JavaScript seems to be disabled in your browser. For the best experience on our site, be sure to turn on Javascript in your browser.
- My Wish List
- Compare Products
- Presentations
You must be logged in to download this file*
item details (6 Editable Slides)
(6 Editable Slides)


Related Products

Vertigo refers to the spinning or movement sensation experienced by an individual when one is stationary and results from issues within the inner ear. Utilize our presentation template for MS PowerPoint and Google Slides to depict how this condition affects a person’s balance and spatial orientation and leads to dizziness, nausea, and even falls.
Otolaryngologists and neurologists can utilize this PPT to deliver a captivating presentation about the impact and consequences of vertigo on an individual's quality of life. You can illustrate the types, symptoms, and causes of vertigo. You can also represent the tests for diagnosing this condition and the treatment options to manage and cure it.
Sizing Charts
| Size | XS | S | S | M | M | L |
|---|---|---|---|---|---|---|
| EU | 32 | 34 | 36 | 38 | 40 | 42 |
| UK | 4 | 6 | 8 | 10 | 12 | 14 |
| US | 0 | 2 | 4 | 6 | 8 | 10 |
| Bust | 79.5cm / 31" | 82cm / 32" | 84.5cm / 33" | 89.5cm / 35" | 94.5cm / 37" | 99.5cm / 39" |
| Waist | 61.5cm / 24" | 64cm / 25" | 66.5cm / 26" | 71.5cm / 28" | 76.5cm / 30" | 81.5cm / 32" |
| Hip | 86.5cm / 34" | 89cm / 35" | 91.5cm / 36" | 96.5cm / 38" | 101.5cm / 40" | 106.5cm / 42" |
| Size | XS | S | M | L | XL | XXL |
|---|---|---|---|---|---|---|
| UK/US | 34 | 36 | 38 | 40 | 42 | 44 |
| Neck | 37cm / 14.5" | 38cm /15" | 39.5cm / 15.5" | 41cm / 16" | 42cm / 16.5" | 43cm / 17" |
| Chest | 86.5cm / 34" | 91.5cm / 36" | 96.5cm / 38" | 101.5cm / 40" | 106.5cm / 42" | 111.5cm / 44" |
| Waist | 71.5cm / 28" | 76.5cm / 30" | 81.5cm / 32" | 86.5cm / 34" | 91.5cm / 36" | 96.5cm / 38" |
| Seat | 90cm / 35.4" | 95cm / 37.4" | 100cm / 39.4" | 105cm / 41.3" | 110cm / 43.3" | 115cm / 45.3" |

- Theatre Etiquette
- Hand Washing
- Scrubbing, Gowning, and Gloving
- Assisting in Theatre
- The Operation Note
- Surgical Safety
- Suture Materials
- Surgical Instruments
- Infiltration of Local Anaesthetic
- Drain Insertion
- Abscess Drainage
- Skin Lesion Excision
- Damage to Local Structures
- Acute Inflammation
- Chronic Inflammation
- Wound Healing
- Basic Wound Management
- Venepuncture
- Cannulation
- Blood Cultures
- Intravenous Infusions
- Female Catheterisation
- Male Catheterisation
- Pre-Op Assessment
- Pre-Op Management
- Fluid Management
- Blood Products
- Perioperative Nutrition
- Enhanced Recovery
- Day Case Surgery
- Haemorrhage
- Nausea & Vomiting
- Atelectasis
- Fat Embolism
- Anastomotic Leak
- Post-Op Ileus
- Bowel Adhesions
- Incisional Hernia
- Constipation
- Acute Kidney Injury
- Urinary Retention
- Urinary Tract Infection
- Hypoglycaemia
- Hyperkalaemia
- Hypokalaemia
- Hypernatremia
- Hyponatraemia
- Surgical Site Infection
- Wound Dehiscence
- Initial Assessment
- The General Approach
- A-E Assessment
- Referring a Patient
- IV Fluid Management
- Post-Op Fever
- Post-Op Pain
- Cardiovascular
- Respiratory
- Cardiothoracic Incisions
- Digital Rectal
- Abdominal Incisions
- Peripheral Vascular
- Peripheral Venous
- Cranial Nerves
- Peripheral Neurological
- Diabetic Foot
- Thyroid Gland
- Foot & Ankle
- Oral Cavity
- Certifying Death
- Acute Abdomen
- Haematemesis
- Gastric Outlet Obstruction
- Bowel Obstruction
- Bowel Perforation
- Rectal Bleeding
- Oesophageal Cancer
- Oesophageal Tears
- Motility Disorders
- Hiatus Hernia
- Peptic Ulcer Disease
- Gastric Cancer
- Inguinal Hernia
- Femoral Hernia
- Abdominal Wall Hernia
- Gastroenteritis
- Angiodysplasia
- Small Bowel Tumours
- Neuroendocrine Tumours
- Meckel’s Diverticulum
- Acute Appendicitis
- Colorectal Cancer
- Diverticular Disease
- Crohn’s Disease
- Ulcerative Colitis
- Pseudo-Obstruction
- Haemorrhoids
- Pilonidal Sinus
- Fistula-in-Ano
- Anorectal Abscess
- Anal Fissure
- Rectal Prolapse
- Anal Cancer
- Colic & Cholecystitis
- Cholangitis
- Cholangiocarcinoma
- Hepatocellular Carcinoma
- Liver Cysts
- Liver Abscess
- Acute Pancreatitis
- Chronic Pancreatitis
- Pancreatic Cancer
- Cystic Neoplasms of the Pancreas
- Splenic Infarct
- Splenic Rupture
- Acutely Painful Limb
- Lower Limb Ulcers
- Carotid Artery Disease
- Abdominal Aortic Aneurysm
- Aortic Dissection
- Thoracic Aortic Aneurysm
- Acute Limb Ischaemia
- Chronic Limb Ischaemia
- Acute Mesenteric Ischaemia
- Chronic Mesenteric Ischaemia
- Pseudoaneurysm
- Peripheral & Visceral Aneurysms
- Varicose Veins
- Venous Insufficiency
- Thoracic Outlet Syndrome
- Subclavian Steal Syndrome
- Hyperhidrosis
- Scrotal Pain
- Acute Urinary Retention
- Chronic Urinary Retention
- Lower Urinary Tract Symptoms
- Scrotal Lumps
- Renal Tract Calculi
- Pyelonephritis
- Renal Cancer
- Renal Cysts
- Urinary Incontinence
- Bladder Cancer
- Benign Prostatic Hyperplasia
- Prostate Cancer
- Prostatitis
- Epididymitis
- Testicular Torsion
- Testicular Cancer
- Fournier’s Gangrene
- Paraphimosis
- Penile Fracture
- Penile Cancer
- Peyronie’s Disease
- Hypospadias
- Cryptorchidism
- Balanitis Xerotica Obliterans
- Osteoarthritis
- Fracture Management
- Acutely Swollen Joint
- Open Fracture
- Compartment Syndrome
- Septic Arthritis
- Osteomyelitis
- Bone Tumours
- Clavicle Fracture
- Rotator Cuff Tear
- Shoulder Fracture
- Shoulder Dislocation
- Humeral Shaft Fracture
- Biceps Tendinopathy
- Adhesive Capsulitis
- Subacromial Impingement Syndrome
- Supracondylar Fracture
- Olecranon Fracture
- Radial Head Fracture
- Elbow Dislocation
- Olecranon Bursitis
- Epicondylitis
- Distal Radius Fracture
- Scaphoid Fracture
- Carpal Tunnel Syndrome
- Dupuytren’s Contracture
- De Quervain’s Tenosynovitis
- Ganglionic Cysts
- Trigger Finger
- Radiculopathy
- Degenerative Disc Disease
- Cervical Fracture
- Thoracolumbar Fracture
- Neck of Femur Fracture
- Hip Osteoarthritis
- Femoral Shaft Fracture
- Quadriceps Tendon Rupture
- Distal Femur Fracture
- Pelvic Fracture
- Acetabular Fracture
- Knee Osteoarthritis
- Meniscal Tear
- Patella Fracture
- Tibial Shaft Fracture
- Tibial Plateau Fracture
- Iliotibial Band Syndrome
- Ankle Fracture
- Calcaneal Fracture
- Achilles Tendonitis
- Talar Fracture
- Tibial Pilon Fracture
- Lisfranc injury
- Hallux Valgus
- Plantar Fasciitis
- The Limping Child
- Growth Plate Fracture
- Triple Assessment
- Galactorrhoea
- Inflammatory Disease
- Benign Tumours
- Gynaecomastia
- Carcinoma in Situ
- Invasive Cancer
- Surgical Treatments
- Non-Surgical Treatments
- Hoarse Voice
- Facial Palsy
- Hearing Loss
- Otitis Externa
- Acute Otitis Media
- Otitis Media with Effusion
- Chronic Mucosal Otitis Media
- Chronic Squamous Otitis Media
- Acute Rhinosinusitis
- Chronic Rhinosinusitis
- Periorbital Cellulitis
- Nasal Trauma
- Obstructive Sleep Apnoea
- Tonsillitis
- Deep Neck Space Infections
- Foreign Bodies
- Sialolithiasis
- Sialadenitis
- Salivary Gland Tumours
- Thyroid Cancer
- Head & Neck Cancer
- Assessment of Head Injury
- Extradural Haematoma
- Subdural Haematoma
- Diffuse Axonal Injury
- Traumatic Spinal Cord Injury
- Monro-Kellie Doctrine
- Intracranial Pressure Monitoring
- Hydrocephalus
- Subarachnoid Haemorrhage
- Intracranial Aneurysms
- Intracerebral Haemorrhage
- Arteriovenous Malformation
- Intracranial Infections
- Pituitary Tumours
- Spinal Tumours
- Deep Brain Stimulation
- Epilepsy Surgery
- Cauda Equina Syndrome
- Spinal Cord Compression
- Spinal Infections
- Principles of Wound Management
- Burns Assessment
- Burns Reconstruction
- Skin Grafts and Flaps
- Basal Cell Carcinoma
- Squamous Cell Carcinoma
- Flexor Tendon Injuries
- Extensor Tendon Injuries
- Metacarpal Fractures
- Phalangeal Fractures
- Nail Bed Injuries
- Finger Replantation
- Skin Abscess
- Necrotising Fasciitis
- Bite Injuries
- Hand Infections
- Cardiopulmonary Bypass
- Bridge to Transplantation
- Foetal & Adult Circulation
- Coronary Artery Disease
- Valvular Disease
- Cardiac Tumours
- Lung Cancer
- Airway Disorders
- Chest Wall Disorders
- Mediastinal Tumours
- Diaphragmatic Hernia
- Pneumothorax
- Haemothorax
- Principles of Transplantation
- Concepts of Brain Death
- Organ Retrieval
- Immunosuppression in Transplantation
- Renal Transplantation
- Liver Transplantation
- Pancreas Transplantation
- Heart Transplantation
- Lung Transplantation
- I&D Abscess
- Diagnostic Laparoscopy
- Appendicectomy
- Small Bowel Resection
- Hartmann’s Procedure
- Gastroscopy
- Colonoscopy
- Excision of a Lump
- Open Inguinal Hernia Repair
- Laparoscopic Inguinal Hernia Repair
- Open Umbilical Hernia Repair
- Laparoscopic Cholecystectomy
- Nissen Fundoplication
- Oesophagectomy
- Gastric Band
- Gastric Bypass
- Sleeve Gastrectomy
- Lay Open Fistula
- Haemorrhoidectomy
- Pilonidal Sinus Repair
- Reversal of a Stoma
- Right Hemicolectomy
- Left Hemicolectomy
- Anterior Resection
- Abdominoperineal Resection
- Carotid Endarterectomy
- Open AAA Repair
- Lower Limb Amputation
- Angioplasty and Stenting
- Embolectomy
- Femoral Endarterectomy
- Arterial Bypass
- Axillofemoral Bypass
- Lower Limb Bypass
- Fem-Fem Crossover
- Endovenous Ablation
- Varicose Veins Stripping
- Foam Sclerotherapy
- AV Fistula Formation
- Cervical Rib Excision
- Flexible Cystoscopy
- Rigid Cystoscopy
- Suprapubic Catheterisation
- Scrotal Exploration
- Inguinal Orchidectomy
- Hydrocoele Excision
- Epididymal Cyst Excision
- Circumcision
- Dorsal Slit Procedure
- Ureteric Stent Insertion
- Percutaneous Nephrolithotomy
- Nephrectomy
- Flexible Nasal Endoscopy
- Microlaryngoscopy
- Grommet Insertion
- Myringoplasty
- Adenoidectomy
- Septoplasty
- Functional Endoscopic Sinus Surgery
- Parotidectomy
Last updated: July 2, 2023 Revisions: 18
- 1 Introduction
- 2.1 Clinical Features
- 2.2 Management
- 3.1 Clinical Features
- 3.2 Investigation and Management
- 4.1 Clinical Features
- 4.2 Investigation and Management
- 5 Key Points
Introduction
Vertigo is a specific symptom of hallucination of movement or spinning of the environment, often resulting in issues with balance .
Whilst aetiology varies, all causes of vertigo produce a conflict between the vestibular input and other sensory inputs of balance (i.e. proprioception and vision), resulting in the sensation of vertigo.
The causes of which can be divided into central or otological:
- Central causes of vertigo include multiple sclerosis, posterior stroke, migraine, or intracranial space occupying lesion
- Otological causes of vertigo include Benign Positional Paroxysmal Vertigo, Meniere’s Disease, and Vestibular Neuronitis
Balance disorders can be multifactorial and have a wide range of causes outside of disorders of the vestibular system or brain. It is important to consider alternative medical issues , such as circulatory/cardiac disease and metabolic issues. Indeed, in the acute setting, the most critical diagnosis to exclude is a posterior circulation stroke.

Figure 1 – The hallucination of movement felt with vertigo
Benign Positional Paroxysmal Vertigo
Benign Positional Paroxysmal Vertigo (BPPV) is caused by the presence of canaliths in the semi-circular canal instead of the utricle (Fig. 2).
Once in the canal, movement of the patient’s head will result movement of these crystals that cause an abnormal movement of endolymph , resulting in vertigo. Risk factors for BPPV include head injury, previous history of labyrinthitis, and older patients. That said, in most patients it is unprovoked.
Clinical Features
In BPPV, vertigo attacks last seconds and result from the same head movement causing the onset of symptoms every time. Accompanying symptoms typically include nausea or vomiting . A classical history is of vertigo when turning the head, e.g. movement of the head on the pillow in the morning.
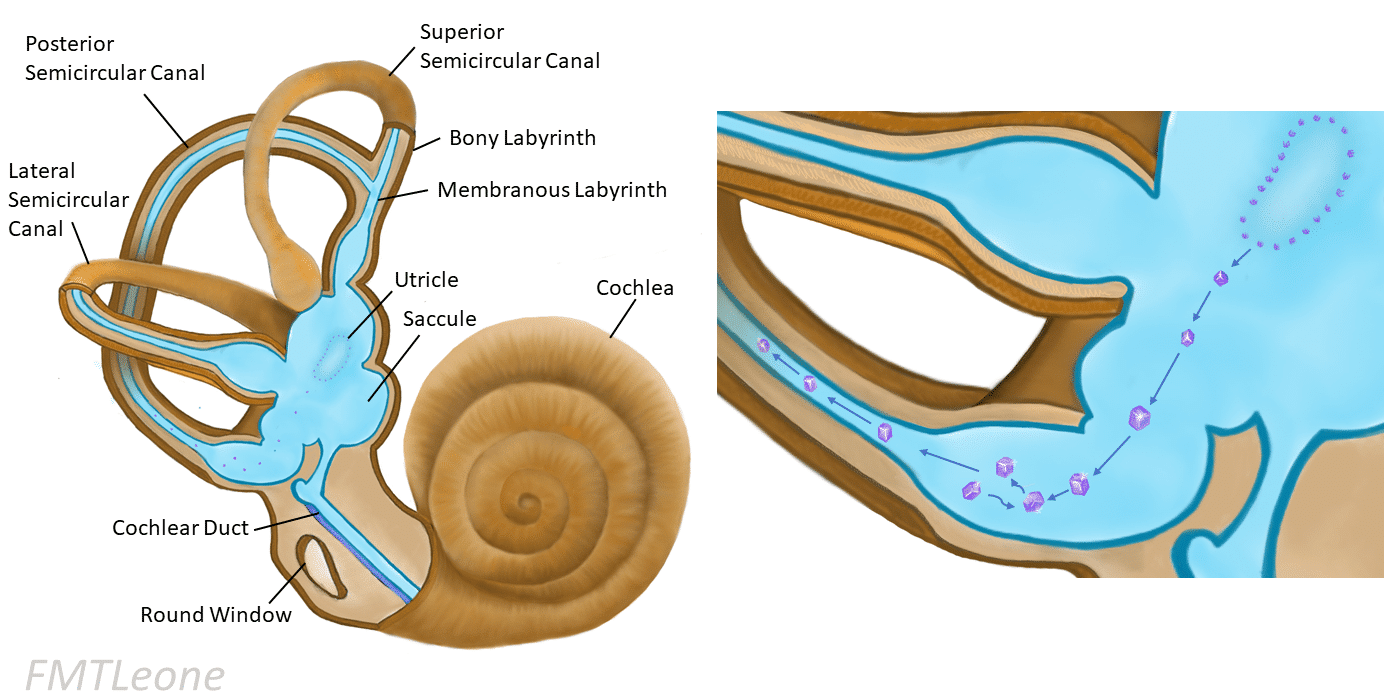
Figure 2 – Formation of crystals and their migration into the semi-circular canals in BPPV
The diagnostic examination for BPPV is the Dix-Hallpike manoeuvre , with a positive test invoking the symptoms and nystagmus * will be present. The nystagmus will typically fatigue in less than a minute.
Once the condition is diagnosed, specific manoeuvres can be employed to remove the crystals from the canal and resolve the symptoms. A common manoeuvre is Epley’s Manoeuvre , performed if the canalith are in the posterior canal.
Patients post-Epley’s manoeuvre are advised not to drive, to keep sleep upright, not to bend down or look upwards for 48 hours. Resolution is not always complete , with some patients requiring repeated Epley’s as symptoms persist, and BPPV can also recur.
Patients can also be advised to perform Brandt-Daroff exercises , positions they can practice at home that are beneficial in reducing symptom intensity.
*Most commonly crystals form in the posterior canal, resulting in a rotatory nystagmus to be present; if in the horizontal canal then result in a horizontal nystagmus.
Meniere’s Disease
Meniere’s Disease is a disorder comprised with a triad of symptoms including vertigo , hearing loss , and tinnitus . Current theories in its pathophysiology suggest the symptoms result from an increase in endolymphatic pressure .
Caused by dysfunctioning sodium channels , an osmotic gradient is subsequently set up that draws fluid into the endolymph, i ncreasing the endolymphatic pressure to cause symptoms.
Figure 3 – The components of the membranous labyrinth
Meniere’s disease presents with attacks comprised of a triad of severe paroxysmal vertigo , sensorineural hearing loss , and tinnitus .
Symptoms are predominantly unilateral , lasting for minutes to hours , and usually resolve within 24 hours . During remission between attacks, the symptoms will improve yet repeated attacks result in a sensorineural hearing loss that worsens over time.
Whilst the disease will burn out eventually with time, permanent sensorineural hearing loss can remain.
Investigation and Management
Otoscopy will show a normal ear drum , audiometry will show a low frequency sensorineural hearing loss , and tympanometry will show type A (normal). In acute attacks, the vertigo and nausea symptoms can be reduced by a short course of prochlorperazine (a vestibular sedative), given either buccal or intramuscular.
Some conservative measures have been suggested to aim to reduce attack frequency such as lifestyle advice (reducing salt or avoiding chocolate and caffeine) and regular betahistine medication .
If attacks persist despite prophylaxis, surgical intervention may be warranted . This can include intratympanic gentamicin injections, intratympanic steroid injections, endolymphatic sac destruction, or labyrinthectomy (now rarely performed).
Vestibular Neuronitis
Vestibular neuronitis is inflammation of the vestibular nerve , resulting in vertigo that typically lasts days but can last weeks to months. Most cases are due to a viral infection , with a upper respiratory tract infection preceding its onset in half of cases.
Symptoms will be sudden onset and severely incapacitating , nearly always associated with nausea and vomiting .
On otoscopy, the ear drum will be normal and a horizontal nystagmus will be present when examining the eyes. Neurological examination will be unremarkable and the hearing for these patients will be normal.
Whilst most cases resolve fully within a week ; long-term vestibular deficit after the acute episode can lead to unsteadiness over a period of weeks whilst the brain compensates for this.
In an acute presentation of dizziness , assessment of a central neurological cause is essential, especially for posterior circulation stroke. Initially this typically involves CT head imaging and, if any uncertainty persists, a subsequent MRI head scan.
Once diagnosed, however, most patients can be managed at home . During the acute episode, a patient may require vestibular sedatives (to be stopped after the acute episode), also considering intravenous fluids if the patient becomes dehydrated from vomiting.
If there are persistent problems due to vestibular hypofunction, then the patient may require longer term vestibular rehabilitation via Cawthorne-Cooksey exercises .
- Vertigo can be divided into central and otological causes
- Balance disorders can be caused by a wide range of multifactorial and medical issues such as cardiac or metabolic disorders, especially a posterior circulation stroke in the acute setting
- Main otological causes include Benign Positional Paroxysmal Vertigo, Meniere’s Disease, and Vestibular Neuronitis
- BPPV symptoms last second to minutes, Meniere’s Disease symptoms last minutes to hours, and Vestibular Neuronitis symptoms last days to weeks.
[embed]https://www.youtube.com/watch?v=fd8TVMOYqZg[/embed]
[start-clinical]
[end-clinical]
Found an error? Is our article missing some key information? Make the changes yourself here!
Once you've finished editing, click 'Submit for Review', and your changes will be reviewed by our team before publishing on the site.
We use cookies to improve your experience on our site and to show you relevant advertising. To find out more, read our privacy policy .
Privacy Overview
| Cookie | Duration | Description |
|---|---|---|
| cookielawinfo-checkbox-analytics | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics". |
| cookielawinfo-checkbox-functional | 11 months | The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional". |
| cookielawinfo-checkbox-necessary | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary". |
| cookielawinfo-checkbox-others | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other. |
| cookielawinfo-checkbox-performance | 11 months | This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance". |
| viewed_cookie_policy | 11 months | The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data. |
Acute Dizziness
Table of contents.
Published March, 2021
Meara Melton, MD Expert review, pending
- Use timing and triggers to differentiate dizziness into four limited differential categories. .
- Perform a bedside Dix-Hallpike exam to diagnose the cause of acute episodic, positionally triggered dizziness.
Perform the HINTS exam to identify concerning features in continuous, spontaneous dizziness.
- Construct a four-step history and physical exam process to differentiate between benign and central causes of dizziness.
Teaching Instructions
Plan to spend at least 30-60 minutes preparing for this talk. Acute dizziness is a topic that is overwhelming and the goal of this talk is to make sure the learners have a general framework, understand key exams for diagnosis, and can identify life-threatening and time-sensitive situations.
This talk begins by presenting a systematic way for learners to think through the patient presenting with acute dizziness using a modified TiTrATE (Timing, Triggers And a Targeted Exam). 1 It is designed to focus on the exam and workup for episodic, positionally-triggered symptoms and continuous, spontaneous symptoms. When introducing the framework, we review the Dix-Halpike maneuver and the HINTS exam. The learners then work through three cases, which highlight positive exam findings during diagnosis and management. If desired, this lecture can be divided into two 20 minute talks by introducing the framework in the first talk and working through the 3 cases in the second.
We have not yet created a Learner board so you will need to use the Presenter board to get a gist of the flow for this talk. On the PowerPoint, every box with a black cursor is an animated button. You will want to click these to advance through the presentation. Select the “home” icon to return to the algorithm at any time and the large blue arrow to return to the cases.
This talk can be presented in two ways:
- Project the “Interactive Board for Presentation”.
- Reproduce a drawing of the presentation on a whiteboard.
With either method, print out copies of the Learner’s Handout so they may follow along during the presentation and take notes as you expand on the decision tree and apply it through the three practice cases. Begin with reviewing the objectives for the session.
Objective 1
Use timing and triggers to differentiate dizziness into four limited differential categories
One of the key objectives of this talk is to establish a consistent framework that is easy to navigate. There are multiple ways to approach dizziness and many providers have been taught to think of it as vertigo, presyncope, disequilibrium, or lightheadedness. The challenge with this approach is that we often get nonspecific descriptions of dizziness from patients and struggle to put them in a category. TiTrATE is a diagnostic approach to determine the probable etiology of dizziness or vertigo. It uses the Ti ming of the symptom, the Tr iggers that provoke the symptom, A nd a T argeted E xamination. The framework in this talk takes a modified approach to classify dizziness as 1) episodic positionally triggered, 2) spontaneous episodic, 3) Continuous due to trauma or toxins, or 4) continuous spontaneous.
Navigate through the algorithm by first selecting “Timing” to show how we characterize symptoms broadly as “episodic” or “continuous”. Here you should emphasize that triggered episodic vestibular syndromes last seconds to minutes, spontaneous episodic vestibular syndromes last minutes to hours, acute vestibular syndromes with the spontaneous onset, and constant vertiginous symptoms last hours to days.
Before expanding the 4 general categories, you may want to ask learners what history or exam findings they want to elicit in a patient presenting with dizziness. Some things to make sure are covered include:
- Assess cardiovascular risk factors, which would increase suspicion for possible posterior circulation stroke affecting the vestibular system.
- Ask about associated hearing loss or tinnitus.
- Assess for additional neurologic symptoms that suggest a central cause.
- Take a complete social history including substance use.
- Review medications/changes
Then click “Trigger” to reveal the four general categories. Reveal the algorithm for “spontaneous episodic” and “trauma or toxins” by clicking on them and briefly talk about how to approach these categories. Things to emphasize:
Spontaneous episodic: Briefly discuss that hearing loss can be evaluated using the Weber/Rinne tests. Meniere disease is often associated with hearing loss. Vestibular migraine should be considered in those with a history of migraine. Consider vasovagal causes or panic attacks in those with associated psychological stress.
Continuous due to trauma or toxins: Almost every class of medications can lead to symptoms of dizziness so we do not list them all out individually. Patients will often have had dizziness that persists, is usually not debilitating, and is not associated with other neurologic changes. Some of the biggest culprits are anti-epileptics, sedatives, anti-hypertensives and analgesics.
Objective 2
Perform a bedside Dix-Hallpike exam and orthostatics to diagnose the cause of acute episodic, positionally triggered dizziness
Click “Positionally triggered” to reveal that the Dix-Halpike maneuver should be performed to determine the diagnosis. Click on the image to link to a picture of the Dix-Halpike maneuver – click on the image to link to a video demonstrating the technique, if desired. If delivering this in person, you can have learners practice on one another at this point. Click the large blue arrow in the top-left corner to return to the framework. Share that a positive Dix-Halpike maneuver suggests the patient has BPPV due to canalith particles in the semicircular canal. A negative test suggests we should perform orthostatics and re-consider other causes.
Objective 3
Click “Spontaneous” to reveal that the HINTS exam should be performed to help further differentiate the cause. Click on the play button to link to a video demonstrating the technique for the HINTS exam. This video is 8 minutes. After the video, reiterate that the HINTS exam should be performed only on those patients with acute persistent dizziness and review how to interpret the findings:
- Catch-up saccades are considered a “reassuring exam” and suggest a peripheral cause
- The absence of catch-up saccades in a patient with continuous dizziness is abnormal and suggests a central cause
- Normal if horizontal and unidirectional
- Abnormal if bidirectional, rotational
- Normal if eyes remain fixed
- Abnormal if eyes exhibit disconjugate gaze
Click “HINTS exam” to reveal that ANY concerning HINTS findings suggest a central cause and if ALL HINTS findings are reassuring, it is likely a peripheral cause like vestibular neuritis or labyrinthitis.
Objective 4
Use a four-step history and physical exam process to differentiate between benign and central causes of dizziness.
Click on each case to reveal the stem of the case and work through it using the TiTrATE format introduced in the framework. At any point, you can click the “Home” button in the top-right corner to return to the algorithm.
Case 1: BPPV
- Click on the exam to link to a video showing an abnormal Dix-Halpike.
- Discuss management options, which include the Epley Maneuver and Half-Somersault maneuver. Click on the maneuvers to link to a slide with an image depicting how it is performed. Emphasize that in small studies the Epley maneuver has been shown to be more effective, but patients had lower adherence than with the half-somersault. You can refer patients to Vestibular physical therapy for additional treatment.
Case 2: Acute cerebrovascular accident
- Click on the exam to link to a slide showing an abnormal HINTS exam. Navigate through the slide by clicking on the boxes with a cursor and return to the case by clicking the large blue arrow in the top-left corner.
- Briefly discuss that management includes emergent imaging with non-contrast CT, MRI/MRA, antiplatelets and statin. Depending on the time course, patient factors and local resources, this may be managed with TPA or thrombectomy.
Case 3: Vestibular neuritis
- Click on the exam to link to a slide showing a normal HINTS exam. Navigate through the slide by clicking on the boxes with a cursor and return to the case by clicking the large blue arrow in the top-left corner.
Discuss that management for vestibular neuritis typically includes antiemetics and anticholinergics. Steroids are often offered for vestibular neuritis, but share with the learner that the primary research comes from small trials with weak outcome measures (for example, looking at caloric recovery and not at quality of life measures). Learners will often ask at this point if steroids are indicated for acute idiopathic hearing loss and the answer should be yes.
coming soon
Interactive Boards
For teaching.
Use for Presenting – there is less text and fewer pop-ups
Take Home Points
- Using Timing and Triggers to narrow the differential for acute dizziness simplifies the next steps for the bedside exam to determine concern for a central process.
- The Dix-Halpike maneuver should be performed to differentiate BPPV from other causes in patients presenting with episodic and positionally triggered dizziness.
- The HINTS exam should be employed to evaluate for cerebrovascular events that are time-sensitive and potentially life-threatening in those patients presenting with acute, persistent, vertiginous symptoms.
Fishman JM, Burgess C, Waddell A. Corticosteroids for the treatment of idiopathic acute vestibular dysfunction (vestibular neuritis). Cochrane Database of Systematic Reviews. 2011; 5. Art. No.: CD008607. doi:10.1002/14651858.CD008607.pub2
Muncie, HL, Sirmans, SM, James, E. Dizziness: Approach to Evaluation and Management. Am Fam Physician. 2017; 95(3):154-162
Newman-Toker DE, Edlow JA. TiTrATE: A Novel, Evidence-Based Approach to Diagnosing Acute Dizziness and Vertigo. Neurol Clin. 2015;33(3):577-viii. doi:10.1016/j.ncl.2015.04.011
Kattah, J. C., Talkad, A. V., Wang, D. Z., Hsieh, Y. H., & Newman-Toker, D. E. (2009). HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke , 40 (11), 3504-3510.
Spiegel, R., Kirsch, M., Rosin, C., Rust, H., Baumann, T., Sutter, R., … & Mantokoudis, G. (2017). Dizziness in the emergency department: An update on diagnostics. Swiss medical weekly , 147 (5152), w14565.
Comment on this article
You must be logged in to post a comment.
Patient confidentiality is a priority. No case presented here contains uniquely identifying characteristics, nor do the cases reflect the presentation or care of any one individual. Rather, they represent a compilation of similar cases adapted to achieve the greatest educational value and generalizability.
The authors provide this content for educational purposes only. This content is not intended, nor should it be used as medical advice.
The content on this site does not necessarily represent the opinions of the principal author, team or their employer.
Copyright © 2020 · TeachIM, Inc · nonprofit 501c3
- - Google Chrome
Intended for healthcare professionals
- My email alerts
- BMA member login
- Username * Password * Forgot your log in details? Need to activate BMA Member Log In Log in via OpenAthens Log in via your institution
Search form
- Advanced search
- Search responses
- Search blogs
- Acute vertigo: getting...
Acute vertigo: getting the diagnosis right
- Related content
- Peer review
- Kiran Agarwal , general practitioner 1 ,
- James Harnett , consultant in emergency medicine 2 ,
- Nishchay Mehta , consultant ENT surgeon 3 ,
- Fiona Humphries , consultant in stroke medicine 4 ,
- Diego Kaski , consultant neurologist 5
- 1 Ashlea Medical Practice, Surrey, UK
- 2 Emergency Department, University College London Hospitals NHS Foundation Trust, London, UK
- 3 University College London Hospitals Biomedical Research Centre, National Institute for Health Research, London, UK
- 4 Comprehensive Stroke Service, University College London Hospitals NHS Foundation Trust, London, UK
- 5 Department of Clinical and Movement Neurosciences, University College London, UK
- Correspondence to: D Kaski d.kaski{at}ucl.ac.uk
What you need to know
All patients presenting with brief episodic acute vertigo or unsteadiness should undergo a Dix-Hallpike manoeuvre
Consider stroke in patients with new onset acute unilateral hearing loss and vertigo
Urgent brain imaging is always indicated when acute vertigo is accompanied by other central neurological signs (such as dysphagia, dysarthria, diplopia)
Severe acute gait ataxia (patient unable to stand without support) is most common with central causes of vertigo (such as cerebellar lesions) rather than inner ear causes
Dizziness is a common presentation to emergency departments and primary care. 1 2 It is defined as the sensation of disturbed or impaired spatial orientation without a false or distorted sense of motion. 3 The estimated prevalence of dizziness in a general practice community sample varies across studies 4 but is approximately 20%. 5 6 Its prevalence increases with age.
While patients often use the word “dizziness” to describe their symptoms, this encapsulates a variety of distinct symptom clusters, including vertigo (box 1). Vertigo is a specific type of dizziness defined as the sensation of self motion when no self motion is occurring or the sensation of distorted self motion during an otherwise normal head movement. 3 Acute vertigo represents up to 5% of all admissions to the emergency department. 7
Specific definitions that are often included under the term “dizziness”
Dizziness— The sensation of disturbed or impaired spatial orientation without a false or distorted sense of motion
Vertigo— The sensation of self motion when no self motion is occurring or the sensation of distorted self motion during an otherwise normal head movement
Light-headedness— A feeling you are “going to faint”
Imbalance— A state of being out of equilibrium, or with loss of balance
Gait disorder— A problem or difficulty with walking
Acute vestibular syndrome— Sudden onset of vertigo, nausea, postural instability, and nystagmus lasting for ≥24 hours
Transient vestibular syndrome— Sudden onset of …
Log in using your username and password
BMA Member Log In
If you have a subscription to The BMJ, log in:
- Need to activate
- Log in via institution
- Log in via OpenAthens
Log in through your institution
Subscribe from £184 *.
Subscribe and get access to all BMJ articles, and much more.
* For online subscription
Access this article for 1 day for: £50 / $60/ €56 ( excludes VAT )
You can download a PDF version for your personal record.
Buy this article
Got any suggestions?
We want to hear from you! Send us a message and help improve Slidesgo
Top searches
Trending searches

hispanic heritage month
21 templates

109 templates

17 templates

35 templates

suicide prevention
9 templates

Dizziness Clinical Case
It seems that you like this template, dizziness clinical case presentation, premium google slides theme, powerpoint template, and canva presentation template.
Are you feeling dizzy? It could be that you just had a sudden drop in blood pressure, or maybe anemia? It could also be a heart disease, or it could be as simple as a mild dehydration! There are so many options to consider… expose them all in this modern template for clinical cases, and let the symptoms and the patient guide you and your audience through the correct diagnostic
Features of this template
- 100% editable and easy to modify
- 33 different slides to impress your audience
- Contains easy-to-edit graphics such as graphs, maps, tables, timelines and mockups
- Includes 500+ icons and Flaticon’s extension for customizing your slides
- Designed to be used in Google Slides, Canva, and Microsoft PowerPoint
- 16:9 widescreen format suitable for all types of screens
- Includes information about fonts, colors, and credits of the resources used
What are the benefits of having a Premium account?
What Premium plans do you have?
What can I do to have unlimited downloads?
Don’t want to attribute Slidesgo?
Gain access to over 29900 templates & presentations with premium from 1.67€/month.
Are you already Premium? Log in

Register for free and start downloading now
Related posts on our blog.

How to Add, Duplicate, Move, Delete or Hide Slides in Google Slides

How to Change Layouts in PowerPoint

How to Change the Slide Size in Google Slides
Related presentations.

Premium template
Unlock this template and gain unlimited access

- Upload Ppt Presentation
- Upload Pdf Presentation
- Upload Infographics
- User Presentation
- Related Presentations

Dermatologic Infections in Children
By: yourdoctors Views: 464

Cardiac Physiology
By: yourdoctors Views: 838

Sickle Cell Genetics
By: yourdoctors Views: 708

Ankle Sprains
By: yourdoctors Views: 635

Guideline of Coronary Artery Revascularization
By: yourdoctors Views: 679

By: bagaric Views: 981

Pharmacotherapy for Substance Use Disorders
By: drdwayn Views: 919

Myastenia gravis
By: Mana.jameie Views: 3184

Cholinergics and anticholinesterases
By: JenniferDwayne Views: 1101

Congenital malformations and hydrocephalus
By: drdwayn Views: 1125

- About : Web Developer/Designer
- Occupation : Medical Establishment
- Specialty : Medical Device Company
- Country : India
HEALTH A TO Z
- Eye Disease
- Heart Attack
- Medications
- Vote: Reader’s Choice
- Meta Quest 4
- Google Pixel 9
- Google Pixel 8a
- Apple Vision Pro 2
- Nintendo Switch 2
- Samsung Galaxy Ring
- Yellowstone Season 6
- Recall an Email in Outlook
- Stranger Things Season 5
How to change the background in Powerpoint

You can change the background to anything you like if you're using Powerpoint to create presentations: a picture, a color, a gradient, or even an in-motion video. You'll know the best background for your presentation, but whatever you want to change it to, we're here to help you do it.
How to change the background to a color or gradient
How to add a picture to the background, how to add a video to the background.
Here's how to change the background in Powerpoint to a few different styles.
What You Need
Don't have Powerpoint installed already? Here's how to download it.
Beyond an empty background, the most simple background you can add to your Powerpoint presentation is a flat color, or a gradient from one color to another. Here's how to do it.
Step 1: Open your Powerpoint document and select the slide that you want to change the background for, on the left-hand side. In this example, we're using the standard template for an architectural pitch presentation.
Step 2: Select Design in the top-menu bar.
Step 3: Select Format Background in the top right.
Step 4: From the menu that appears, select either Solid fill or Gradient fill depending on your needs.
Step 5: If you want a solid color, select the paint can icon and choose your color preference. You can select from a range of curated color options, select More colors for a greater array of options, or use the Eyedropper tool to grab a color from the presentation to use for your background.
You can also adjust the transparency using the slider, to fade the color in and out.
If you want a gradient from one color to another, you can select a Preset gradient between two colors — but you can also fine-tune it using the Gradient stops options to control the number and type of color changes within the gradient. You can also adjust the position, transparency, direction, and brightness of the colors and the gradient itself.
Step 6: Play around with the option until you're happy. If you want to start again at any point, select the Reset background button at the bottom of the Format Background menu.
When you're happy with the result, just close the menu down by selecting the X icon in the top-right corner of the Format Background menu. Alternatively, if you want to apply that gradient or solid-color background to every slide, select the Apply to all button at the bottom of the window.
Would you rather make an image the background for your presentation's slide(s)? You can do that too.
Step 1: Select the slide that you want to change the background for, on the left-hand side. Then select Format Background in the top-right.
Step 2: Select Picture or texture fill .
Step 3: If you want to use a texture for the background, select the box next to Texture and choose the texture you want for the background from the pop-out window.
Step 4: If you want to use an image, select the Insert button under the "Picture source" subheading. Then decide where you want to source the image from.
Step 5: Select From a file if you want to use a local image file, then choose it using the file explorer and select Open . If you'd rather source it online, stock images, or the stack of pre-installed logos, select those and follow the on-screen instructions to introduce the image.
Step 6: If you want the image or texture to appear in the background of all slides, select the Apply to all slides button at the bottom right of the screen.
You can embed a video in a PowerPoint presentation , but if you want to really spice up a slide, why not change the entire background to a video? Here's how to do it.
Step 1: Select Insert followed by Video . Choose whether you want to add a video from your local device or an online source. If the former, select it from the file explorer and select Open . If it's online, paste the URL and select Insert .
In this example, I'm using a clip from the 1988 sci-fi comedy Red Dwarf .
Step 2: Use your mouse to drag and move the video so that it covers the portion of the slide that you want it to play on (or the whole thing). You can resize it too, using the corner controls by clicking and dragging.
Step 3: Right-click the video and select Send to back .
You can also take this opportunity to use the built-in controls to trim the video if it needs it, choose when you want it to start (automatically, or when clicked on), and its style — whether you want it to appear at an angle or with a fade around it.
Step 4: When you're happy with the video's implementation, select Slideshow at the top, then select either From beginning or From current slide in the top left to check out the presentation to make sure the video is working correctly.
If it's not in the right position, starts at the wrong point, or isn't formatted how you'd like it, use the right-click controls on the video to make your adjustments.
Now that you've become a master of Powerpoint backgrounds, how about playing around with the new Copilot features? Here are five of the best things you can do with Copilot Pro right now.
Alternatively, hone your presentation creating skills with these Microsoft PowerPoint best practices .
Editors’ Recommendations
- How to add audio to PowerPoint
- How to add notes to your Microsoft PowerPoint slides
- How to convert PDF to PowerPoint
- How to embed a video in PowerPoint
- How to use Microsoft PowerPoint
- How-To Guides

Online team collaboration is the new norm as companies spread their workforce across the globe. Gone are the days of primarily relying on group emails, as teams can now work together in real time using an instant chat-style interface, no matter where they are.
Microsoft Teams is one of many collaboration tools designed to bring company workers together in an online space. It’s not designed for communicating with family and friends, but instead provides a platform for video conferencing, real-time discussions, document sharing and editing, and more for companies and corporations. What is Microsoft Teams? Microsoft Teams is a chat-based workspace initially introduced in 2016 for customers subscribing to the Office 365 Enterprise and Business plans, serving as the successor to Microsoft’s Skype for Business platform. It also replaced the Microsoft Classroom service in Office 365 Education.
Double-spacing is a great way to organize your word processing, and an excellent optimization that is built into most word processing tools. And whenever we hear “word processing,” one of the first programs that comes to mind is Microsoft Word. Learning how to use Microsoft Word is usually straightforward, but it has various formatting features that aren't immediately obvious. Here, we’re going to teach you how to implement double spaces throughout your next Word doc.
Microsoft Word is one of the most feature-rich word processing tools gifted to us human beings. In fact, the very word “Word” has invaded nomenclature to the point where any discussion of this type of software, regardless of what the product is actually called, typically results in at least one person calling the software “Word.”
With each new release of the industry-lauded software, we get more and more capabilities. But this shouldn’t prevent us from knowing how to incorporate classic Word elements, such as the hanging indent. We understand how tough it can be to stay on top of how to use Microsoft Word though, so we’ve made this guide to teach you how to quickly and easily add a hanging indent to your next Word doc.
How to Record a PowerPoint Presentation

Knowing how to record a PowerPoint presentation with audio and video can provide viewers with an engaging experience. Whether you're creating a tutorial , a lecture, or a business presentation, combining visuals with narration helps convey your message more effectively.
In this guide, we will walk you through the step-by-step recording process in PowerPoint . From setting up your equipment and recording your screen to editing the final video, you'll learn everything you need to know about creating narrated PowerPoint presentations.
Prepare everything
- Presentation . Ensure your slides are complete and in the correct order. Update PowerPoint to the latest version for the best performance and features.
- Microphone . Use a good-quality microphone to record clear audio . A USB or headset microphone is recommended.
- Webcam (Optional) . If you want to include a video of yourself, use a built-in or external webcam.
- Script . Outline what you want to say for each slide. This will help you stay on track during the presentation recording.
How to record a PowerPoint presentation?
1. set up a screen recorder.
Download and install the free screen recording software for Windows from the official website. Launch the video recorder on your computer.
Easy to use free screen recorder for PC. Record desktop, take screenshots, upload the created content to the cloud for easy and fast sharing.

2. Configure settings
Go to " Settings " to set recording preferences .
- In " Video ", choose the desired output quality and format. Make sure the toggles next to " Record mouse movements " and " Animate mouse clicks " are enabled if needed.
- In the " Audio " tab, adjust the sound levels and select the desired input devices.

3. Record your presentation
Click the " Capture video " option in the side menu and select the mode. Choose the entire display if your presentation is in full-screen mode. You can also manually adjust the screen recording area to show the desired content.
Open your PowerPoint and press the F7 hotkey or click the " Rec " button to record the presentation with audio . Navigate through your slides while speaking clearly into the microphone.
Use drawing tools in the presentation recorder to highlight key points during your narration.
If you need to take a break, use the pause button to temporarily stop the recording. When you've completed your presentation, press the F8 hotkey or click " Stop ".

4. Editing the final video
Use the built-in video editor to trim any unwanted parts of the presentation recording. You can also adjust the playback speed, change the format, and resize the video.
If you need to make more changes, you can import your recorded clip into third-party video editing software . Add transitions, effects, background music, or other enhancements as needed.
Save your edited video in the desired location. It is also possible to upload the recording to the cloud and share it via a link .

FAQ on how to record a presentation
PowerPoint screen recording with audio and video is a powerful way to enhance your message and engage your audience. By following the steps outlined in this guide, you can create professional and polished videos that combine your slides with a voice-over .
Whether you're an educator, business professional, or content creator, knowing how to narrate a PowerPoint presentation recording can significantly boost your impact. Remember to practice your delivery and utilize editing tools to refine your final product.
Expert Tech Writer
Like the article? Share it!
Your current User-Agent string appears to be from an automated process, if this is incorrect, please click this link:
Intel's Core Ultra 200V chips aim for AI PC dominance
Lunar lake is coming on september 24th..
The race to build the most compelling AI PC processors continues with the launch of Intel's Core Ultra 200V. At Computex in June , we learned these "Lunar Lake" laptop chips would feature a powerful 48 TOPS (tera operations per second) neural processing unit for AI work, and, surprisingly enough, they'd also sport up to 32GB of built-in memory for faster performance and lower power consumption. Today at Germany's IFA trade show, Intel has given us an even closer look at its next-generation AI PC hardware.
According to Intel, the Core Ultra 200V will be "the most efficient x86 processor ever," with up to 50 percent lower on-package power consumption. In addition to bringing memory directly on the chip, Intel also doubled the cache and core count (reaching 4MB and 4 cores) for its "Low Power Island," which handles less demanding work. Performance per watt has also more than doubled across general performance and gaming, thanks tot he new Xe2 built-in GPU. (One example: Intel claims the Core Ultra 200V uses 35 percent less power than the previous generation, while also getting 32 percent faster performance.)
It's clear that Intel is gunning directly for Qualcomm, whose Arm-based Snapdragon chips have traditionally been more power efficient than x86 processors. Intel even claims it has a lead in battery life. In one test performed on the same laptop model, the Core Ultra 7 268V lasted for 20.1 hours in the UL Procyon Office Productivity benchmark, compared to 18.4 hours with a Qualcomm X Elite chip. The Snapdragon system still maintained a lead in a Microsoft Teams 3x3 test, lasting 12.7 hours compared to the Intel 268V's 10.7 hours.
In practically every way, the Core Ultra 200V is a rethinking of Intel's traditional x86 processor design. For example, the company has given up on its Hyperthreading technology, which virtually allowed a single CPU core to support multiple task threads. Instead, Intel is optimizing the new chips for single-threaded performance. The company claims the Core Ultra 200V's P-cores (performance) are 14 percent faster than the last generation, and its E-cores (efficiency) are a whopping 68 percent faster.
Unlike Qualcomm's Snapdragon chips, Intel's Core Ultra 200V processors can also run legacy x86 software without any issue. There's no emulation slowdown or Arm incompatibility to worry about. While I was impressed by the Snapdragon X Elite chips on the Surface Pro and XPS 13 Copilot+ systems , Windows on Arm performance issues remains, like their inability to play games with strong anti-cheat protection like Fortnite . If you're at all worried about running older software or games, it makes sense to stick with an x86 chip for the next few years.
While the Core Ultra 200V series tops out with 8-core 8-thread processors, Intel says it's up to three times faster than its previous chips when it comes to performance per thread. And if that's not boastful enough, Intel also claims its new Xe2 GPU is 32 percent faster than before, 68 percent speedier than Qualcomm's 12-core X Elite chip and 16 percent better than AMD's HX 370. The Xe2 also adds an additional 67 TOPS of AI compute performance, in addition to the NPU's 48 TOPS.
When it comes to AI, Intel claims the Core Ultra 9 288V's NPU is 79 percent faster denoising in Adobe Lightroom compared to its previous chip. The Snapdragon X Elite 78-100, meanwhile, was 66 percent slower than Intel's last chip. As always, we'll need to do our own testing to confirm the company's figures, but it's clearly not being shy about its potential performance leads.
The Intel Core Ultra 200V family tops out with the Ultra 9 288V, which features eight cores (4P + 4E) with up to 5.1GHz Max Turbo speeds on the P cores. That model also comes stacked with hte most powerful 8-core Xe2 Arc 140V GPU and 32GB of RAM. While all of the 200V chips feature 8-cores, their respective GPU, NPU and RAM all scale down across the line. The bottom-rung Core Ultra 226V, for example, sports a 7-core Arc GPU, 40 TOPS NPU and 16GB of RAM.
Just like Apple's M-series chips, the Core Ultra 200V's built-in memory means you won't be able to upgrade your memory down the line. That's a particular shame, as we're finally easily upgradable LPCAMM2 memory making its way to notebooks. At least Intel isn't forcing anyone to permanently live with 8GB of RAM, though.
Intel Core Ultra 200V systems will be available on September 24th from major manufacturers like Dell, ASUS and Acer.
- Advertisement

Aug 11, 2014
510 likes | 1.9k Views
To insert your company logo on this slide From the Insert Menu Select “Picture” Locate your logo file Click OK To resize the logo Click anywhere inside the logo. The boxes that appear outside the logo are known as “resize handles.” Use these to resize the object.
Share Presentation
- benign positional vertigo
- ent specialist
- symptomatic recovery
- last seconds
- first awakening

Presentation Transcript
To insert your company logo on this slide • From the Insert Menu • Select “Picture” • Locate your logo file • Click OK • To resize the logo • Click anywhere inside the logo. The boxes that appear outside the logo are known as “resize handles.” • Use these to resize the object. • If you hold down the shift key before using the resize handles, you will maintain the proportions of the object you wish to resize. Vertigo Lawrence Pike James Street Family Practice
Definition An illusion or hallucination of movement which is usually rotation, either of oneself or the environment
Major Causes in General Practice 3 Major Causes: Vestibular Neuronitis Benign Positional Vertigo Meniere’s
Vestibular Neuronitis
Vestibular Neuronitis - Features • Commonly occurs on first awakening • Nausea is marked and almost universal • 57% evidence or recent viral infection • Fine horizontal or rotatory nystagmus
Vestibular Neuronitis - Course • Attacks become sequentially shorter and if not then consider another diagnosis • Vertigo symptoms usually resolve over a few days as vestibular compensation occurs
Vestibular Neuronitis - Management • Symptomatic treatment for first few days only • Vestibular drugs delay compensation
Vestibular Neuronitis - Prognosis • Excellent • 5% progress to Benign Positional Vertigo
Benign Positional Vertigo
Benign Positional Vertigo - Features • Recurrent • Brought on by changes in head position • Episodes last seconds, never >5 mins • Onset late middle age usually • Females : Males = 2 : 1 • Typically turning over in bed, bending over and straightening, extending neck
Benign Positional Vertigo - Management • Vestibular sedatives should be avoided where the vertigo becomes chronic as they supress vestibular feedback crucial for compensation and symptomatic recovery
Benign Positional Vertigo - Brandt-Daroff Exercises • Simple repositioning exercises and are appropriate for less severe BPV • Complete relief within 3 to 14 days
Benign Positional Vertigo - Brandt-Daroff Exercises • Sit patient on couch with eyes closed • Tilt whole upper body laterally towards lesion until lateral aspect of occiput lies on the bed. Maintain until vertigo subsides • Sit patient upright for 30 seconds • Repeat on then other side and rest head for 30 seconds • Repeat every 3 hours during day
Menieres - Features • Hearing Loss • Tinnitus • Vertigo • Sensation of fullness or pressure in ear • Fluctuates and episodic, lasts hours • Unilateral • 20-50 years Familial predisposition
Menieres - Course • Progressive • Early on predominant Vertigo with Deafness but normal hearing between • Later on hearing loss stops fluctuating and becomes progressively worse
Menieres - Management • Referral to ENT Specialist has been recommended for every case of vertigo and hearing loss to exclude acoustic neuroma • Betahistine with or without diuretic is favoured current treatment
Vertigo Final Notes • Vertigo with Diplopia is likely to be a vascular event • Vestibular sedatives are not recommended on a prolonged basis for any type of vertigo
- More by User

VERTIGO. AYESHA SHAIKH PGY2 EMORY FAMILY MEDICINE 09.17.2008. CASE. 31,female doctor, otherwise healthy, post partum week 5. First episode, sudden feeling of room spinning, while entering patient data in computer, during Family Medicine Clinic… One fine day last year same time! .
1.53k views • 37 slides

Vertigo. Southern Neurology. Dizziness – is it vertigo ?. Is the dizziness is vertiginous in nature , or more suggestive of near-syncope or non-vestibular dizziness Is the dizziness is affected by movements of the head, if so it suggests a peripheral vertigo
1.23k views • 41 slides

Vertigo. Dr. Abdulrahman Alsanosi Associate professor King Saud University Otolaryngology consultant Otologist , Neurotologist &Skull Base Surgeon King Abdulaziz University Hospital / KFMC. What are the components of balance system ?. Inner ear (3 semicicular canals and otolith organ )
1.19k views • 36 slides

Vertigo. Dr. Abdulrahman Alsanosi Associate professor Otolaryngology consultant Otologist , Neurotologist &Skull Base Surgeon Head of Otology / Neurotology Unit Director of cochlear implant program King Abdulaziz University Hospital. Importance.
1.18k views • 40 slides

Definition. An illusion or hallucination of movement which is usually rotation, either of oneself or the environment. Major Causes in General Practice. 3 Major Causes:Vestibular NeuronitisBenign Positional VertigoMeniere's. Vestibular Neuronitis. . Vestibular Neuronitis - Features. Commonly
502 views • 18 slides

1.43k views • 61 slides

Vertigo. Case.
320 views • 11 slides

643 views • 24 slides

Vertigo. How many different ways can we look at Hitchcock?. C ritical response to Vertigo. The general consensus of reviews in 1958 was that ‘Vertigo’ is ‘too slow and too long’, which contrasts with today’s general view of ‘Vertigo’, with Rotten Tomatoes giving it a 98% ‘Fresh’. .
763 views • 27 slides

VERTIGO. Controlling a Smartphone from an Architectural Vantage Point . Kirk Swidowski mail [email protected] web www.de7ec7ed.com twitter de7ec7ed github github.com/de7ec7ed. Special thanks to Dr. Joseph Sharkey for his help with the project. About me.
679 views • 46 slides

VERTIGO. 3 D 3 – dimensional flightsystem. VERTIGO An artist flys over the “Stade de France”.
333 views • 6 slides

VERTIGO. Illusion of motion interpreted as self movement or environmental movement Rotating with spinning sense of falling or swaying back and forth: Merry-Go-Round Effect 1/2 of patients with dizziness have vertigo. VERIGO. PERIPHERAL Otitis Media Acute Labyrinthitis
1.36k views • 67 slides

Vertigo. Dr. Victor James Abdullah. Proprioceptors. Vestibular Organ. Vestibular Hair Cells. Semicircular Canals. AICA. Causes of Vertigo. Trauma Infection Vascular Metabolic Dysequilibrium of ageing Psychogenic/Hyperventilation Tumour Meniere’s BPPV. Trauma. Proprioceptors.
1.17k views • 78 slides

VERTIGO. Ermenegildo Zegna Pal Zileri Hugo Boss Van Laack Zilton Brax Morisson Piacenza kashmir Boss Shoes Façonnable Gant. VERTIGO WAREGEM. VERTIGO WAREGEM. VERTIGO WAREGEM. VERTIGO WAREGEM. VERTIGO WAREGEM. VERTIGO WAREGEM. VERTIGO WAREGEM. VERTIGO WAREGEM. VERTIGO
621 views • 25 slides

Vertigo. Vertigo / Dizziness. Sir Terence Cawthorne said: “ Labyrinthine disturbance may make one feel like the end of the world has arrived….” Doctor said: “ dealing with dizzy patient make me dizzy”. Definitions. Dizziness (vertigo):
560 views • 21 slides
IMAGES
VIDEO
COMMENTS
Reflex pathways that are responsible for making compensatory movements and adjustments in body position. Pathways that project to the cortex to provide perceptions of gravity and movement. Components: 3 semicircular ducts (horizontal, anterior and posterior), 2 otolith organs (saccule and utricle), vestibular nuclei, central connections ...
Check out this medical PowerPoint presentation titled "Dizziness and Vertigo" by V. Abbasi, MD.<break><break>This medical PowerPoint presentation is about dizziness and vertigo, two terms that are often used interchangeably, but they actually refer to different sensations.<break><break>Dizziness is a feeling of lightheadedness or unsteadiness that can be accompanied by a range of symptoms ...
Check out this medical PowerPoint presentation titled "Dizziness and Vertigo" by Gail Ishiyama, MD.<break><break>This medical PowerPoint presentation is about dizziness and vertigo, two related but distinct conditions that can cause a person to feel off-balance, unsteady, or disoriented.<break><break>Dizziness is a general term that describes a feeling of lightheadedness or faintness, or a ...
UNDERSTANDING VERTIGO CAUSES AND SYMPTOMS! Causes of Vertigo 1. Benign Paroxysmal Positional Vertigo (BPPV) is a common cause, arising from displaced inner ear crystals, triggering sudden spinning sensations. Meniere's disease, marked by fluid imbalance in the inner ear, leads to recurrent vertigo attacks, often accompanied by hearing loss and ...
Vertigo.ppt - Free download as Powerpoint Presentation (.ppt), PDF File (.pdf), Text File (.txt) or view presentation slides online. This document provides information on evaluating and diagnosing vertigo. It describes the Dix-Hallpike maneuver test and distinguishes between peripheral and central vertigo. Common causes of vertigo are discussed, including benign paroxysmal positional vertigo ...
Vertigo refers to the spinning or movement sensation experienced by an individual when one is stationary and results from issues within the inner ear. Utilize our presentation template for MS PowerPoint and Google Slides to depict how this condition affects a person's balance and spatial orientation and leads to dizziness, nausea, and even falls.
500 likes | 656 Views. Gail Ishiyama, M.D. Assistant Professor Department of Neurology, Division of Neurotology UCLA School of Medicine. Dizziness and Vertigo. Vertigo: illusion of movement Ataxia: inability to co-ordinate movements (walking or of extremities), "feel as if drunk". Download Presentation. vertigo.
Introduction. Vertigo is a specific symptom of hallucination of movement or spinning of the environment, often resulting in issues with balance.. Whilst aetiology varies, all causes of vertigo produce a conflict between the vestibular input and other sensory inputs of balance (i.e. proprioception and vision), resulting in the sensation of vertigo.. The causes of which can be divided into ...
VERTIGO. Apr 01, 2023. 80 likes | 99 Views. Vertigo refers to a spinning sensation, which can occur due to an inner ear problem or a problem with the brainstem. The condition may cause nausea, vomiting, and difficulty balancing. Treatment may include medications, vestibular rehabilitation therapy, or surgery in severe cases. Download Presentation.
Description : Check out this medical PowerPoint presentation titled "Vertigo" by Dr. Thamara Gunasekera. This medical PowerPoint presentation is about Vertigo is a medical condition characterized by a sensation of spinning or whirling, often accompanied by nausea, vomiting, and loss of balance. It can be caused by various factors, including ...
On the PowerPoint, every box with a black cursor is an animated button. You will want to click these to advance through the presentation. Select the "home" icon to return to the algorithm at any time and the large blue arrow to return to the cases. This talk can be presented in two ways: Project the "Interactive Board for Presentation". or
Dizziness is a common presentation to emergency departments and primary care. 1 2 It is defined as the sensation of disturbed or impaired spatial orientation without a false or distorted sense of motion. 3 The estimated prevalence of dizziness in a general practice community sample varies across studies 4 but is approximately 20%. 5 6 Its prevalence increases with age.
The cupular deflection produces nystagmus. Benign positional vertigo -epidemiology In one U.S. study, the age- and sex-adjusted incidence was 64 per 100,000. Incidence in general population is higher in persons older than 40 years. In a recent study of a group of elderly patients, the incidence was found to be approximately 8%.
Contains easy-to-edit graphics such as graphs, maps, tables, timelines and mockups. Includes 500+ icons and Flaticon's extension for customizing your slides. Designed to be used in Google Slides, Canva, and Microsoft PowerPoint. 16:9 widescreen format suitable for all types of screens. Includes information about fonts, colors, and credits of ...
Check out this medical PowerPoint presentation titled "Vertigo" by Dr. Abdulrahman Alsanosi.<break><break>This medical PowerPoint presentation is about vertigo, a type of dizziness or a sensation of spinning or movement, even when a person is stationary. It can be caused by problems in the inner ear, such as benign paroxysmal positional vertigo (BPPV), Menieres disease, or vestibular ...
Microsoft You can change the background to anything you like if you're using Powerpoint to create presentations: a picture, a color, a gradient, or even an in-motion video. You'll know the best ...
2. Configure settings. Go to "Settings" to set recording preferences.In "Video", choose the desired output quality and format.Make sure the toggles next to "Record mouse movements" and "Animate mouse clicks" are enabled if needed.In the "Audio" tab, adjust the sound levels and select the desired input devices.3. Record your presentation. Click the "Capture video" option in the side menu and ...
Invite collaborators: Share the presentation with your team members by sending them a link or inviting them directly through the software. Work together in real time: Once your team members have access, they can start editing the slide presentation simultaneously.Use the built-in chat and comment features to communicate and provide feedback in real time.
Presentation Transcript. VERTIGO AYESHA SHAIKH PGY2 EMORY FAMILY MEDICINE 09.17.2008. CASE • 31,female doctor, otherwise healthy, post partum week 5. • First episode, sudden feeling of room spinning, while entering patient data in computer, during Family Medicine Clinic…. One fine day last year same time!
The race to build the most compelling AI PC processors continues with the launch of Intel's Core Ultra 200V. At Computex in June, we learned these "Lunar Lake" laptop chips would feature a ...
Vertigo. Aug 11, 2014. 510 likes | 1.9k Views. To insert your company logo on this slide From the Insert Menu Select "Picture" Locate your logo file Click OK To resize the logo Click anywhere inside the logo. The boxes that appear outside the logo are known as "resize handles.". Use these to resize the object. Download Presentation.