cases, there may be no symptoms at all.
Spondylolisthesis can lead to increased lordosis (also called swayback), and in later stages may result in kyphosis, or round back, as the upper spine falls off the lower.
Symptoms may include:
- Lower back pain
- Muscle tightness (tight hamstring muscle)
- Pain, numbness or tingling in the thighs and buttocks
- Tenderness in the area of the vertebra that is out of place
- Weakness in the legs
- Stiffness, causing changes in posture and gait
- A semi-kyphotic posture (leaning forward)
- A waddling gate in advanced cases
- Lower-back pain along the sciatic nerve
- Changes in bladder function
Spondylolisthesis may also produce a slipping sensation when moving into an upright position and pain when sitting and trying to stand.
Spondylolisthesis may appear in children as the result of a birth defect or sudden injury, typically occurring between the fifth bone in the lower back (lumbar vertebra) and the first bone in the sacrum (pelvis).
In adults, spondylolisthesis is the result of abnormal wear on the cartilage and bones from conditions such as arthritis , trauma from an accident or injury, or the result of a fracture, tumor or bone abnormality.
Sports that place a great deal of stress on bones may cause additional deterioration, fractures and bone disease, which may cause the bones of the spine to become weak and shift out of place.
A simple X-ray of the back will show any cracks, fractures or vertebrae slippage that are the signs of spondylolisthesis.
A CT scan or an MRI may be used to further diagnose the extent of the damage and possible treatments.
Treatment for spondylolisthesis will depend on the severity of the vertebra shift. Stretching and exercise may improve some cases as back muscles strengthen.
Non-invasive treatments include:
- Heat/Ice application
- Pain medicine (Tylenol and/or NSAIDS)
- Physical therapy
- Epidural injections
Surgery may be needed to fuse the shifted vertebrae if the patient has:
- Severe pain that does not get better with treatment
- A severe shift of a spine bone
- Weakness of muscles in a leg or both legs
Surgical process realigns the vertebrae, fixing them in place with a small rod that is attached with a pedicle screw, adding stability to the spine with or without the addition to an interbody (bone graft or cage) placed between the vertebra from the side or front.
Choose a doctor and schedule an appointment.
Get the care you need from world-class medical providers working with advanced technology.
Cedars-Sinai has a range of comprehensive treatment options.
(1-800-233-2771)
Available 7 days a week, 6 am - 9 pm PT
Expert Care for Life™ Starts Here
Looking for a physician.
Spondylolisthesis: Back Condition and Treatment
What causes a vertebra to slip and what the different grades of spondylolisthesis look like.
The word spondylolisthesis derives from two parts: spondylo which means spine, and listhesis which means slippage. So, a spondylolisthesis is a forward slip of one vertebra (ie, one of the 33 bones of the spinal column) relative to another. Spondylolisthesis usually occurs towards the base of your spine in the lumbar area.

Spondylolisthesis Grades
Spondylolisthesis can be described according to its degree of severity. One commonly used description grades spondylolisthesis, with grade 1 being least advanced, and grade 5 being most advanced . The spondylolisthesis is graded by measuring how much of a vertebral body has slipped forward over the body beneath it.
Grade 1: 25% of vertebral body has slipped forward
Grade 2: 50%
Grade 3: 75%
Grade 4: 100%
Grade 5: Vertebral body completely fallen off (i.e., spondyloptosis)

How Do People Get Spondylolisthesis?
Approximately 5%-6% of males, and 2%-3% of females have a spondylolisthesis.
It becomes apparent more often in people who are involved with very physical activities such as weightlifting, gymnastics, or football.
Males are more likely than females to develop symptoms from the disorder, primarily due to their engaging in more physical activities.
Although some children under the age of 5 may be pre-disposed towards having a spondylolisthesis, or may indeed already have an undetected spondylolisthesis, it is rare that such young children are diagnosed with spondylolisthesis.
Spondylolisthesis becomes more common among 7-10 year olds. The increased physical activities of adolescence and adulthood, along with the wear-and-tear of daily life, result in spondylolisthesis being most common among adolescents and adults.
Types of Spondylolisthesis
Different types of spondylolisthesis may be caused in a various ways. Some examples are:
Developmental Spondylolisthesis
This type of spondylolisthesis may exist at birth, or may develop during childhood, but generally is not noticed until later in childhood or even in adult life.
Acquired Spondylolisthesis
Acquired spondylolisthesis can be caused in one of two ways:
With all of the daily stresses that are put on a spine, such as carrying heavy items and physical sports, the spine may wear out (ie, degenerate). As the connections between the vertebrae weaken, this may lead to spondylolisthesis.
A single or repeated force being applied to the spine can cause spondylolisthesis; for example, the impact of falling off a ladder and landing on your feet, or the regular impact to the spine endured by offensive linemen playing football.
What Symptoms Might I Notice ?
Many people with a spondylolisthesis will have no symptoms and will only become aware of the problem when it is revealed on an X-ray for a different problem. However, there are several symptoms that often accompany spondylolisthesis:
Pain in the low back, especially after exercise
Increased lordosis (ie, swayback).
Pain and/or weakness in one or both thighs or legs
Reduced ability to control bowel and bladder functions
Tight hamstring musculature
In cases of advanced spondylolisthesis changes may occur in the way people stand and walk; for example, development of a waddling style of walking. This causes the abdomen to protrude further, due to the lowback curving forward more. The torso (chest, etc.) may seem shorter; and muscle spasms in the lowback may occur.

Professor Rodts has done an excellent job at distilling the basics of spondylolisthesis into a concise easy to read layman's format. Anatomy and natural history are well described with the help of visual aids.
- Share via facebook
- Share via pinterest
- Share via twitter
- Share via mail
More Like This
Surgery for spondylolisthesis.

Spinal Bracing: A Treatment Option for Spondylolisthesis

What Makes Spondylolisthesis Worse

Degenerative Spondylolisthesis of the Lumbar Spine

- Degenerative Spondylolisthesis Symptoms
By: Marco Funiciello, DO, Physiatrist
Degenerative spondylolisthesis typically causes low back pain along with a cluster of symptoms and signs in one or both legs.
Degenerative Spondylolisthesis: Common Symptoms and Signs

Degenerative spondylolisthesis symptoms include neurogenic claudication, sciatica, and radiculopathy.
In degenerative spondylolisthesis, the degenerated facet joints and other parts of the vertebral bone tend to increase in size. The enlarged, abnormal bone then encroaches upon the central canal and/or nerve hole (foramen) causing spinal stenosis or foraminal stenosis.
In This Article:
- Degenerative Spondylolisthesis
- Degenerative Spondylolisthesis Treatment
- Surgery for Degenerative Spondylolisthesis
Degenerative Spondylolisthesis Video
These changes typically result in some combination of the following symptoms and signs.
Persistent low back pain
Low back pain caused by degenerative spondylolisthesis is usually persistent and described as a consistent dull ache, 1 Cushnie D, Johnstone R, Urquhart JC, Gurr KR, Bailey SI, Bailey CS. Quality of Life and Slip Progression in Degenerative Spondylolisthesis Treated Nonoperatively. Spine (Phila Pa 1976). 2018;43(10):E574-E579. doi: 10.1097/BRS.0000000000002429 but it may also feel like a sharp, stabbing sensation for some individuals.
The pain is typically localized in the low back region and may worsen with physical activity, standing, or walking.
Neurogenic claudication
Intermittent neurogenic claudication affects around 75% of people with degenerative spondylolisthesis. It is characterized by episodes of low back pain that radiate to both legs, along with accompanying sensations of tingling, a sensation of weakness, and hamstring spasm. 2 Li N, Scofield J, Mangham P, Cooper J, Sherman W, Kaye A. Spondylolisthesis. Orthop Rev (Pavia). 2022 Jul 27;14(4):36917. doi: 10.52965/001c.36917 . PMID: 35910544; PMCID: PMC9329062. , 3 García-Ramos CL, Valenzuela-González J, Baeza-Álvarez VB, Rosales-Olivarez LM, Alpizar-Aguirre A, Reyes-Sánchez A. Degenerative spondylolisthesis I: general principles. Espondilolistesis degenerativa lumbar I: principios generales. Acta Ortop Mex. 2020;34(5):324-328.. , 4 Wang YXJ, Káplár Z, Deng M, Leung JCS. Lumbar degenerative spondylolisthesis epidemiology: A systematic review with a focus on gender-specific and age-specific prevalence. J Orthop Translat. 2016;11:39-52. Published 2016 Dec 1. doi: 10.1016/j.jot.2016.11.001
It is possible to have any combination of symptoms and they typically occur during walking variable distances or prolonged standing. 2 Li N, Scofield J, Mangham P, Cooper J, Sherman W, Kaye A. Spondylolisthesis. Orthop Rev (Pavia). 2022 Jul 27;14(4):36917. doi: 10.52965/001c.36917 . PMID: 35910544; PMCID: PMC9329062.
Sciatica: Radiating leg pain
Back pain may radiate into the buttock, thighs, and into the leg and foot. 4 Wang YXJ, Káplár Z, Deng M, Leung JCS. Lumbar degenerative spondylolisthesis epidemiology: A systematic review with a focus on gender-specific and age-specific prevalence. J Orthop Translat. 2016;11:39-52. Published 2016 Dec 1. doi: 10.1016/j.jot.2016.11.001
Radiating leg pain is commonly known as sciatica . This pain occurs due to the irritation, compression, or inflammation of spinal nerve roots in the lower back. 4 Wang YXJ, Káplár Z, Deng M, Leung JCS. Lumbar degenerative spondylolisthesis epidemiology: A systematic review with a focus on gender-specific and age-specific prevalence. J Orthop Translat. 2016;11:39-52. Published 2016 Dec 1. doi: 10.1016/j.jot.2016.11.001
Radiculopathy: Abnormal sensations, weakness, and loss of muscle reflexes
When the spinal nerve roots are compressed or sufficiently inflamed and neurologic deficits are present, the condition is called radiculopathy . Radiculopathy may cause leg weakness and affect muscle reflexes. Additionally, numbness may be felt in the thigh, leg, and/or foot. 4 Wang YXJ, Káplár Z, Deng M, Leung JCS. Lumbar degenerative spondylolisthesis epidemiology: A systematic review with a focus on gender-specific and age-specific prevalence. J Orthop Translat. 2016;11:39-52. Published 2016 Dec 1. doi: 10.1016/j.jot.2016.11.001
It may be challenging to perform activities that require strength, such as walking, climbing stairs, or lifting objects.
Little Known Symptoms of Degenerative Spondylolisthesis
As degenerative spondylolisthesis progresses, the symptoms may lessen due to compensatory mechanisms of the spine that increase spinal stability and prevent further progression.
However, in some individuals, the progression may continue and cause the following symptoms and signs.
Sleep disturbances
Back pain and leg pain may cause disturbed sleep or trouble falling asleep. 5 Kalichman L, Hunter DJ. Diagnosis and conservative management of degenerative lumbar spondylolisthesis. Eur Spine J. 2008;17(3):327-335. doi: 10.1007/s00586-007-0543-3
For this reason, some individuals may choose to sleep in the fetal position (sleeping on the side with knees bent close to the chest) to relieve leg symptoms. 5 Kalichman L, Hunter DJ. Diagnosis and conservative management of degenerative lumbar spondylolisthesis. Eur Spine J. 2008;17(3):327-335. doi: 10.1007/s00586-007-0543-3
Restless leg syndrome
Leg pain and claudication may sometimes cause restless legs syndrome. In this condition, aching or burning pain in the calves causes an irresistible urge to move the legs continuously, causing disturbed sleep. 5 Kalichman L, Hunter DJ. Diagnosis and conservative management of degenerative lumbar spondylolisthesis. Eur Spine J. 2008;17(3):327-335. doi: 10.1007/s00586-007-0543-3
Difficulty walking and imbalance

Degenerative spondylolisthesis may cause difficulty walking and maintaining balance.
As degenerative spondylolisthesis progresses, difficulties with walking and maintaining balance may be experienced. These signs arise from nerve compression caused by the slipped vertebra and associated degenerative changes, Altered posture, muscle weakness and reduced coordination may result. 6 Studnicka K, Ampat G. Lumbosacral Spondylolisthesis. [Updated 2022 Sep 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560679/
There are many nerves in our legs that are responsible for relaying information to the brain about position and balance. If these nerves are irritated or compressed in the spine then the brain may not get the necessary information needed for good balance and posture control.
These changes can impact mobility and function, making it harder to engage in normal daily activities.
Limited range of motion
Degenerative spondylolisthesis can affect lumbar range of motion due to the degenerative bone changes that prevent full segmental motion. Muscle spasm and stiffness may result.
Individuals may find it challenging to twist or engage in activities that involve spinal movement. This restricted range of motion can contribute to discomfort and stiffness in the affected area.
Menopause-Related Spondylolisthesis Symptoms
The onset of menopause may accelerate normal degenerative changes of the lumbar vertebrae, discs, facet joints, and ligaments. 4 Wang YXJ, Káplár Z, Deng M, Leung JCS. Lumbar degenerative spondylolisthesis epidemiology: A systematic review with a focus on gender-specific and age-specific prevalence. J Orthop Translat. 2016;11:39-52. Published 2016 Dec 1. doi: 10.1016/j.jot.2016.11.001
Typically, the symptoms associated with this progression include low back pain, stiffness, and/or pain radiating down the leg (sciatica). 4 Wang YXJ, Káplár Z, Deng M, Leung JCS. Lumbar degenerative spondylolisthesis epidemiology: A systematic review with a focus on gender-specific and age-specific prevalence. J Orthop Translat. 2016;11:39-52. Published 2016 Dec 1. doi: 10.1016/j.jot.2016.11.001
Read more about Sciatica Symptoms
Diagnosis of Degenerative Spondylolisthesis

Radiating sciatica pain may occur in degenerative spondylolisthesis.
A physician trained in musculoskeletal conditions can help diagnose degenerative spondylolisthesis.
A comprehensive assessment of the patient’s history, past medical history, thorough physical examination, and review of any prior tests and imaging studies are performed.
During the review of patient history and the physical examination, physicians typically check for 7 Akkawi I, Zmerly H. Degenerative Spondylolisthesis: A Narrative Review. Acta Biomed. 2022;92(6):e2021313. Published 2022 Jan 19. doi: 10.23750/abm.v92i6.10526 :
- Pain pattern. Physicians ask about localized or radiating pain and the pattern of pain distribution to check if sciatica is present.
- Postural effects. In degenerative spondylolisthesis, pain is exacerbated while bending backward and relieved when bending forward.
- History of symptoms. Neurogenic claudication and hamstring spasm while walking or standing for variable periods of time may indicate spinal stenosis caused by degenerative spondylolisthesis.
If these symptoms and signs are noticed, the physician may order imaging tests to further investigate the condition.
Imaging Tests for Degenerative Spondylolisthesis

X-rays are helpful in diagnosing and assessing the extent of degenerative spondylolisthesis.
Imaging tests may help confirm the diagnosis of degenerative spondylolisthesis and provide evidence of the extent of progression of the condition.
- Standing lateral radiographs are considered the most reliable and standard test for diagnosing degenerative spondylolisthesis. 7 Akkawi I, Zmerly H. Degenerative Spondylolisthesis: A Narrative Review. Acta Biomed. 2022;92(6):e2021313. Published 2022 Jan 19. doi: 10.23750/abm.v92i6.10526
- Flexion-extension radiographs are used to determine if there is any motion of one vertebra upon the other (translation) and/or instability during spinal movements. 7 Akkawi I, Zmerly H. Degenerative Spondylolisthesis: A Narrative Review. Acta Biomed. 2022;92(6):e2021313. Published 2022 Jan 19. doi: 10.23750/abm.v92i6.10526
- Magnetic resonance imaging (MRI) scans may be used to check for spinal stenosis, nerve root compression, spinal cord involvement, and disc degeneration. 3 García-Ramos CL, Valenzuela-González J, Baeza-Álvarez VB, Rosales-Olivarez LM, Alpizar-Aguirre A, Reyes-Sánchez A. Degenerative spondylolisthesis I: general principles. Espondilolistesis degenerativa lumbar I: principios generales. Acta Ortop Mex. 2020;34(5):324-328.. , 7 Akkawi I, Zmerly H. Degenerative Spondylolisthesis: A Narrative Review. Acta Biomed. 2022;92(6):e2021313. Published 2022 Jan 19. doi: 10.23750/abm.v92i6.10526 Some researchers consider MRI scans as the most reliable test to diagnose spinal stenosis in degenerative lumbar spondylolisthesis. 8 Matz PG, Meagher RJ, Lamer T, et al. North American Spine Society. Clinical Guidelines for Multidisciplinary Spine Care. Diagnosis and Treatment of Degenerative Lumbar Spondylolisthesis. 2nd ed.; 2016.
- CT scans are used if bone involvement such as spondylolysis or isthmic spondylolisthesis is suspected, as these scans provide detailed evaluation of bone integrity.
If an MRI is not possible, computed tomography (CT) scans with myelography may be used as an alternative test. 7 Akkawi I, Zmerly H. Degenerative Spondylolisthesis: A Narrative Review. Acta Biomed. 2022;92(6):e2021313. Published 2022 Jan 19. doi: 10.23750/abm.v92i6.10526 , 8 Matz PG, Meagher RJ, Lamer T, et al. North American Spine Society. Clinical Guidelines for Multidisciplinary Spine Care. Diagnosis and Treatment of Degenerative Lumbar Spondylolisthesis. 2nd ed.; 2016.
MRI scans or CT scans may also be used if severe neurogenic claudication is present, bowel and/or bladder incontinence is reported, and/or tumors are suspected.
- 1 Cushnie D, Johnstone R, Urquhart JC, Gurr KR, Bailey SI, Bailey CS. Quality of Life and Slip Progression in Degenerative Spondylolisthesis Treated Nonoperatively. Spine (Phila Pa 1976). 2018;43(10):E574-E579. doi: 10.1097/BRS.0000000000002429
- 2 Li N, Scofield J, Mangham P, Cooper J, Sherman W, Kaye A. Spondylolisthesis. Orthop Rev (Pavia). 2022 Jul 27;14(4):36917. doi: 10.52965/001c.36917 . PMID: 35910544; PMCID: PMC9329062.
- 3 García-Ramos CL, Valenzuela-González J, Baeza-Álvarez VB, Rosales-Olivarez LM, Alpizar-Aguirre A, Reyes-Sánchez A. Degenerative spondylolisthesis I: general principles. Espondilolistesis degenerativa lumbar I: principios generales. Acta Ortop Mex. 2020;34(5):324-328..
- 4 Wang YXJ, Káplár Z, Deng M, Leung JCS. Lumbar degenerative spondylolisthesis epidemiology: A systematic review with a focus on gender-specific and age-specific prevalence. J Orthop Translat. 2016;11:39-52. Published 2016 Dec 1. doi: 10.1016/j.jot.2016.11.001
- 5 Kalichman L, Hunter DJ. Diagnosis and conservative management of degenerative lumbar spondylolisthesis. Eur Spine J. 2008;17(3):327-335. doi: 10.1007/s00586-007-0543-3
- 6 Studnicka K, Ampat G. Lumbosacral Spondylolisthesis. [Updated 2022 Sep 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560679/
- 7 Akkawi I, Zmerly H. Degenerative Spondylolisthesis: A Narrative Review. Acta Biomed. 2022;92(6):e2021313. Published 2022 Jan 19. doi: 10.23750/abm.v92i6.10526
- 8 Matz PG, Meagher RJ, Lamer T, et al. North American Spine Society. Clinical Guidelines for Multidisciplinary Spine Care. Diagnosis and Treatment of Degenerative Lumbar Spondylolisthesis. 2nd ed.; 2016.
Dr. Marco Funiciello is a physiatrist with Princeton Spine and Joint Center. He has a decade of clinical experience caring for spine and muscle conditions with non-surgical treatments.
- Degenerative Spondylolisthesis Symptoms "> Share on Facebook
- Degenerative Spondylolisthesis Symptoms "> Share on Pinterest
- Degenerative Spondylolisthesis Symptoms "> Share on X
- Subscribe to our newsletter
- Print this article
- Degenerative Spondylolisthesis Symptoms &body=https://www.spine-health.com/conditions/spondylolisthesis/degenerative-spondylolisthesis-symptoms&subject= Degenerative Spondylolisthesis Symptoms "> Email this article
Editor’s Top Picks
Spondylolysis and Spondylolisthesis
Leg Pain and Numbness: What Might These Symptoms Mean?
Sciatica Symptoms
Lumbar Radiculopathy
Isthmic Spondylolisthesis Symptoms
Popular Videos

Sciatica Causes and Symptoms Video

Cervical Disc Replacement Surgery Video

Lower Back Strain Video

3 Gentle Stretches to Prevent Neck Pain Video
Health Information (Sponsored)
- Take the Chronic Pain Quiz
- Suffering from Lumbar Spinal Stenosis? Obtain Long Term Pain Relief
- Relieve Your Chronic Low Back Pain with the Intracept™ Procedure
- Spondylolisthesis
Spondylolisthesis is a Latin term meaning slipped vertebral body (spinal bone).
“Spondylo”= vertebrae “listhesis”=slippage
Spondylolisthesis in the lumbar spine is most commonly caused by degenerative spinal disease (degenerative spondylolisthesis), or a defect in one region of a vertebra (isthmic spondylolisthesis).
ON THIS PAGE
- What are the types of spondylolisthesis?
- Which type is most common?
WHAT ARE THE TYPES OF SPONDYLOLISTHESIS?
Spondylolisthesis can be classified by into five groups (newman (1976)):.
- Group 1: dysplastic
- Group 2: isthmic
- Group 3: traumatic
- Group 4: degenerative
- Group 5: pathological
WHICH TYPE IS MOST COMMON?
Degenerative spondylolisthesis is very common, and occurs as a result of due to degeneration or wear and tear of the intervertebral discs and ligaments. Osteoarthritis of the facet joints can also play an important role in the development of instability and slippage. Degenerative spondylolisthesis usually occurs in people over 60 years of age.
In degenerative spondylolisthesis, what usually happens is that ongoing degeneration weakens the facet joints and disc, and (typically) the L4 vertebral body slips forward on the L5 vertebral body. Under normal circumstances, the L4-L5 segment is the one in the lumbar spine with the most movement. It is therefore most likely to slip when this process occurs. The next most common levels affected by degenerative spondylolisthesis are L3-L4 and L5-S1.
Isthmic spondylolisthesis occurs most often at L5-S1, and is more often seen in younger adults than degenerative spondylolisthesis. The cause is a defect in an important bridge bone (the pars interarticularis) of L5.
HOW IS SPONDYLOLISTHESIS GRADED?
Spondylolisthesis is graded according to the severity of the slippage. This is known as the Mayerding classification:
- Grade 1: <25% slip
- Grade 2: 25-50% slip
- Grade 3 50-75% slip
- Grade 4: 75-100% slip
When one vertebra slips entirely off the one below (>100% slip), this is known as spondyloptosis (see picture).
Spondylolisthesis doesn’t usually have any symptoms. In fact, it is commonly seen on X-rays and CT scans as an ‘incidental’ finding. It may, however, produce significant symptoms and disability.
Back pain is the most common symptom of spondylolisthesis. This pain is typically worse with activities such as bending and lifting, and often eases when lying down.
As the spine attempts to stabilise the unstable segment, the facet joints enlarge and place pressure on the nerve root causing lumbar spinal stenosis and lateral recess stenosis.
As one bone slips forward on the other, a narrowing of the intervertebral foramen may also occur (foraminal stenosis). Severe nerve compression can therefore occur with pain, numbness and weakness in the legs. Sometimes loss of control of the bladder and/or bowels can occur due to pressure on the nerves going to these important structures.
Imaging studies including MRI and CT can show a slip, as well as narrowing (stenosis) or compressed nerves in the spinal canal.
The CT and MRI scans are usually obtained with the patient lying flat, however sometimes a slip may only be obvious when standing or bending forwards. This is why your neurosurgeon or spinal surgeon will sometimes obtain flexion, extension and standing X-rays, and occasionally a CT myelogram.
Treatment for spondylolisthesis is similar to treatments for other causes of mechanical and compressive back pain. It is usually non-operative, and surgery is only necessary in a small percentage of patients.
MODIFIED ACTIVITIES
Your specialist may suggest that you modify some of your usual physical activities, this will help to help settle symptoms from mechanical back pain. Special braces are occasionally prescribed to ease back pain. Short periods of bed rest can sometimes help with very painful episodes.
PHYSICAL REHABILITATION
A comprehensive physical rehabilitation program can assist in settling pain and inflammation, as well as improving mobility and strength. A combination of physiotherapy, hydrotherapy and clinical Pilates typically works well and is often recommended. The aims of these physical therapies are to assist you in:
- managing your condition and controlling your symptoms
- correcting your posture and body movements to reduce back strain
- improving your flexibility and core strength
Some patients also benefit from chiropractic treatment osteopathy, remedial massage, and acupuncture.
PSYCHOLOGIST REVIEW
Having a review by a clinical psychologist can be helpful in for creating strategies to manage pain. It is also important to address any associated feelings of depression or anxiety, as these conditions can heighten your experience of pain.
MEDICATIONS
Medication often plays an important role in controlling pain and easing muscle spasms. It can also help you to get back to a normal sleep pattern. Long-term medication usage should be closely supervised as problems such as tolerance and dependence (addiction) are known to occur.
Surgery is only needed only if other non-surgical treatments are not keeping your pain at a manageable level. Surgical treatment for spondylolisthesis need to take into account both mechanical (instability) and compressive (nerve pressure) issues. Nerve pressure usually involves surgical decompression, also known as a decompressive laminectomy. In order to deal with the compressive issues by taking pressure off the nerves, your surgeon may need to remove some or all of one or both facet joints, as well as portions of the lamina.
As the facet joints typically provide stability to the lumbar spine, the spine can spine to become loose and unstable, especially after some slippage has already occurred. A fusion is usually therefore recommended.
Similarly, a fusion is necessary to adequately deal with the mechanical issues of instability in spondylolisthesis.
Six types of fusion surgery are commonly recommended for the treatment of spondylolisthesis, depending upon individual patient factors:
- Transforaminal lumbar interbody fusion (TLIF)
- Posterior lumbar interbody fusion (PLIF)
- Instrumented posterolateral fusion (pedicle screw fixation and posterolateral bone graft)
- Anterior lumbar interbody fusion (carried out through the abdomen, rather than from the back)
- Extracavitatory lateral interbody fusion (XLIF)
- Oblique lateral interbody fusion (OLIF)
Healthcare Services
- Anatomy of the Spine
- Brachialgia (Cervical Radiculopathy)
- Cervical Spinal Stenosis
- Degenerative Disc Disease
- Herniated Disk
- Facet Joint Pain
- Failed Back Surgery
- Lower Back Pain
- Lumbar Spinal Stenosis
- Spinal Tumours
- Trauma (fractures, dislocations, instability)
pain management center
Spondylolisthesis
- Medical Author: William C. Shiel Jr., MD, FACP, FACR
- Medical Editor: Catherine Burt Driver, MD
Spondylolisthesis Facts
What is spondylolisthesis, what are the types of spondylolisthesis, what causes spondylolisthesis, what are spondylolisthesis symptoms and signs, how do doctors diagnose and grade spondylolisthesis, what are treatments and home remedies for spondylolisthesis, what is the prognosis for spondylolisthesis, is it possible to prevent spondylolisthesis.
- Doctor's Notes on Spondylolisthesis Symptoms

- Slippage of one spinal vertebra over another is spondylolisthesis .
- Spondylolisthesis occurs in different grades and can be either congenital or acquired.
- Spondylolisthesis can cause symptoms by irritation of nervous tissue, either within the nearby spinal cord or of the adjacent spinal nerves.
- Radiology imaging is used to confirm the diagnosis of spondylolisthesis.
- Treatments of spondylolisthesis depend on the severity and persistence of symptoms.
Spondylolisthesis is slippage of one spinal vertebra over another. This most commonly occurs in the lower back in the lumbar spine.
Spondylolisthesis occurs in different degrees based on the amount of slippage of one vertebra on another. These degrees of slippage are medically termed grades . Accordingly, grade I is 0%-25%, grade II is 25%-50%, grade III is 50%-75%, grade IV is 75%-100%, and grade V is >100%. See the below table.
| Grades | Degrees of Slippage |
|---|---|
| grade I | 0%-25% |
| grade II | 25%-50% |
| Grade III | 50%-75% |
| Grade IV | 75%-100% |
| Grade V | >100% |
Spondylolisthesis can also be classified as congenital (present at birth) as a result of inherited factors or acquired as a result of injury or degeneration.
In children, spondylolisthesis is often related to a defect in, or injury to, a portion of the lumbar vertebra that connects to the spinous process (called the pars interarticularis). Medical professionals refer to the "disconnection" of this bone (pars defect) as spondylolysis and leads to slippage of the entire body of the vertebra, or spondylolisthesis.
In adults, spondylolysis can be degenerative and lead to spondylolisthesis. Degeneration of the cervical or lumbar disc can cause spondylolisthesis in adults. This, too, can lead to spondylolisthesis of the vertebrae above and below the worn out disc.
Spondylolisthesis commonly causes no symptoms or signs. When spondylolisthesis causes symptoms, they are typically a result of irritation of nervous tissue, either within the nearby spinal cord or of the adjacent spinal nerves. Such symptoms include low back pain , as well as pain, numbness, tingling, and weakness of one or both lower extremities. This can lead to leg pain , difficulty walking , incontinence , insomnia , and inability to function. Spondylolisthesis can lead to spinal stenosis with pain in the extremities with movement.
Spondylolisthesis is diagnosed by the history of chronic pain , numbness, tingling, and weakness of the extremities. Physicians confirm and visualize it with X-ray imaging. Health care professionals can also visualize it with CAT scan or MRI scan imaging.
Treatments of spondylolisthesis depend on the severity and persistence of symptoms. These include heat, analgesics, physical therapy exercises, braces , cortisone (steroid) injections, and orthopedic surgery procedures.
Home remedies include heat and/or ice applications, rest, avoiding reinjury, lumbar exercises, and acetaminophen (Tylenol), ibuprofen (Motrin, Advil), or naproxen (Aleve).
The prognosis for spondylolisthesis depends on the cause, severity, and overall condition of the patient involved. Most spondylolisthesis can respond to conservative treatments. Patients with persisting symptoms, or with severe traumatic spondylolisthesis, may require surgery.
The only prevention for spondylolisthesis is to prevent spinal injury.
Back Pain Resources
- WebMD Health Resources
Featured Centers
- What Are the Best PsA Treatments for You?
- Understanding Biologics
- 10 Things People With Depression Wish You Knew
More than 90% of all orthopedic conditions are treated without surgery. Let New York Bone & Joint Specialists heal and preserve your joints.
Spondylolisthesis: Symptoms, Treatment, & Surgery
What is spondylolisthesis.
Spondylolisthesis is the displacement or dislocation of a vertebra. It most commonly occurs in the lower back, but it can affect any region of the spinal column. In most cases, the affected vertebra protrudes forward over the vertebra directly beneath it, impinging or compressing the nerves in the back.
Spondylolisthesis Symptoms
Common symptoms of spondylolisthesis include a sudden pain that radiates down the back or buttocks and becomes more severe when bending or twisting, a sense of weakness in the legs, and an inability to walk without significant pain. In particularly extreme cases, it can also lead to incontinence.
Spondylolisthesis Grading
Spondylolisthesis can be categorized by the extent of the displacement in relation to the length of the vertebra. If 30% of a vertebra hangs over the vertebra beneath it, for example, the displacement is a grade 2 case of spondylolisthesis.
Grade 1 Spondylolisthesis
In Grade 1 spondylolisthesis, 0% to 25% of the vertebra hangs over the vertebra beneath it.
Grade 2 Spondylolisthesis
In Grade 1 spondylolisthesis, 25% to 50% of the vertebra hangs over the vertebra beneath it.
Grade 3 Spondylolisthesis
In Grade 1 spondylolisthesis, 50% to 75% of the vertebra hangs over the vertebra beneath it.
Grade 4 Spondylolisthesis
In Grade 1 spondylolisthesis, 75% to 100% of the vertebra hangs over the vertebra beneath it.
Grade 5 Spondylolisthesis
In Grade 1 spondylolisthesis, the entire vertebra hangs over the vertebra beneath it.
Spondylolisthesis Treatment
Treatments for spondylolisthesis depend on the severity of the condition, but most cases respond well to more conservative measures. Indeed, surgery is generally necessary only if the displacement has significantly limited the patient’s ability to function.
Conservative
The first line of treatment for spondylolisthesis is to simply refrain from any activity that might have caused the displacement or could exacerbate it. Minor to moderate pain can be effectively relieved with ibuprofen or acetaminophen. Corticosteroid injections can also alleviate pain and swelling. These treatments should be complemented with a physical therapy program, specifically flexion exercises, which are designed to rebuild the muscles in the core and back while restoring function to the affected vertebra.
Spondylolisthesis Surgery
Should the condition result in damage to the nerves or surrounding vertebrae, spondylolisthesis can also be treated with surgery. During this procedure, your surgeon will remove any bone or tissue that might be compressing the nerves and fuse the vertebrae together to prevent further displacement. This surgery can be performed openly or arthroscopically, and complete recovery can be expected after several months of rest and physical therapy.
Doctors Seeing Patients for Spine Conditions:

You can book your appointment with New York Bone & Joint online by submitting the appointment request form here:
Prefer to speak to someone right away, our locations.

1198 3rd Ave

130 E 67th St

Upper East Side Physical Therapy
Spondylolisthesis

Spondylolisthesis is a back injury which affects children between the ages of 9 and 14. It involves one vertebra in the spine slipping forward over another. Here we explain the symptoms, causes, and treatment of Spondylolisthesis.
Symptoms of Spondylolisthesis
Spondylolisthesis symptoms are categorized into grades 1 to 4 depending on severity.
- With grade 1 Spondylolisthesis there may be no symptoms at all and patients may be totally unaware they have a defect in the spine.
- Grade 2 Spondylolisthesis symptoms may include lower back pain, which may, or may not radiate into the legs.
- Pain is worse with activities which involve bending backwards of the spine.
- It may be possible to feel a dip in the spine at the point where the vertebrae slip forwards.
- An X-ray in a position that triggers the pain can confirm the diagnosis.
What is Spondylolisthesis?

Spondylolisthesis is a back injury involving a forward slipping of one vertebra over another and is most commonly seen in children between the ages of 9 and 14. It is also more common in sports that have a lot of strain on the back, for example, throwing events, wrestling, weight lifting, and gymnastics. The risk of slipping forward in people over the age of twenty-five is very small. It is usually the fifth or bottom lumbar vertebrae (L5) which slip forward over the top sacrum bone (S1).
It is often seen in conjunction with a stress fracture of the pars interarticularis ( Spondylolysis ). Most cases of pars interarticularis defects associated with spondylolysis are those where there is a family history of the defect. Stress fractures of the pars interarticularis through overuse are rarely thought to cause spondylolisthesis.
Spondylolisthesis is graded depending on how far forward the vertebra has slipped. It is measured by X-ray from the side and graded as follows:
- 1 – 25% forward movement
- 2 – greater than 25% forward movement.
- 3 – greater than 50% forward movement.
- 4 – greater than 75% forward movement.
Treatment of Spondylolisthesis
What can the athlete do.
- Rest from activities which cause or make the pain worse.
- The athlete may be able to continue training but avoid exercises that stress the back.
- Stretch the hamstring muscles as tight hamstring muscles may rotate the pelvis backwards in relation to the forward slipping vertebra.
- Do abdominal and core strengthening exercises.
- Wear a back brace or back support to prevent the lower spine from bending forward too much (anti-lordotic).
- See a sports injury specialist or doctor.

Cold Therapy Wraps
UPMedical.co.uk (UK)
Amazon.com (USA)
What can a sports injury specialist or doctor do?
- Prescribe strengthening exercises.
- Gently mobilize stiff joints in the spine around the forward slipping joint (but manipulation should not be done at the joint itself).
- Operate if another treatment is not successful.
When can I return to sports?
- Grade 1 and 2 patients can return as soon as they are pain-free and have good core strength.
- Grade 3 and 4 patients should avoid contact sports or sports involving high speed and changes of direction.
Spondylolisthesis does not usually get worse, but if the amount of slipping increases then a surgeon may operate to fuse the bones together preventing further forward slipping.
References & further reading
- Andrade N, Ashton C, Wray N et al. Systematic review of observational studies reveals no association between low back pain and lumbar spondylolysis with or without isthmic spondylolisthesis. Eur Spine J 2015;24:1289–95 .
About The Author
Mike walden, related articles.

Achilles Tendonitis & Tendinopathy
Achilles tendontis is an overuse injury causing pain at the back of the ankle. If not caught early, it can be a difficult injury to…
Read More »

Adductor Tendonitis
Groin inflammation or adductor tendonitis occurs when the tendons of the adductor muscles become inflamed causing pain, specifically high in the groin where the muscles…

Sprained Wrist
A sprained wrist is an injury to any of the ligaments which connect bone to bone in the wrist. Wrist sprains are common in sports.…

Immediate First Aid for Thigh Injuries
The PRICE principles are the gold standard set for treating sports injuries. The acronym stands for Protection, Rest, Ice, Compression, and Elevation and should be…

A TFCC tear is an injury to the triangular fibrocartilage complex found in the wrist. Either sudden trauma or overuse causes it. Here we explain…

Achilles Tendonitis Exercises
Achilles tendonitis heel drop exercises have proven to be successful for treating chronic Achilles tendon pain. The Hakan Alfredson’s heel drop protocol involves twice daily…

Gastrocnemius Tendonitis
Gastrocnemius tendonitis is inflammation of the gastrocnemius tendon at the back of the knee. It is most likely an overuse injury, more common in runners…

Calf Strain
A calf strain is a tear of one or more of the muscles at the back of the lower leg. They range from very mild…
Privacy Overview
Insert/edit link.
Enter the destination URL
Or link to existing content
- 086558 85566
- Request Appointment --> Request Appointment
Request Appointment
Enter your details and we will be in touch with you shortly; Or call 08655885566 between 8 am and 8 pm.
QI Spine Blog
- Everyday Tips
- Success Stories

Spondylolisthesis L5-S1: Symptoms, Causes & Treatment
Qi spine clinic, 4 years ago, what do you mean by spondylolisthesis l5-s1, difference between spondylolysis & spondylolisthesis, overview of l5-s1, spondylolisthesis – types & grades, signs & symptoms of spondylolisthesis l5-s1, other common symptoms are: –.
- Lower back pain is the most common one.
- Weakness in one or both thighs/legs
- Pain might radiate to buttocks or thighs
- Decreased ability to control bowel/bladder movements (in type IV and above)
- The muscles in the back of thigh i.e. hamstrings feel tight
- Difficulty in standing, walking.
Causes of Spondylolisthesis L5-S1
- Birth defect
- Followed by trauma
Other common problems at L5-S1 are as follows: –
- Spondylolysis
- Disc herniation
- Facet joint arthropathy
- Nerve compression
Diagnosing L5-S1 Spondylolisthesis
Treatment for spondylolisthesis l5-s1, the non-surgical treatment methods include:-, pain management.
- Rest – Take relative rest. Taking a break from all the strenuous activities can help in relieving the pain but it won’t reverse the condition.
- Medication – You can ease your pain with the help of OTC medicines.
- Injections – You might be suggested to get steroid medications/injections directly into the affected area.
- Physical Therapy – Specific exercises can help you in strengthening your abdomen and back. Frequency specific microcurrent and certain exercises can relieve pain.
To stabilize the spine for a long term effect
- Spine rehab & accurate treatment by targeting specific muscle – This can be achieved by exercise plan focusing on the weaker muscles around abdomen and back. Regular exercise can relieve pain.
- Brace – A brace can help in stabilizing your spine. It limits movement so that fractures can heal.
Spondylolisthesis L5-S1 Exercises
Below are the exercises that may help in decreasing the pain..
- Pelvic tilt – It strengthens your lower abdominal muscles and also stretches your lower back.
- Lower trunk rotation – It increases the mobility and flexibility of your spine.
- Partial curl
- Pelvic bridging
Frequently Asked Questions about L5-S1 Spondylolisthesis
What do you mean by l5-s1, what is the best exercise for l5-s1 spondylolisthesis, what does spondylolisthesis mean, what are the common symptoms of l5-s1 spondylolisthesis.
- Pain in the lower back and/or associated leg pain
- Pain, numbness, weakness or tingling in legs or feet
- Pain that gets worse with activity
- Change in posture and gait caused by hamstring tightness
- Intermittent shooting pain that passes from buttocks down to legs
What are the different grades of spondylolisthesis?
What is the objective of l5-s1 spondylolisthesis treatment, what are the necessary diagnostic tests to be done for l5-s1 spondylolisthesis, what are the main causes of l5-s1 spondylolisthesis, what are the other problems that may occur at l5-s1.
Visit our nearest clinic for your first consultation
Recommended Articles

Have You Been Recommended Back Surgery?
Past admins, 6 years ago.

Disc Degenerative L4-L5: Causes And Treatment
Qi spine clinic, 3 years ago.

Managing pain and mobility with sacroiliac joint d...
Qi spine clinic, 12 months ago.
We will notify you when our specialist answer your question.
Leave us your details
We will notify you when your question is answered
Our doctors usually respond within 24 hours
Enter your details and we will be in touch with you shortly Or call 086558 85566 between 8 am and 8 pm
We will be in touch with you shortly. Our clinic working hours are 8AM to 8PM.

Modal Header

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
The PMC website is updating on October 15, 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- PMC11392987
Minimally invasive versus mini-open transforaminal lumbar interbody fusion in managing low-grade degenerative spondylolisthesis
Elsayed mohamed selim ali.
Orthopedic Department, Faculty of Medicine, Zagazig University Hospital, Zagazig, Egypt
Mohamed Abdeen
Mohammed khalid saleh, associated data.
No datasets were generated or analysed during the current study.
Data background
Because the traditional open-TLIF approach has several drawbacks, minimally invasive surgery (MIS) approaches for TLIF (MISTLIF) have been developed to speed up recovery after surgery and minimize pressure on the para-spinal muscles, necessitating a cost-utility analysis for comparison in healthcare reforms.
Objectives and aim of the work
This study aimed to compare the radiological and clinical parameters between mini-open TLIF and minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) surgery in patients with single-level lumbar degenerative spondylolisthesis.
This study hypothesizes that both minimally invasive and mini-open methods using sublaminar trimming laminoplasty (SLTL) (while preserving midline structures) and interbody cages have comparable mid- and long-term clinical and radiological outcomes.
Retrospective analyses were performed on 120 patients who underwent single-level TLIF procedures with a minimum of two years of follow-up utilizing either the mini-open (n = 60) or MIS (n = 60) technique. Records of the operation's time frame, intraoperative fluoroscopy, blood loss, postoperative drainage volume, duration of bed rest, and complications were recorded. The Oswestry Disability Index (ODI) and visual analog scale (VAS) scores for both groups were utilized to assess improvements in clinical scores, and t tests were employed to statistically compare the outcomes. For comparison, radiological parameters, including lumbar lordosis, pelvic incidence (PI), and localized lordosis at the index level, were measured preoperatively, postoperatively, and at the final follow-up. To assess postoperative interbody fusion, the Bridwell grading system was used.
In the Mini-open TLIF group, the average follow-up time was 24.91 ± 5.7 months, while in the MIS-TLIF group, the average follow-up time was 25.15 ± 4.2 months. In the MIS-TLIF group, the mean operation and radiological time were longer. However, compared to the Mini-open TLIF group, the MISTLIF group experienced less blood loss and a shorter hospital stay. The MIS-TLIF group outperformed the Open-TLIF group in terms of the VAS score for back pain and the ODI at less than 6 months following surgery, and the differences were statistically significant. However, at the final follow-up, there were no statistically significant differences in the VAS score for the back between the two groups, but the ODI score was significantly greater in the MIS-TLIF group. Both groups' lumbar lordosis and focal lordosis significantly improved at the index level, with the Mini-open-TLIF group showing more focal lordosis. The interbody fusion rate did not significantly differ between the two groups.
MIS-TLIF and mini-open-TLIF can be surgically effective in treating single-level degenerative lumbar spine spondylolisthesis.
Introduction
Patients with degenerative spondylolisthesis of the lumbar spine usually present with radicular leg pain or neurogenic claudication, with or without low back pain. Whenever conservative management fails, patients are offered surgery. In the case of stable spondylolisthesis documented on dynamic radiographs, patients can be treated with decompression alone, and the modest difference in favor of additional instrumentation does not justify the associated higher costs for implants and longer duration of surgery [ 5 ]. Most patients with unstable spondylolisthesis are treated with nerve root decompression in addition to pedicle screw fixation and interbody fusion.
Minimally invasive spine surgery (MISS) is becoming increasingly popular worldwide. The rationale behind minimally invasive techniques is less tissue damage, reduced back pain leading to a shorter rehabilitation period, and faster return to work and resumption of daily activities [ 1 , 11 ].
In 2014, Wulu et al. described his new sublaminar trimming laminoplasty technique. This technique comprises aspects of laminotomy and laminectomy. It is proposed to remove tissue around the thecal sac and nerve root to widen the spinal canal while preserving structures that stabilize the spine, such as the facet joint, interspinous ligament, and supraspinous ligament [ 12 ]. In this study, we used this technique for mini-open access for interbody fusion to benefit both decompression and interbody fusion together with posterior and posterolateral fusion while preserving midline structures.
Patients and methods
The primary outcomes will be the VAS score for leg pain and back pain, and the 2nd outcome will be the ODI score, return to work, blood loss, blood transfusion, length of hospital stay, incidence of reoperation, and documentation of fusion. A retrospective study was performed using the medical records of our University Hospital for patients suffering from single-level lumbar low-grade degenerative spondylolisthesis who underwent surgical intervention with minimally invasive surgery (group 1, sixty patients) or mini-open surgery (group 2, sixty patients). Patients younger than 18 years, patients diagnosed with lytic and/or high-grade spondylolisthesis, patients who presented with infection, tumors, trauma, multiple levels of degenerative spondylolisthesis, and morbid obesity with a body mass index (BMI) greater than 40 were excluded.
On CT slices taken every six months until fusion, the modified Bridwell criteria for fusion of the lumbar spine were used. A sufficient fusion rate was determined using both grades I and II.
Surgical techniques
Minimally invasive interbody fusion with percutaneous pedicle screw insertion.
MIS‑TLIF procedure. After successful general anesthesia, the patient was placed in a prone position with chest and hip pads to avoid abdominal compression. Before the operation, a C-arm machine was used to fluoroscopically locate the surgical segment and mark the pedicle. After routine disinfection and towel laying, we made a bilateral longitudinal incision of approximately 2.5 cm at the marked position (Wiltse approach) and cut the skin, subcutaneous tissue and deep fascia in sequence. The four guide wires for the percutaneous pedicular screws were inserted before decompression was performed, and then the muscles were bluntly separated using tubular dilators to reach our docking site at the facet joint until insertion of the working channel. After fluoroscopy, the operation segment was correct, part or all of the upper and lower articular processes were removed according to the patient’s symptoms and spinal canal anatomy, and part of the lamina was removed to enlarge the spinal canal.
We decompressed the dural sac, the traversing nerve roots and the exiting nerve roots. The nucleus pulposus was removed from the degenerated nucleus, the endplate cartilage was scraped off, and the autogenous bone and BMP were implanted and beaten tightly. After a successful mold trial, a suitable PEEK cage was placed into the center of the intervertebral space through the Kambin triangle area. Percutaneous pediclular screws were placed over the guide wires previously inserted, the rods were inserted manually, and final tightening was performed after reduction of the spondylolisthesis (Fig. 1 and and2 2 ) .

MISTLIF case : (A-B) show antero-posterior and lateral radiology of the slipped level and (C-D) show the MRI photo of that level (sagittal and axial cut)

MISTLIF case : (A–B) show intraoperative fluoroscopic image antro-posterior and lateral view of the slipped level after insertion of the screws and rods, (C) show intraoperative photo of the wound, and ( D ) the tubular system in place, ( E ) C-Arm photo of the tubular system fixed on the facet (F-G) postoperative X-ray intro-posterior and lateral view of the slipped level and (H) shows the wound photo after closure of the wound
Mini-open sublaminar trimming laminoplasty with interbody cage insertion
In this technique, a posterior midline incision approximately 3 cm centered over the affected level is made. We preserved midline structures, including the spinous process and the inter-spinous ligament. The lower part of the laminae of the level above was removed together with the upper part of the laminae of the lower level to complete the foraminotomy with removal of the superior articulating process of the lower level. The ligamentum flavum was removed with a curved curette. The pedicular screws were inserted through the prepared holes together with the rods, and the screws were finally tightened. The interbody cage was inserted after the intervertebral disc was removed and the bed was prepared. Decortication of the posterior structures with insertion of the posterolateral graft (Fig. 3 and and4 4 ) .

Mini-open TLIF case: (A–B) antero-posterior and lateral radiology of the slipped level and (C-D) show the sagittal and axial cut of MRI photo of that level (E–F) postoperative X-ray intro-posterior and lateral view of the slipped level

Intraoperative photo of the Mini-open TLIF case with the spinous process in the midline and the lateral edge of the Dural sac seen bilateral (two white arrows) after performing the decompression and the blue arrow points the site of cage entry ( A ), ( B ) a pointer marking the window for cage entry
Statistical analysis
Data were coded, entered and analyzed using SPSS (Statistical Package for Social Science) version 25. Qualitative data were presented as frequencies and percentages while, quantitative data were presented as mean, standard deviations. Comparison of quantitative normally distributed data of two independent groups was done using Student t test, while comparison of quantitative dependent normally distributed data with repeated measures over different period of time was done using Repeated Measures ANOVA. Comparisons among qualitative variables was done using Chi Square test. P value (≤ 0.05) was considered statistically significant difference and P value < 0.001 was considered high statistically significant difference.
The MIS-TLIF group included 34 males and 26 females, with an average age of 40.4 ± 13.6 years. Of those, 45 had grade 1 degenerative spondylolisthesis, and 15 had grade 2 degenerative spondylolisthesis. In the Open-TLIF group, the average age of the 24 females and 36 males was 42.2 ± 13.7 years. Forty patients were categorized as grade 1, and twenty were categorized as grade 2. Age, sex, body mass index (BMI), slippage grade, surgical segment, and medical comorbidities did not significantly differ between the two groups ( Table 1 ). The mean follow-up period for the MIS-TLIF group was 25.15 ± 4.2 months, whereas that for the Open-TLIF group was 24.91 ± 5.7 months.
Table 1
Clinical characteristics of studied patients
| Group I (No. = 60) Mean ± SD | Group I (No. = 60) Mean ± SD | T test | .value | |||
|---|---|---|---|---|---|---|
| Age | 40.4 ± 13.6 | 42.2 ± 13.7 | − | 0.461 | ||
| No | % | No | % | X2 | .value | |
| Sex | ||||||
| Males | 34 | 56.7 | 34 | 60.0 | 0.137 | 0.711 |
| Females | 26 | 43.3 | 26 | 40.0 | ||
| Slip grade | ||||||
| Level 1 | 29 | 48.33 | 26 | 43.33 | ||
| Level 2 | 31 | 51.66 | 34 | 56.66 | ||
| Level | ||||||
| L4-5 | 50 | 83.33 | 48 | 80 | ||
| L3-4 | 10 | 16.66 | 12 | 20 | ||
| Follow-up period (months) | 25.15 ± 4.2 | 24.91 ± 5.7 | ||||
| Fusion (modified Bridwell) | ||||||
| Grade I | 40 | 66.66 | 35 | 58.33 | 0.5602 | |
| Grade II | 18 | 33.33 | 24 | 41.66 | ||
| Complications | ||||||
| Psudoarthrosis (n = 3) | 2 | 2.4 | 1 | 1.8 | 3.6 | 0.057 |
| Dural tear (n = 2) | 0 | 0.0 | 2 | 100.0 | 4.0 | 0.045* |
| Superficial wound infection (n = 2) | 0 | 0.0 | 2 | 100.0 | 4.0 | 0.045* |
| Hospital cost | 13,000$ | 12,500$ | 0.835 | |||
The MIS-TLIF group had significantly longer operation and intraoperative fluoroscopy times than did the Open-TLIF group ( Table 2 ). However, the MIS-TLIF group exhibited significantly less intraoperative blood loss, postoperative drainage volume, bed rest duration, and hospital stay than did the Open-TLIF group .
Table 2
Operative data
| Group I (No. = 60) Mean ± SD | Group I (No. = 60) Mean ± SD | T test | .value | |
|---|---|---|---|---|
| Operative time(min) | 134.8 ± 26.1 | 109.7 ± 12.8 | 6.676 | < 0.001** |
| Estimated blood loss (ml) | 256.3 ± 139 | 550.3 ± 186 | − 1.465 | 0.023* |
| Irradiation time(sec) | 84.4 ± 17.2 | 29.9 ± 5.4 | 23.47 | < 0.001** |
| hospital stay (day) | 3.2 ± 0.9 | 6.7 ± 1.6 | 14.999 | < 0.001** |
There were no statistically significant differences in the preoperative VAS score for both back and leg pain or in the ODI between the two groups ( Table 3 ). When comparing each group's postoperative VAS score for back and leg pain and ODI score to their preoperative values at any follow-up time point, substantial improvement was observed ( Tables Tables4 4 and and5 5 ). The MIS-TLIF group outperformed the Open-TLIF group in terms of the VAS score for back pain and the ODI at less than 6 months following surgery, and the differences were statistically significant. However, at the final follow-up, there were no statistically significant differences in the VAS score for the back between the two groups, but the ODI score was significantly greater in the MIS-TLIF group. Nevertheless, over the course of the follow-up period, the VAS score for leg pain in the mini-open-TLIF group remained better than that in the MIS-TLIF group ( Table 6 ).
Table 3
Comparison between studied groups regarding preoperative VAS back pain, ODI and VAS leg pain
| Group I (No. = 60) Mean ± SD | Group I (No. = 60) Mean ± SD | T test | .value | |
|---|---|---|---|---|
| Preoperative VAS back pain | 7.9 ± 0.8 | 8.1 ± 0.7 | − 1.229 | 0.222 |
| ODI preoperative | 48.7 ± 6.6 | 49.9 ± 6.8 | − 0.907 | 0.366 |
| VAS preoperative leg pain | 8.0 ± 0.9 | 7.7 ± 1.1 | 1.668 | 0.098 |
Table 4
Comparison of VAS back pain, ODI and VAS leg pain preoperative, one month, six month and 24 months among group I
| Group I preoperative | 1 month | 6 months | 24 months | F | .value | Partial Eta Squared | |
|---|---|---|---|---|---|---|---|
| VAS back pain | 7.9 ± 0.8†‡$ | 5.6 ± 0.5‡ #$ | 3.3 ± 0.5#†$ | 1.6 ± 0.5#†‡ | 1278.1 | < 0.001** | 0.96 |
| ODI | 48.7 ± 6.6 | 28.7 ± 4.9 | 21.5 ± 2.5 | 21.6 ± 2.3 | 500.262 | < 0.001** | 0.895 |
| VAS leg pain | 8.0 ± 0.9 | 4.2 ± 0.7 | 1.7 ± 0.6 | 1.6 ± 0.4 | 1130.241 | < 0.001** | 0.95 |
F Value of repeated measures ANOVA
Partial Eta Squared to detect effect size of intervention
# Significance with preoperative
† Significance with1 months postoperative
‡ Significance with 6 months postoperative
$ Significance with 24 months postoperative
Table 5
Comparison of VAS back pain, ODI and VAS leg pain preoperative, one month, six month and 24 months among group II
| Group I preoperative | 1 month | 6 months | 24 months | F | .value | Partial Eta Squared | |
|---|---|---|---|---|---|---|---|
| VAS back pain | 8.1 ± 0.7†‡$ | 6.6 ± 0.4‡ #$ | 3.5 ± 0.5#†$ | 1.7 ± 0.7#†‡ | 1515.9 | < 0.001** | 0.963 |
| ODI | 49.9 ± 6.8†‡$ | 28.6 ± 4.7‡ #$ | 24.3 ± 4.2#†$ | 22.7 ± 2.8#†‡ | 392.3 | < 0.001** | 0.869 |
| VAS leg pain | 7.7 ± 1.1†‡$ | 3.9 ± 0.8‡ #$ | 2.0 ± 0.6#†$ | 1.4 ± 0.4#†‡ | 755.8 | < 0.001** | 0.928 |
Table 6
Comparison between studied groups regarding post-operative VAS back pain, ODI and VAS leg pain
| Group I Mean ± SD | Group II Mean ± SD | T test | .value | ||
|---|---|---|---|---|---|
| VAS back pain | After 1 month | 5.6 ± 0.5 | 6.6 ± 0.4 | − 10.768 | < 0.001** |
| After 6 month | 3.3 ± 0.5 | 3.5 ± 0.5 | − 1.825 | 0.071 | |
| After 24 month | 1.6 ± 0.5 | 1.7 ± 0.7 | − 0.996 | 0.321 | |
| ODI | After 1 month | 21.4 ± 2.4 | 24.2 ± 4.4 | − 4.422 | < 0.001** |
| After 6 month | 21.5 ± 2.5 | 24.3 ± 4.2 | − 4.418 | < 0.001** | |
| After 24 month | 21.6 ± 2.3 | 22.7 ± 2.8 | − 2.499 | 0.014* | |
| VAS leg pain | After 1 month | 4.2 ± 0.7 | 3.9 ± 0.8 | 2.152 | 0.033* |
| After 6 month | 1.7 ± 0.6 | 2.0 ± 0.6 | − 2.206 | 0.029* | |
| After 24 month | 1.6 ± 0.4 | 1.4 ± 0.4 | 2.613 | 0.01* |
When comparing each group's vertebral slippage percentage to its preoperative rank, a statistically significant improvement was observed immediately following surgery until the most recent follow-up. Furthermore, at every follow-up time point, there was no statistically significant difference in the vertebral slip ratio between the MIS-TLIF group and the Open-TLIF group. In both groups, there was a statistically significant difference in the segmental lordosis of the slipping level and the lumbar lordosis between the pre- and postoperative periods. However, when comparing preoperation, immediately postoperatively, and segmental lordosis, no discernible changes were detected between the two groups. On the other hand, there was more segmental lumbar lordosis in the Open-TLIF group. The postoperative interbody fusion rate did not significantly differ between the two groups according to the Bridwell classification ( p < 0.05) (Table 7 ).
Table 7
Comparison between studied groups regarding radiological outcome
| MIS-TLIF | Mini-Open TLIF | |
|---|---|---|
| Vertebral slip % | ||
| Pre-operative | 24.23 ± 4.22 | 25.33 ± 5.33‡ |
| Post-operative | 8.67 ± 2.91* | 8.45 ± 2.55*‡ |
| Last follow up | 8.99 ± 2.3*† | 8.87 ± 2.1*†‡ |
| Lumbar lordosis | ||
| Pre-operative | 43.3 ± 7.9 | 42.1 ± 8.5‡ |
| Post-operative | 48.1 ± 8.2* | 48.7 ± 7.6*‡ |
| Last follow up | 47.2 ± 7.9*† | 48.5 ± 6.2*†‡ |
| Focal lordosis | ||
| Pre-operative | 5.4 ± 5.9 | 6.5 ± 4.3‡ |
| Post-operative | 8.9 ± 7.8* | 9.2 ± 5.1*‡ |
| Last follow up | 8.1 ± 6.7*† | 8.2 ± 4.9*†‡ |
Vertebral slip percentage, Lumbar lordosis and focal lordosis comparison between the two groups: * P < 0.05, comparing post-operative data in each group compared to preoperative data, † P > 0.05, comparing data at last follow-up versus immediately following surgery. ‡ P > 0.05, comparing the two groups'
There were two occurrences of superficial incision infection in the open-TLIF group and none in the MIS-TLIF group. Anti-infection medications and frequent dressing changes were used to treat both infections. Two incidences of intraoperative dural tears were recorded in the mini-open-TLIF group; these were immediately repaired, and there was no postoperative leakage of CSF. With two cases of nonunion, the MIS group had a greater rate of pseudoarthrosis. Patients, however, declined to have the procedure repeated.
Numerous published lumbar interbody fusion techniques have been developed with the goal of maintaining spinal alignment, boosting fusion rates, and reducing back and leg discomfort. To achieve smaller surgical wounds, less trauma to surrounding tissue, and a quicker recovery after surgery, Foley et al. introduced MIS-TLIF as an alternative to conventional open-TLIF in the early 2000s. However, similar long-term results for both MIS- and open-TLIF have been previously described in the literature. On the other hand, the positive impacts of MIS-TLIF might be evident in the early stages of recovery, with a shorter period of postoperative opioid use, a shorter hospital stay and an earlier return to work following surgery [ 15 ]. However, strong data are currently lacking on which technique is more clinically effective in treating symptomatic low-grade degenerative spondylolisthesis. This study aimed to compare and evaluate the safety and effectiveness of mini-open-TLIF and MIS-TLIF in the treatment of degenerative spondylolisthesis. To prevent bias, the same surgical team with extensive training in the MIS/mini Open-TLIF approach handled every patient in our study.
The paraspinal muscles sustain more damage when they are separated from their origin/insertion during the mini-open-TLIF. On the other hand, MIS-TLIF involves the use of the paraspinal approach, which aims to dilate the muscles to minimize muscular damage. This was observed in our study because the amount of blood loss was greater in the mini-open-TLIF group. Evaniew et al. [ 3 ] reported that patients who underwent MIS experienced reduced blood loss and quicker surgery. Similar to the findings of a previous study, Qin et al. [ 16 ] demonstrated that MIS-TLIFs reduce blood loss better than do mini-open TLIFs; nevertheless, the authors noted that the MIS-TLIF group needed more time during surgery. Similar outcomes to our investigation were observed in the previous trial, with the MIS group requiring more time during surgery and less blood loss. This could be attributed to the surgical and technique learning curve and familiarity with the approach with fewer bony landmarks and working in a narrow tube.
It is important to consider the cumulative effects of radiation exposure on both the patient and the surgical team [ 7 ]. The smaller operating field, difficulty in seeing bone landmarks, and challenging learning curve associated with MIS-TLIF all contribute to greater radiation exposure duration. According to our study, the prolonged fluoroscopy time needed for percutaneous pedicle screw implantation with MISTLIF accounts for the majority of the increased radiation exposure compared to that of mini-open-TLIF. The radiation exposure period could be shortened with more surgical experience and an improvement in the learning curve, as we noticed in the latter patients who underwent MIS-TLIF [ 14 ].
In the current economic environment, comparing the cost-effectiveness of MIS-TLIF versus mini-open-TLIF is crucial. In two papers published in 2012 and 2014, Parker et al. computed ICERs taking into account both direct and indirect costs; however, the results were inconsistent. A statistically significant difference in cost between the two procedures was not found by our study's cost comparison. However, MIS-TLIF implants were more costly than Open-TLIF implants. This may be explained by the fact that the open-TLIF group required a longer postoperative hospital stay (6.7 ± 1.6 days) together with the indirect cost of delayed return to work in comparison to 3.2 ± 0.9 days in the MIS group. Early hospital discharge minimizes exposure to nosocomial infections, promotes earlier and more frequent mobility, and decreases hospital expenses.
Both groups' back and leg pain VAS scores and ODI scores significantly improved following surgery compared to the preoperative values. This demonstrates that both approaches have proven successful in addressing those suffering from degenerative spondylolisthesis, as reported in the literature [ 1 , 7 , 16 ].
Furthermore, when treating degenerative lumbar illnesses, Heemserk et al. [ 8 ] demonstrated that MIS and open operations have comparable outcomes at two years of follow-up. Qin et al. [ 16 ] reported that when treating single-level low-grade spondylolisthesis, MIS-TLIF seems to be a more effective and safer approach and has a better long-term functional prognosis. The sole difference in the quality-of-life score between the two groups in our study was discovered during follow-up, as the MIS-TLIF group outperformed the Open-TLIF group during the first month in terms of the VAS score for back pain and during the first 6 months in terms of the ODI score for disability ( p < 0.001). The open-TLIF group, however, had a greater VAS score for leg pain relief ( p < 0.05) than did the MIS group. This suggests that although the two groups' clinical performance was similar over time, the MIS-TLIF group performed better than the Open-TLIF group only in terms of early reduction in low back pain and disability. However, Open-TLIF is better for neural tissue decompression because of the large exposure of the approach.
Currently, vertebral slip reduction in spondylolisthesis patients remains a controversial topic. Several studies have shown that satisfaction rates ranging from 75 to 80% can be achieved with in situ fusion without reducing slippage [ 4 , 13 ]. Conversely, other studies have reported a notable prevalence of sagittal imbalance, progressive slippage and pseudoarthrosis. Reducing degenerative spondylolisthesis will somewhat enhance the sagittal lumbosacral balance and the clinical outcome even if it is not required and provide areas for bony fusion [ 4 ]. In our study, both techniques showed significant changes in the slip degree, with no difference between the two techniques. The discrepancy in the reduction data may be limited to patients with high-grade spondylolisthesis, and all our patients had low-grade spondylolisthesis [ 1 ].
Higher grades of spondylolisthesis are characterized by a sagittal imbalance caused by slippage and lordosis loss (LL), which are correlated with disc degeneration. Pelvic retroversion, the result of the pelvis rotating, causes the sacral slope (SS) to decrease and the pelvic tilt (PT) to increase, which restricts the anterior translation of the axis of gravity. Therefore, the restoration of the normal PT range requires the restoration of lumbar lordosis [ 1 , 17 ]. Lower back discomfort can arise from relative kyphosis on the fused segment caused by a decrease in postoperative LL. This, in turn, increases the tensile stress on the spinal structures posterior to the fused segment, including the paraspinal muscles. Therefore, the restoration of segmental and total lordosis is essential for these patients.
Compared to MIS-TLIF, a few surgeons have theorized that open TLIF would allow for more segmental and global lordosis correction. After MIS-TLIF, Dibble et al. [ 2 ] observed greater improvements in segmental lordosis (SL). However, there were no variations in the global lordosis angle compared to that of the Open-TLIF group. On the other hand, the global lordosis angle did not vary. We discovered the same findings during our investigation, with no statistically significant difference in segmental or global lordosis between the two groups. On the other hand, LL and SL significantly changed between the preoperative and postoperative data.
The postoperative interbody fusion rate did not significantly differ between the two groups according to the Bridwell classification (p < 0.05). This finding implies that the fusion rate was unaffected by the surgical technique. In a 5-year follow-up investigation on the fusion findings of MIS-TLIF, Kim et al. [ 9 ], in a narrative review of 14 prospective observational studies and 6 randomized controlled trials, estimated a fusion rate of more than 90%. This is consistent with the results of our study. It could be concluded that for both mini-opening and MIS, the surgical fusion rate may produce good outcomes. However, a number of studies comparing the two methods of treatment have suggested that open-TLIF may provide superior interbody space preparation compared with MIS-TLIF and that MIS-TLIF may result in a lower fusion rate than open-TLIF [ 9 , 14 ]. Many other factors may contribute to this discrepancy, such as the type of graft used (either autograft or synthetic). Sufficient autografts were used in all patients in this study.
According to Goertz et al. [ 6 ] and Krüger M.T. et al. [ 10 ], obese patients who underwent MIS-TLF surgery had a greater incidence of dural tears. The use of TLIF through tube retractors placed directly over the facet avoids the need for retraction of the dura, which avoids the incidence of tears and the avoidance of dural tears during the insertion of the roods or the set esrew at the final step in Open-TLIF. The open-TLIF group experienced an intraoperative dural tear in two patients; however, the MIS-TLIF group experienced no such problems. The use of skin retractors resulted in two cases of skin edge necrosis in the Open-TLIF group, which were further worsened by superficial skin infections. Using a tubular retractor prevented complications in the MIS-TLIF group by preventing significant skin retraction and causing less tissue injury, which minimized the infection rate.
Limitations
There are several limitations to this study. First, the study was a single-center retrospective study and included only a small number of scenarios. Second, the duration of patient follow-up was somewhat brief. Third, the analysis included only patients who had single-level low-grade spondylolisthesis, and all of them had disc-level lesions at the L4-L5 and L5-S1 levels. More research is required on people with higher-level spondylolisthesis and multisegment disc degenerative diseases.
MIS-TLIF and mini-open-TLIF can be surgically effective in treating single-level degenerative lumbar spine spondylolisthesis in properly selected patients. More specifically, MIS-TLIF can significantly reduce bleeding and the length of hospital stay; nevertheless, MIS-TLIF is associated with increased radiological exposure.
Author contributions
Elsayed Mohamed Selim Ali: (Technique, handling of data, theory, structure, analysis, interpretation, publication search, and writing are all the author's responsibility.). Mohamed Abdeen: (theory, structure, and analysis of literature). Mohammed Khaled Saleh: (Responsible for idea, layout, evaluation, and interpretation).
Open access funding provided by The Science, Technology & Innovation Funding Authority (STDF) in cooperation with The Egyptian Knowledge Bank (EKB). This research was not given a particular grant from any public or private funding organizations.
Data availability
Declarations.
An ethical approval was done by the IRB, Informed consent was obtained from all individual participants included in the study. Patients signed informed consent regarding publishing their data and photographs.
This study was not presented at any congress or symposium.
All work done at Zagazig university hospitals.
The authors declare no competing interests.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
IMAGES
VIDEO
COMMENTS
Learn about the causes, symptoms and treatment options for spondylolisthesis, a condition where a vertebra slips forward over the one below. Grade 2 spondylolisthesis is the most common grade and can be treated with conservative methods or bracing.
Spondylolisthesis is a condition in which a vertebra slips out of place and puts pressure on a nerve. Learn about the types, grades, diagnosis, and treatment options for this spine problem.
Spondylolisthesis is a condition where one vertebra slips forward or backwards relative to the vertebra below. Spondylosis is a fracture of a small bone that connects the vertebrae, which may lead to spondylolisthesis. Learn about the types, grades, symptoms, and treatments of spondylolisthesis.
Spondylolisthesis is a condition where a vertebra slips forward and out of place in the spine. It can cause back and leg pain, nerve compression, and spinal stenosis. Learn about the causes, symptoms, diagnosis, and treatment of spondylolisthesis.
Spondylolisthesis is a condition where one vertebra slips forward over another, causing back pain and spinal deformity. Learn about the causes, stages, symptoms, and treatment options for spondylolisthesis, and how to prevent it from progressing.
Spondylolisthesis is a spinal condition that affects the lower vertebrae. It can cause lower back pain, stiffness, and nerve damage. Learn about the causes, diagnosis, and treatment options for ...
Learn about the causes, symptoms, and treatments of spondylolysis and spondylolisthesis, two common causes of low back pain in children and adolescents. Spondylolysis is a stress fracture in the vertebra, and spondylolisthesis is when the fractured vertebra slips forward.
Spondylolisthesis is a condition where one of the bones in your spine, called a vertebra, slips forward. It can cause lower back pain, sciatica, tight hamstrings and other symptoms. Learn about the causes, diagnosis and treatments of spondylolisthesis.
Spondylolisthesis is a condition where spinal vertebrae slip over one another, causing lower back pain and nerve injury in some cases. Learn about the types, causes, symptoms and treatments of spondylolisthesis, and when surgery may be necessary.
Spondylolisthesis is a condition where a vertebra slips out of place, causing back pain and nerve compression. Learn about the types, risk factors, diagnosis and treatment options, and the potential complications of spondylolisthesis if left untreated.
Spondylolisthesis is a condition in which a vertebra slips out of place, causing back pain, nerve damage and posture problems. Traumatic spondylolisthesis is caused by a fracture of the vertebrae due to injury. Learn about the symptoms, causes, diagnosis and treatment options.
Spondylolisthesis is the slippage of one vertebral body with respect to the adjacent vertebral body causing mechanical or radicular symptoms or pain. It can be due to congenital, acquired, or idiopathic causes. Spondylolisthesis is graded based on the degree of slippage of one vertebral body on the adjacent vertebral body.
Learn about spondylolisthesis, a forward slip of one vertebra over another, and its grades, causes, and symptoms. Grade 2 spondylolisthesis means 50% of a vertebral body has slipped forward over ...
Learn about degenerative spondylolisthesis, a condition where one vertebra slips forward over the one below, often affecting the L4-L5 spinal segment. Find out the causes, symptoms, treatment options and surgery for this spine disorder.
Degenerative spondylolisthesis is a condition that causes low back pain and leg symptoms due to spinal stenosis or nerve compression. It may affect bowel function, but this is not a common symptom and may depend on the severity and location of the slipped vertebra.
Spondylolisthesis is a condition where a vertebra slips forward on the one below, causing back pain and nerve compression. Learn about the causes, grades, and treatments of spondylolisthesis, including surgery for spondyloptosis (grade 5).
When spondylolisthesis causes symptoms, they are typically a result of irritation of nervous tissue, either within the nearby spinal cord or of the adjacent spinal nerves. Such symptoms include low back pain, as well as pain, numbness, tingling, and weakness of one or both lower extremities. This can lead to leg pain, difficulty walking ...
Spondylolisthesis Symptoms. Common symptoms of spondylolisthesis include a sudden pain that radiates down the back or buttocks and becomes more severe when bending or twisting, a sense of weakness in the legs, and an inability to walk without significant pain. ... Grade 4 Spondylolisthesis. In Grade 1 spondylolisthesis, 75% to 100% of the ...
Spondylolisthesis symptoms are categorized into grades 1 to 4 depending on severity. With grade 1 Spondylolisthesis there may be no symptoms at all and patients may be totally unaware they have a defect in the spine. Grade 2 Spondylolisthesis symptoms may include lower back pain, which may, or may not radiate into the legs.
Learn about spondylolisthesis, a condition where one vertebra slips over another, causing back pain and nerve compression. Find out the types, grades, diagnosis and treatment options for L5-S1 spondylolisthesis, a common site of slippage.
The MIS-TLIF group included 34 males and 26 females, with an average age of 40.4 ± 13.6 years. Of those, 45 had grade 1 degenerative spondylolisthesis, and 15 had grade 2 degenerative spondylolisthesis. In the Open-TLIF group, the average age of the 24 females and 36 males was 42.2 ± 13.7 years.