

Burns Nursing Diagnosis and Nursing Care Plan
Last updated on July 21st, 2023 at 09:01 pm
Burns Nursing Care Plans Diagnosis and Interventions
Burns occur as a result of skin damage secondary to exposure to heat, chemicals, sunlight, electricity, or radiation.
Burns can be excruciatingly unpleasant and can be susceptible to infection if left untreated.
Classification of Burns
Types of burns, signs and symptoms of burns.
The symptoms are frequently worst in the hours or days following a burn and vary according to the extent of the burn. Symptoms of burns usually include
Causes of Burns
Risk factors to burns, complications of burns.
Third-degree burns that are deep and cover a big area of skin are extremely dangerous and can be fatal. Burns of the first and second degrees can become infected, resulting in discoloration and scarring. Scarring is not present in first-degree burns.
Diagnosis of Burns
Treatment for burns.
Burn treatment is a sensitive undertaking for any nurse to undertake and understanding the right sequencing of interventions is crucial.
Burns NCLEX Questions
Burns NCLEX Questions #3 (25 Questions)
Nursing Diagnosis for Burns
Nursing care plan for burns 1.
Desired Outcomes :
| Examine the patient’s and SO’s reactions to the loss or change, including future expectations and the impact of cultural or religious beliefs. | A traumatic event causes abrupt, unplanned changes, causing grief over actual or perceived losses. This demands assistance in order to reach a satisfactory conclusion. |
| Accept and acknowledge frustration, reliance, rage, grief, and hostility as feelings. Take note of the withdrawn manner and denial. | Accepting these feelings as a normal reaction to what has happened can help with resolution. Pushing a patient before they are ready to deal with an issue is neither helpful nor possible. Because the patient is not ready to deal with personal concerns, denial may be prolonged and serve as an adaptive mechanism. |
| Place restrictions on maladaptive behavior. While providing care, maintain a nonjudgmental attitude and assist the patient in identifying positive behaviors that will aid in recovery. | The patient and SO likely to approach this issue in the same manner they have approached previous problems. Staff may find it challenging and upsetting to deal with disruptive and unhelpful conduct, but they should keep in mind that the behavior is usually directed at the situation rather than the caregiver. |
| Be realistic and optimistic during treatments, health education, and goal-setting within constraints. | Improves patient and nurse trust and rapport. |
| Encourage the patient and SO to look at the wounds and aid with care as needed. | Encourages acceptance of the realities of injury and physical change, as well as a new self-image. |
| Provide hope within the boundaries of the unique situation; do not provide false assurance. | Encourages a good attitude and provides opportunities to create objectives and make realistic plans for the future. |
| Assist the patient in determining the extent of the real change in appearance and body function. | Assists at the beginning of the process of looking forward to the future and how life will be different. |
| Encourage positive reinforcement of progress and efforts toward achieving rehabilitative goals. | Healthy coping behaviors can be aided by words of encouragement. |
| Present photographs or videos of burn care and/or other patient outcomes, selecting what to show based on the specific situation. Encourage patients to express their feelings about what they’ve witnessed. | Allows the patient and SO to set realistic goals. Additionally, it aids in the explanation of the importance and/or necessity of specific devices and procedures. |
| Encourage engagement between family members and the rehabilitation staff. | To improve patient and family communication and provide continuing assistance. |
| Refer the patient who has been disfigured by burns to a reconstructive surgeon. | Reconstructive surgery can help patients regain their confidence and self-esteem. |
| Give the patient thorough instruction and detailed aftercare instructions. Emphasize the significance of keeping the dressing clean and dry. | Reinforcing teaching can help the patient acquire self-care. |
Nursing Care Plan for Burns 2
Desired Outcomes:
| Examine and note the size, color, and depth of the wound, as well as any necrotic tissue and the status of the surrounding skin. | Provides baseline information on the requirement for skin grafting as well as possible insights about the area’s circulation. |
| Provide proper burn treatment and infection control. | Reduces the risk of infection and graft failure by preparing tissues for transplantation. |
| If feasible, elevate the grafted area. When indicated, maintain the proper position and immobility of the region. | Tissue movement under the graft can dislodge it, preventing proper healing. |
| Maintain the following dressings over the freshly grafted area and/or donor site: mesh, petroleum, and non-adhesive. | To avoid shearing of new epithelium and protect healing tissue, translucent, nonreactive surface material can be used between the graft and the outer dressing. After covering the donor site for 4–24 hours, bulky dressings are removed and fine mesh gauze is kept in place. |
| Maintain and ensure that the patient’s skin is void of pressure. | Improves circulation and prevents ischemia, necrosis, and graft failure. |
| Examine the grafted and donor sites for color, as well as the presence or absence of healing | Examines the efficacy of circulation and looks for any possible problems. |
| After the dressings have been removed and healing has occurred, wash the sites with mild soap, rinse, and lubricate with cream several times daily. | To preserve flexibility, newly grafted skin and healed donor areas require extra attention. |
| Blebs under sheet grafts should be aspirated with a sterile needle or rolled with a sterile swab. | Fluid-filled blebs make it difficult for grafts to adhere to the underlying tissue, increasing the risk of graft failure. |
Nursing Care Plan for Burns 3
| Frequently note digit circulation, motion, and feeling. | Edema can impair circulation to the extremities, increasing the risk of tissue necrosis and contractures. |
| On admittance, begin the rehabilitation phase. | When the patient is aware of the potential for recovery, it is easier to enlist their help. |
| Use supports or splints to keep the patient’s body aligned, especially if they have burns over joints. | Promotes functional extremity alignment and avoids contractures, which are more common over joints. |
| Perform ROM exercises on a regular basis, first passively and later actively. | This prevents the tightening of scar tissue and contractures as time progresses. This can also enhance muscle and joint function and decreases calcium sequestration from the bones. |
| Before engaging in any activity or exercise, take pain medication. | This allows the patient to be more active and participative by reducing muscle tension and tissue stiffness. |
| Treatments and care tasks should be scheduled to provide for uninterrupted rest intervals. | Increases the patient’s strength and exercise tolerance. |
| Encourage family and SO involvement in ROM exercises. | Allows family/SO to participate in patient care, resulting in more consistent therapy. |
| Physical therapy, hydrotherapy, and nursing care should all be incorporated into ADLs. | Combining activities improves outcomes by amplifying the effects of each. |
| Encourage patients to participate in as many activities as they are capable of. | Encourages independence, boosts self-esteem, and speeds up the rehabilitation process. |
Nursing Care Plan for Burns 4
Desired Outcome: The patient will achieve timely wound healing as manifested by the absence of purulent exudate and fever.
| Examine wounds on a daily basis, taking note of any changes in look, odor, or discharge volume. | Sepsis indicators, which frequently arise with full-thickness burns, require immediate investigation and treatment. Sensorium, bowel habits, and respiratory rate changes frequently precede fever and laboratory study changes. |
| Unburned areas (such as the groin, neck creases, and mucous membranes) and vaginal discharge should be checked on a regular basis. | Drainage from nearby burns may cause eyes to swell shut and/or become infected. Eye coverings may be required if the lids are burned, to avoid corneal injury. |
| Fever, increased breathing rate and depth in combination with changes in sensorium, diarrhea, low platelet count, and hyperglycemia with glycosuria should all be monitored. | Water softens, making it easier to remove dressings and eschar (slough layer of dead skin or tissue). Whether to take a bath or shower depends on the source. Bathing has the benefit of giving support for exercising extremities, but it may also cause wound cross-contamination. Showering improves wound examination and keeps floating debris from contaminating the wound. |
| Implement the recommended isolation techniques. | Isolation may range from simple wound and/or skin to complete or reverse to limit the danger of cross-contamination and exposure to multiple bacterial flora, depending on the type or size of wounds and the wound treatment (open versus closed). |
| Instruct and demonstrate proper handwashing for all individuals who come into touch with the patient. | To prevent cross-contamination and lowers the risk of illness. |
| During direct wound care, use gowns, gloves, masks, and rigorous aseptic technique, and give sterile or newly laundered bed sheets or gowns. | To protect against infectious germs. |
| If necessary, keep track of and/or limit visitors. Explain the isolation technique to visitors if it is used. Ensure that visitors follow the protocol as directed. | Cross-contamination from visitors is avoided. The patient’s need for family support and socializing should be balanced against the risk of infection. |
| Including a 1-inch perimeter, shave or trim any hair from around burned areas (excluding eyebrows). Men should shave their beards and shampoo their heads every day. | During systemic antibiotic therapy, opportunistic infections (yeast) are common due to immune system suppression and/or growth of normal body flora. |
| Eyes require extra attention, so wear eye coverings and tear solutions as needed. | Prevents adhesion to any surfaces it may come into contact with and promotes appropriate healing. It’s worth noting that ear cartilage has poor circulation and is susceptible to pressure necrosis. |
| Avoid skin-to-skin contact on the surface (wrap each burned finger or toe separately; do not allow burned ear to touch scalp). | Provides early diagnosis of burn-wound infection by detecting the presence of healing (granulation tissue). Infection can cause a partial-thickness burn to become a full-thickness damage. Pseudomonas is identified by a distinct sweet, musty odor at the graft site. |
| In a hydrotherapy or whirlpool tub, or in a shower stall with a handheld shower head, remove dressings and cleanse burned areas. Maintain a temperature of 100°F (37.8°C) in the water. Use a gentle washing agent or surgical soap to clean the affected regions. | Early excision is known to lessen scarring and infection risk, allowing for faster recovery. |
| With scissors and forceps, remove necrotic or loose tissue (including ruptured blisters). If the blisters are smaller than 12 cm, do not interfere with joint function, and do not appear infectious, do not touch them. | To promote recovery. Autocontamination is avoided. Unless the burn injury is caused by chemicals, small, intact blisters can preserve the skin and enhance the process of re-epithelialization (in which case fluid contained in blisters may continue to cause tissue destruction). |
| Photograph the wound at first and thereafter at regular intervals. | To establish a baseline and records the healing process. |
| Topical agents should be used as directed. | Topical agents aid in bacterial control and wound drying, which can lead to additional tissue loss. |
| Other treatments should be given as needed: subeschar clysis or systemic antibiotics; tetanus toxoid or clostridial antitoxin, if needed. | Tissue loss and weakened defense mechanisms raise the risk of tetanus or gas , particularly in serious burns produced by electricity. |
| In the non-burned area, place IV and/or invasive lines. | Reduced risk of infection at the insertion site, with the potential for septicemia. |
| Obtain routine wound cultures and/or drainage sensitivity. | To allow for the early detection and treatment of wound infections. |
Nursing Care Plan for Burns 5
| Examine the patient’s condition, prognosis, and future prospects. | Provides a knowledge base for patients to make well-informed decisions. |
| Discuss the patient’s expectations for returning to his or her home, work, and normal activities. | Following discharge, patients usually experience a tough and lengthy adjustment period. Sleep disturbances, nightmares, reliving the event, trouble resuming social interactions, intimacy and sexual activity, emotional lability are all common problems that obstruct successful return of regular life. |
| Review and demonstrate proper burn, skin-graft, and wound care practices to the patient/SO. Determine the best outpatient care and supply options. | After discharge, encourages effective self-care and independence. |
| Talk about skin care. Teach how to apply moisturizers, sunscreens, and anti-itch drugs correctly. | Itching, blistering, and sensitivity of healing wounds or graft sites can last a long time, and harm might occur due to the new tissue’s fragility. |
| Examine drugs for their intended use, dose, mode of administration, and predicted and/or reportable side effects. | Reiteration helps the patient to raise questions and confirm that their information is correct. |
| Explain the scarring process, as well as the need for the proper application of pressure garments when they are required. | Promotes healthy skin renewal while reducing hypertrophic scars and contractures and speeding up the healing process. Note: Long-term use of the pressure garment can lessen the need for reconstructive surgery to remove scars and release contractures. |
| Encourage the patient to adhere to the planned workout routine and relaxation times. | Maintains mobility, decreases problems, and prevents weariness, allowing for a quicker recovery. |
| Individually appropriate activity constraints should be identified. | Restrictions are imposed based on the degree and location of the injury, as well as the stage of recovery. |
| Stress the necessity of eating high-protein, high-calorie meals and snacks on a regular basis. | Optimal diet promotes tissue repair and overall happiness. Note: To meet calorie and protein requirements for recovery, patients frequently need to increase their caloric intake. |
Nursing References
Ignatavicius, D. D., Workman, M. L., Rebar, C. R., & Heimgartner, N. M. (2020). Medical-surgical nursing: Concepts for interprofessional collaborative care . St. Louis, MO: Elsevier. Buy on Amazon
Disclaimer:
The medical information on this site is provided as an information resource only and is not to be used or relied on for any diagnostic or treatment purposes.
This information is intended to be nursing education and should not be used as a substitute for professional diagnosis and treatment.
Leave a Comment Cancel reply
VIDEO LIBRARY
Nursing Care Plan For Burns
Introduction:.
A nursing care plan for burns is a crucial component of comprehensive burn management. Burns can result from various sources, such as thermal, electrical, or chemical injuries, and can vary in severity from minor to life-threatening. The nursing care plan for burns focuses on providing holistic care that addresses the physical, emotional, and psycho-social needs of the patient throughout their recovery journey. The primary goal of the nursing care plan for burns is to promote wound healing, prevent complications, alleviate pain, and support the patient’s overall well-being. This care plan involves a collaborative approach, where nurses work closely with the healthcare team, including physicians, wound care specialists, physical therapists, and psychologists, to ensure coordinated and effective care.
In the initial stages of burn care, the nursing care plan emphasizes the assessment and stabilization of the patient’s condition. This includes a comprehensive assessment of the burn injury, determination of burn depth and extent, assessment of associated injuries, and evaluation of vital signs and fluid balance. This assessment serves as the foundation for developing individualized nursing diagnoses and interventions.
The nursing care plan for burns is dynamic and requires ongoing assessment, evaluation, and adjustment based on the patient’s progress and changing needs. By providing individualized care, fostering a therapeutic relationship, and advocating for the patient, nurses play a crucial role in promoting optimal outcomes and facilitating the patient’s recovery and rehabilitation process.
Nursing Assessment for Burn:
A comprehensive nursing assessment is vital in determining the extent and severity of a burn injury and guiding the development of an individualized care plan. The assessment should encompass a systematic gathering of subjective and objective data to evaluate the patient’s physical and psychosocial well-being. Below is a plagiarism-free outline of the nursing assessment for the burn:
Initial Assessment:
- Evaluate the patient’s airway, breathing, and circulation (ABCs) to ensure adequate oxygenation and perfusion.
- Assess the patient’s level of consciousness and mental status.
- Determine the mechanism and cause of the burn injury, noting any associated injuries or trauma.
- Obtain a detailed history of the burn, including the source, duration, and circumstances surrounding the injury.
Physical Assessment:
- Perform a thorough head-to-toe examination to assess the extent and depth of the burn injury.
- Identify the location and size of the burn, using the “Rule of Nines” or Lund and Browder chart to estimate the total body surface area (TBSA) affected.
- Assess the burn wound characteristics, including color, texture, blistering, eschar formation, and presence of any foreign objects.
- Evaluate the peripheral pulses, capillary refill, and skin temperature to assess the circulation to the affected area.
- Assess for associated injuries, such as fractures, lacerations, or inhalation injuries.
Pain Assessment:
- Use a validated pain assessment scale to evaluate the intensity and characteristics of the patient’s pain.
- Assess the patient’s verbal and non-verbal cues of pain, such as facial expressions, restlessness, guarding, or increased heart rate.
- Determine the effectiveness of pain management interventions and reassess pain regularly.
Fluid and Electrolyte Assessment:
- Monitor vital signs, including blood pressure, heart rate, and urine output, to assess the patient’s hemodynamic stability.
- Assess for signs of fluid imbalance, such as hypovolemia, tachycardia, hypotension, or oliguria.
- Evaluate laboratory values, including electrolyte levels and serum albumin, to identify any imbalances and guide fluid replacement therapy.
Psychosocial Assessment:
- Assess the patient’s emotional and psychological well-being, including their response to the burn injury and their coping mechanisms
- Evaluate the patient’s support system, including family, friends, or other available resources.
- Identify any pre-existing psychological conditions or risk factors that may impact the patient’s psychological adjustment.
Risk Assessment:
- Assess for potential complications associated with burn injuries, such as infection, inhalation injury, compartment syndrome, or hypothermia.
- Identify risk factors that may impact wound healing and recovery, such as diabetes, immunosuppression, or peripheral vascular disease.
Remember, when conducting a nursing assessment for burns, it is essential to document findings accurately, communicate effectively with the healthcare team, and update the assessment regularly to monitor changes in the patient’s condition. Additionally, incorporating your own clinical knowledge and expertise while adhering to ethical guidelines for academic integrity is crucial when utilizing this information for your nursing care plan.
Nursing Diagnosis for Burn:
Nursing diagnoses for patients with burn injuries are essential for identifying their specific needs and providing individualized care. The following nursing diagnoses are plagiarism-free examples that can guide the development of a comprehensive care plan for burn patients:
Impaired Skin Integrity :
Related to Loss of Skin Barrier Secondary to Burn Injury:
This nursing diagnosis addresses the compromised skin integrity resulting from the burn injury. Assessment findings may include erythema, blistering, open wounds, or eschar formation.
Acute Pain :
Related to Thermal Injury and Tissue Inflammation:
This nursing diagnosis recognizes the patient’s experience of pain resulting from the burn injury. Assessment findings may include reports of pain, increased heart rate, facial grimacing, or guarding behaviors.
Risk for Infection :
Related to Compromised Skin Barrier and Invasive Procedures:
This nursing diagnosis identifies the patient’s vulnerability to infection due to the loss of the protective skin barrier and invasive procedures such as wound debridement or insertion of invasive devices.
Impaired Gas Exchange :
Related to Inhalation Injury or Circumferential Burns:
. This nursing diagnosis reflects the patient’s impaired ability to exchange oxygen and carbon dioxide effectively due to inhalation injury or the restriction of chest expansion caused by circumferential burns.
Disturbed Body Image :
Related to Changes in Physical Appearance and Visible Scars:
This nursing diagnosis addresses the patient’s emotional response to changes in physical appearance and the presence of visible scars resulting from the burn injury.
Remember, nursing diagnoses should be individualized to each patient’s unique situation, and the provided examples should be adapted to align with the specific assessment findings of your patient. Additionally, incorporating evidence-based interventions and collaborating with the healthcare team will contribute to the development of an effective and personalized care plan for burn patients.
Nursing Interventions for Burn:
Nursing interventions for burn patients are aimed at promoting wound healing, preventing complications, managing pain, facilitating psychological adjustment, and supporting overall well-being. These interventions should be evidence-based, individualized, and tailored to the specific needs of each patient. Here are plagiarism-free examples of nursing interventions for burns:
Wound Care Management:
- Follow appropriate sterile technique during wound dressing changes to prevent infection.
- Cleanse the burn wounds using prescribed solutions or sterile saline.
- Apply appropriate dressings based on the type and depth of the burn, such as non-adherent dressings, hydrogels, or antimicrobial dressings.
- Monitor and document the appearance of the wound, including signs of infection, healing progression, or complications.
Pain Management:
- Administer prescribed analgesics promptly and regularly to control pain.
- Utilize non-pharmacological pain management techniques, such as distraction, relaxation techniques, or guided imagery.
- Position the patient in a comfortable position that reduces pressure on the burn wounds.
- Implement cold therapy or administer topical analgesics as ordered to provide localized pain relief.
Fluid and Electrolyte Balance:
- Monitor the patient’s fluid intake and output closely to assess for signs of inadequate hydration or fluid overload.
- Administer intravenous fluids as prescribed to maintain fluid balance and replace fluid losses.
- Monitor electrolyte levels regularly and collaborate with the healthcare team to address any imbalances.
Collaborate with the Healthcare Team:
- Communicate effectively with physicians, wound care specialists, physical therapists, and other members of the healthcare team.
- Participate in interdisciplinary rounds or meetings to discuss the patient’s progress, treatment plan, and potential adjustments.
- Coordinate with the team to ensure continuity of care, appropriate wound care techniques, and timely interventions.
Remember, these nursing interventions should be adapted and tailored to the individual patient’s needs and preferences. Additionally, staying up to date with current evidence and guidelines is crucial in providing optimal care for burn patients.
Conclusion:
In conclusion, the nursing care plan for burn patients focuses on providing comprehensive care that addresses the physical, emotional, and psychosocial needs of the individual. Through the implementation of evidence-based nursing interventions, nurses play a crucial role in promoting wound healing, preventing complications, managing pain, facilitating psychological adjustment, and supporting overall well-being.
The nursing care plan for burns begins with a thorough assessment to determine the extent and severity of the burn injury. This assessment serves as the foundation for developing individualized nursing diagnoses and interventions that guide the care provided to the patient. Wound care management is a fundamental aspect of the nursing care plan for burns. By following sterile techniques, cleansing the burn wounds, and applying appropriate dressings, nurses promote healing and reduce the risk of infection. Pain management interventions, including the administration of analgesics, non-pharmacological techniques, and positioning, help alleviate the patient’s discomfort and improve their quality of life. Psychosocial support is a crucial component of the nursing care plan for burns, recognizing the emotional impact of the burn injury on the patient. Nurses provide a therapeutic environment, offer emotional support, and facilitate access to counseling or support groups to assist with the patient’s psychological adjustment and overall well-being.
In conclusion, the nursing care plan for burns aims to provide holistic care that encompasses physical, emotional, and psychosocial well-being. By implementing evidence-based interventions, advocating for the patient, and fostering a therapeutic relationship, nurses contribute significantly to the patient’s recovery, rehabilitation, and successful reintegration into their daily lives.
burn prevention nursing interventions burns nursing care technique burns nursing diagnosis burns nursing interventions burns nursing management nursing care plan for burn pain nursing care plan for burn patient pdf nursing care plan for burns pdf nursing care plan for burns scribd nursing care plan for burns slideshare
Leave a Reply
Your email address will not be published. Required fields are marked *
- Exploring Retroviruses: Nature’s Intriguing Genetic Hackers
- Orthomyxoviridae: The Viral Family Behind Influenza
- Adenoviruses: Understanding a Common Yet Complex Virus
- Understanding Norovirus: The Stomach Bug
- The Varicellovirus: Insights into a Viral Master of Stealth and Symptomatology
TERMS OF SERVICE
PRIVACY POLICY
Made For Medical
Copyrights © 2024. All rights reserved.
🌟Calling all Doctors, Nurses, and Physician Assistants! 🩺✨
🚀Supercharge your medical knowledge with our exclusive video lectures tailored for YOU!! 🚀 Unlock expert insights, earn FREE CME/CE credits, and learn at your own pace! 📚💡
Burns Nursing Care Plan & Management
Description.
- Burns are caused by a transfer of energy from a heat source to the body. The depth of the injury depends on the temperature of the burning agent and the duration of contact with it.
- Burns disrupt the skin, which leads to increased fluid loss; infection; hypothermia; scarring; compromised immunity; and changes in function, appearance, and body image. Young children and the elderly continue to have increased morbidity and mortality when compared to other age groups with similar injuries. Inhalation injuries in addition to cutaneous burns worsen the prognosis.
Characteristics of Burn
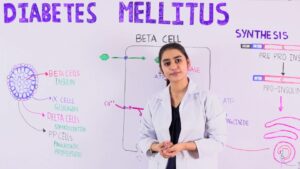
- Superficial partialthickness burns (similar to firstdegree), such as sunburn: The epidermis and possibly a portion of the dermis are destroyed.
- Deep partialthickness burns (similar to seconddegree), such as a scald: The epidermis and upper to deeper portions of the dermis are injured.
- Fullthickness burns (thirddegree), such as a burn from a flame or electric current: The epidermis, entire dermis, and sometimes the underlying tissue, muscle, and bone are destroyed.
Extent of Body Surface Area Burned
How much total body surface area is burned is determined by one of the following methods:
- Lund and Browder method: a more precise method of estimating the extent of the burn; takes into account that the percentage of the surface area represented by various anatomic parts (head and legs) changes with growth.
- Palm method: used to estimate percentage of scattered burns, using the size of the patient’s palm (about 1% of body surface area) to assess the extent of burn injury.
Most burns result from preventable accidents. Thermal burns, which are the most common type,occur because of fires from motor vehicle crashes, accidents in residences, and arson or electrical malfunctions. Children may be burned when they play with matches or firecrackers or because of a kitchen accident. Chemical burns occur as a result of contact with, ingestion of, or inhalation of acids, alkalis, or vesicants (blistering gases). The percentage of burns actually caused by abuse is fairly small, but they are some of the most difficult to manage. Neglect or inadequate supervision of children is fairly common. Effective prevention and educational efforts such as smoke detectors, flame-retardant clothing, child-resistant cigarette lighters, and the Stop Drop and Roll program have decreased the number and severity of injuries.
Gender, Ethnic/Racial, and Life Span Considerations
Preschool children account for over two-thirds of all burn fatalities. Clinicians use a special chart (Lund-Browder Chart) for children that provides a picture and a graph to account for the difference in body surface area by age. Serious burn injuries occur most commonly in males, and in particular, young adult males ages 20 to 29 years of age, followed by children under 9 years of age. Individuals older than 50 years sustain the fewest number of serious burn injuries.
The younger child is the most common victim of burns that have been caused by liquids. Preschoolers, school-aged children, and teenagers are more frequently the victims of flame burns. Young children playing with lighters or matches are at risk, as are teenagers because of carelessness or risk-taking behaviors around fires. Toddlers incur electrical burns from biting electrical cords or putting objects in outlets.
Most adults are victims of house fires or workrelated accidents that involve chemicals or electricity. The elderly are also prone to scald injuries because their skin tends to be extremely thin and sensitive to heat.
Because of the severe impact of this injury, the very young and the very old are less able to respond to therapy and have a higher incidence of mortality. In addition, when a child Burns 167 experiences a burn, multiple surgeries are required to release contractures that occur as normal growth pulls at the scar tissue of their healed burns. Adolescents are particularly prone to psychological difficulties because of sensitivity regarding body image issues. No specific gender and ethnic/racial considerations exist in burns.
Gerontologic Considerations
- Elderly people are at higher risk for burn injury because of reduced coordination, strength, and sensation and changes in vision.
- Predisposing factors and the health history in the older adult influence the complexity of care for the patient.
- Pulmonary function is limited in the older adult and therefore airway exchange, lung elasticity, and ventilation can be affected.
- This can be further affected by a history of smoking.
- Decreased cardiac function and coronary artery disease increase the risk of complications in elderly patients with burn injuries. Malnutrition and presence of diabetes mellitus orother endocrine disorders present nutritional challenges and require close monitoring.
- Varying degrees of orientation may present themselves on admission or through the course of care making assessment of pain and anxiety a challenge for the burn team.
- The skin of the elderly is thinner and less elastic, which affects the depth of injury and its ability to heal.
Primary Nursing Diagnosis
Ineffective airway clearance related to airway edema
OUTCOMES. Respiratory status: Gas exchange; Respiratory status: Ventilation; Symptom control behavior; Treatment behavior: Illness or injury; Comfort level INTERVENTIONS. Airway management; Anxiety reduction; Oxygen therapy; Airway suctioning; Airway insertion and stabilization; Cough enhancement; Mechanical ventilation; Positioning; Respiratory monitoring
Medical Management
MINOR BURN CARE . Minor burn wounds are cared for by using the principles of comfort, cleanliness, and infection control. A gentle cleansing of the wound with soap and water 2 or 3 times a day, followed with a topical agent such as silver sulfadiazine or mafenide, prevents infection. Minor burns should heal in 7 to 10 days; however, if they take longer than 14 days, excision of the wound and a small graft may be needed. Oral analgesics may be prescribed to manage discomfort, and as do all burn patients, the patient needs to receive tetanus toxoid to prevent infection.
MAJOR BURN CARE . For patients with a major injury, effective treatment is provided by a multidisciplinary team with special training in burn care. In addition to the physician and nurse, the team includes specialists in physical and occupational therapy, respiratory therapy, social work, nutrition, psychology, and child life for children. The course of recovery is divided into four phases: emergent-resuscitative, acute-wound coverage, convalescent-rehabilitative, and reorganization-reintegration.
The emergent-resuscitative phase lasts from 48 to 72 hours after injury or until diuresis takes place. In addition to managing airway, breathing, and circulation, the patient receives fluid resuscitation, maintenance of electrolytes, aggressive pain management, and early nutrition.Wounds are cleansed with chlorhexidine gluconate and care consists of silver sulfadiazine ormafenide and surgical management as needed. To prevent infection, continued care includes further débridement by washing the surface of the wounds with mild soap or aseptic solutions. Then the physician débrides devitalized tissue, and often the wound is covered with antibacterial agents such as silver sulfadiazine and occlusive cotton gauze.
The acute-wound coverage phase, which varies depending on the extent of injury, lasts until the wounds have been covered, through either the normal healing process or grafting. The risk for infection is high during this phase; the physician follows wound and blood cultures and prescribes antibiotics as needed. Wound management includes excision of devitalized tissue, surgical grafting of donor skin, or placement of synthetic membranes. Inpatient rehabilitation takes place during the convalescent-rehabilitative phase. Although principles of rehabilitation are included in the plan of care from the day of admission, during this time, home exercises and wound care are taught. In addition, pressure appliances to reduce scarring, or braces to prevent contractures, are fitted. The reorganization phase is the long period of time that it may take after the injury for physical and emotional healing to take place.
Nursing Management: Emergent/Resuscitative Phase
- Focus on the major priorities of any trauma patient; the burn wound is a secondary consideration, although aseptic management of the burn wounds and invasive lines continues.
- Assess circumstances surrounding the injury: time of injury, mechanism of burn, whether the burn occurred in a closed space, the possibility of inhalation of noxious chemicals, and any related trauma.
- Monitor vital signs frequently; monitor respiratory status closely; and evaluate apical, carotid, and femoral pulses particularly in areas of circumferential burn injury to an extremity.
- Start cardiac monitoring if indicated (eg, history of cardiac or respiratory problems, electrical injury).
- Check peripheral pulses on burned extremities hourly; use Doppler as needed.
- Monitor fluid intake (IV fluids) and output (urinary catheter) and measure hourly. Note amount of urine obtained when catheter is inserted (indicates preburn renal function and fluid status).
- Assess body temperature, body weight, history of preburn weight, allergies, tetanus immunization, past medicalsurgical problems, current illnesses, and use of medications.
- Arrange for patients with facial burns to be assessed for corneal injury.
- Continue to assess the extent of the burn; assess depth of wound, and identify areas of full and partialthickness injury.
- Assess neurologic status: consciousness, psychological status, pain and anxiety levels, and behavior.
- Assess patient’s and family’s understanding of injury and treatment. Assess patient’s support system and coping skills.
Interventions
Promoting Gas Exchange and Airway Clearance
- Provide humidified oxygen, and monitor arterial blood gases (ABGs), pulse oximetry, and carboxyhemoglobin levels.
- Assess breath sounds and respiratory rate, rhythm, depth, and symmetry; monitor for hypoxia.
- Observe for signs of inhalation injury: blistering of lips or buccal mucosa; singed nostrils; burns of face, neck, or chest; increasing hoarseness; or soot in sputum or respiratory secretions.
- Report labored respirations, decreased depth of respirations, or signs of hypoxia to physician immediately; prepare to assist with intubation and escharotomies.
- Monitor mechanically ventilated patient closely.
- Institute aggressive pulmonary care measures: turning, coughing, deep breathing, periodic forceful inspiration using spirometry, and tracheal suctioning.
- Maintain proper positioning to promote removal of secretions and patent airway and to promote optimal chest expansion; use artificial airway as needed.
Restoring Fluid and Electrolyte Balance
- Monitor vital signs and urinary output (hourly), central venous pressure (CVP), pulmonary artery pressure, and cardiac output.
- Note and report signs of hypovolemia or fluid overload.
- Maintain IV lines and regular fluids at appropriate rates, as prescribed. Document intake, output, and daily weight.
- Elevate the head of bed and burned extremities.
- Monitor serum electrolyte levels (eg, sodium, potassium, calcium, phosphorus, bicarbonate); recognize developing electrolyte imbalances.
- Notify physician immediately of decreased urine output; blood pressure; central venous, pulmonary artery, or pulmonary artery wedge pressures; or increased pulse rate.
Maintaining Normal Body Temperature
- Provide warm environment: use heat shield, space blanket, heat lights, or blankets.
- Assess core body temperature frequently.
- Work quickly when wounds must be exposed to minimize heat loss from the wound.
Minimizing Pain and Anxiety
- Use a pain scale to assess pain level (ie, 1 to 10); differentiate between restlessness due to pain and restlessness due to hypoxia.
- Administer IV opioid analgesics as prescribed, and assess response to medication; observe for respiratory depression in patient who is not mechanically ventilated.
- Provide emotional support, reassurance, and simple explanations about procedures.
- Assess patient and family understanding of burn injury, coping strategies, family dynamics, and anxiety levels. Provide individualized responses to support patient and family coping; explain all procedures in clear, simple terms.
- Provide pain relief, and give antianxiety medications if patient remains highly anxious and agitated after psychological interventions.
Monitoring and Managing Potential Complications
- Acute respiratory failure: Assess for increasing dyspnea, stridor, changes in respiratory patterns; monitor pulse oximetry and ABG values to detect problematic oxygen saturation and increasing CO2; monitor chest xrays; assess for cerebral hypoxia (eg, restlessness, confusion); report deteriorating
- respiratory status immediately to physician; and assist as needed with intubation or escharotomy.
- Distributive shock: Monitor for early signs of shock (decreased urine output, cardiac output, pulmonary artery pressure, pulmonary capillary wedge pressure, blood pressure, or increasing pulse) or progressive edema. Administer fluid resuscitation as ordered in response to physical findings; continue monitoring fluid status.
- Acute renal failure: Monitor and report abnormal urine output and quality, blood urea nitrogen (BUN) and creatinine levels; assess for urine hemoglobin or myoglobin; administer increased fluids as prescribed.
- Compartment syndrome: Assess peripheral pulses hourly with Doppler; assess neurovascular status of extremities hourly (warmth, capillary refill, sensation, and movement); remove blood pressure cuff after each reading; elevate burned extremities; report any extremity pain, loss of peripheral pulses or sensation; prepare to assist with escharotomies.
- Paralytic ileus: Maintain nasogastric tube on low intermittent suction until bowel sounds resume; auscultate abdomen regularly for distention and bowel sounds.
- Curling’s ulcer: Assess gastric aspirate for blood and pH; assess stools for occult blood; administer antacids and histamine blockers (eg, ranitidine [Zantac]) as prescribed.
Nursing Management: Acute/ Intermediate Phase
The acute or intermediate phase begins 48 to 72 hours after the burn injury. Burn wound care and pain control are priorities at this stage.
- Focus on hemodynamic alterations, wound healing, pain and psychosocial responses, and early detection of complications.
- Measure vital signs frequently; respiratory and fluid status remains highest priority.
- Assess peripheral pulses frequently for first few days after the burn for restricted blood flow.
- Closely observe hourly fluid intake and urinary output, as well as blood pressure and cardiac rhythm; changes should be reported to the burn surgeon promptly.
- For patient with inhalation injury, regularly monitor level of consciousness, pulmonary function, and ability to ventilate; if patient is intubated and placed on a ventilator, frequent suctioning and assessment of the airway are priorities.
Restoring Normal Fluid Balance
- Monitor IV and oral fluid intake; use IV infusion pumps.
- Measure intake and output and daily weight.
- Report changes (eg, blood pressure, pulse rate) to physician.
Preventing Infection
- Provide a clean and safe environment; protect patient from sources of crosscontamination (eg, visitors, other patients, staff, equipment).
- Closely scrutinize wound to detect early signs of infection.
Monitor culture results and white blood cell counts.
- Practice clean technique for wound care procedures and aseptic technique for any invasive procedures. Use meticulous hand hygiene before and after contact with patient.
- Caution patient to avoid touching wounds or dressings; wash unburned areas and change linens regularly.
Maintaining Adequate Nutrition
- Initiate oral fluids slowly when bowel sounds resume; record tolerance—if vomiting and distention do not occur, fluids
- may be increased gradually and the patient may be advanced to a normal diet or to tube feedings.
- Collaborate with dietitian to plan a protein and calorie-rich diet acceptable to patient. Encourage family to bring nutritious and patient’s favorite foods. Provide nutritional and vitamin and mineral supplements if prescribed.
- Document caloric intake. Insert feeding tube if caloric goals cannot be met by oral feeding (for continuous or bolus feedings); note residual volumes.
- Weigh patient daily and graph weights.
Promoting Skin Integrity
- Assess wound status.
- Support patient during distressing and painful wound care.
- Coordinate complex aspects of wound care and dressing changes.
- Assess burn for size, color, odor, eschar, exudate, epithelial buds (small pearllike clusters of cells on the wound surface), bleeding, granulation tissue, the status of graft take, healing of the donor site, and the condition of the surrounding skin; report any significant changes to the physician.
- Inform all members of the health care team of latest wound care procedures in use for the patient.
- Assist, instruct, support, and encourage patient and family to take part in dressing changes and wound care.
- Early on, assess strengths of patient and family in preparing for discharge and home care.
Relieving Pain and Discomfort
- Frequently assess pain and discomfort; administer analgesic agents and anxiolytic medications, as prescribed, before the pain becomes severe. Assess and document the patient’s response to medication and any other interventions.
- Teach patient relaxation techniques. Give some control over wound care and analgesia. Provide frequent reassurance.
- Use guided imagery and distraction to alter patient’s perceptions and responses to pain; hypnosis, music therapy, and virtual reality are also useful.
- Assess the patient’s sleep patterns daily; administer sedatives, if prescribed.
- Work quickly to complete treatments and dressing changes.
Encourage patient to use analgesic medications before painful procedures.
- Promote comfort during healing phase with the following:
- oral antipruritic agents, a cool environment, frequent lubrication of the skin with water or a silicabased lotion, exercise and splinting to prevent skin contracture, and diversional activities.
Promoting Physical Mobility
- Prevent complications of immobility (atelectasis, pneumonia, edema, pressure ulcers, and contractures) by deep breathing, turning, and proper repositioning.
- Modify interventions to meet patient’s needs. Encourage early sitting and ambulation. When legs are involved, apply elastic pressure bandages before assisting patient to upright position.
- Make aggressive efforts to prevent contractures and hypertrophic scarring of the wound area after wound closure for a year or more.
- Initiate passive and active range-of-motion exercises from admission until after grafting, within prescribed limitations.
- Apply splints or functional devices to extremities for contracture control; monitor for signs of vascular insufficiency, nerve compression, and skin breakdown.
Strengthening Coping Strategies
- Assist patient to develop effective coping strategies: Set specific expectations for behavior, promote truthful communication to build trust, help patient practice coping strategies, and give positive reinforcement when appropriate.
- Demonstrate acceptance of patient. Enlist a noninvolved person for patient to vent feelings without fear of retaliation.
- Include patient in decisions regarding care. Encourage patient to assert individuality and preferences. Set realistic expectations for selfcare.
Supporting Patient and Family Processes
- Support and address the verbal and nonverbal concerns of the patient and family.
- Instruct family in ways to support patient.
- Make psychological or social work referrals as needed.
- Provide information about burn care and expected course of treatment.
- Initiate patient and family education during burn management. Assess and consider preferred learning styles; assess ability to grasp and cope with the information; determine barriers to learning when planning and executing teaching.
- Remain sensitive to the possibility of changing family dynamics.
- Heart failure: Assess for fluid overload, decreased cardiac output, oliguria, jugular vein distention, edema, or onset of S3 or S4 heart sounds.
- Pulmonary edema: Assess for increasing CVP, pulmonary artery and wedge pressures, and crackles; report promptly. Position comfortably with head elevated unless contraindicated. Administer medications and oxygen as prescribed and assess response.
- Sepsis: Assess for increased temperature, increased pulse, widened pulse pressure, and flushed, dry skin in unburned areas (early signs), and note trends in the data. Perform wound and blood cultures as prescribed. Give scheduled antibiotics on time.
- Acute respiratory failure and acute respiratory distress syndrome (ARDS): Monitor respiratory status for dyspnea, change in respiratory pattern, and onset of adventitious sounds. Assess for decrease in tidal volume and lung compliance in patients on mechanical ventilation. The hallmark of onset of ARDS is hypoxemia on 100% oxygen, decreased lung compliance, and significant shunting; notify physician of deteriorating respiratory status.
- Visceral damage (from electrical burns): Monitor electrocardiogram (ECG) and report dysrhythmias; pay attention to pain related to deep muscle ischemia and report. Early detection may minimize severity of this complication. Fasciotomies may be necessary to relieve swelling and ischemia in the muscles and fascia; monitor patient for excessive blood loss and hypovolemia after fasciotomy.
Nursing Process: Rehabilitation Phase
Rehabilitation should begin immediately after the burn has occurred. Wound healing, psychosocial support, and restoring maximum functional activity remain priorities. Maintaining fluid and electrolyte balance and improving nutrition status continue to be important.
- In early assessment, obtain information about patient’s educational level, occupation, leisure activities, cultural background, religion, and family interactions.
- Assess selfconcept, mental status, emotional response to the injury and hospitalization, level of intellectual functioning, previous hospitalizations, response to pain and pain relief measures, and sleep pattern.
- Perform ongoing assessments relative to rehabilitation goals, including range of motion of affected joints, functional abilities in ADLs, early signs of skin breakdown from splints or positioning devices, evidence of neuropathies (neurologic damage), activity tolerance, and quality or condition of healing skin.
- Document participation and selfcare abilities in ambulation, eating, wound cleaning, and applying pressure wraps.
- Maintain comprehensive and continuous assessment for early detection of complications, with specific assessments as needed for specific treatments, such as postoperative assessment of patient undergoing primary excision.
Nursing Diagnoses
- Activity intolerance related to pain on exercise, limited joint mobility, muscle wasting, and limited endurance
- Disturbed body image related to altered appearance and selfconcept
- Deficient knowledge of postdischarge home care and recovery needs
Collaborative Problems/Potential Complications
- Contractures
- Inadequate psychological adaptation to burn injury
Planning and Goals
- Goals include increased participation in ADLs; increased understanding of the injury, treatment, and planned followup care; adaptation and adjustment to alterations in body image, selfconcept, and lifestyle; and absence of complications.
Nursing Interventions
Promoting Activity Tolerance
- Schedule care to allow periods of uninterrupted sleep. Administer hypnotic agents, as prescribed, to promote sleep.
- Communicate plan of care to family and other caregivers.
- Reduce metabolic stress by relieving pain, preventing chilling or fever, and promoting integrity of all body systems to help conserve energy. Monitor fatigue, pain, and fever to determine amount of activity to be encouraged daily.
- Incorporate physical therapy exercises to prevent muscular atrophy and maintain mobility required for daily activities.
- Support positive outlook, and increase tolerance for activity by scheduling diversion activities in periods of increasing duration.
Improving Body Image and Self-Concept
- Take time to listen to patient’s concerns and provide realistic support; refer patient to a support group to develop coping strategies to deal with losses.
- Assess patient’s psychosocial reactions; provide support and develop a plan to help the patient handle feelings.
- Promote a healthy body image and selfconcept by helping patient practice responses to people who stare or ask about the injury.
- Support patient through small gestures such as providing a birthday cake, combing patient’s hair before visitors, and sharing information on cosmetic resources to enhance appearance.
- Teach patient ways to direct attention away from a disfigured body to the self within.
- Coordinate communications of consultants, such as psychologists, social workers, vocational counselors, and teachers, during rehabilitation.
- Contractures: Provide early and aggressive physical and occupational therapy; support patient if surgery is needed to achieve full range of motion.
- Impaired psychological adaptation to the burn injury:
- Obtain psychological or psychiatric referral as soon as evidence of major coping problems appears.
Teaching Self-care
- Throughout the phases of burn care, make efforts to prepare patient and family for the care they will perform at home. Instruct them about measures and procedures.
- Provide verbal and written instructions about wound care, prevention of complications, pain management, and nutrition.
- Inform and review with patient specific exercises and use of elastic pressure garments and splints; provide written instructions.
- Teach patient and family to recognize abnormal signs and report them to the physician.
- Assist the patient and family in planning for the patient’s continued care by identifying and acquiring supplies and equipment that are needed at home.
- Encourage and support followup wound care.
- Refer patient with inadequate support system to home care resources for assistance with wound care and exercises.
- Evaluate patient status periodically for modification of home care instructions and/or planning for reconstructive surgery.
Expected Patient Outcomes
- Demonstrates activity tolerance required for desired daily activities
- Adapts to altered body image
- Demonstrates knowledge of required selfcare and followup care
- Exhibits no complications
[mtouchquiz 428 title=off]
Nursing Care Plan
Nursing diagnosis, impaired physical mobility.
May be related to
- Neuromuscular impairment, pain/discomfort, decreased strength and endurance
- Restrictive therapies, limb immobilization; contractures
Possibly evidenced by
- Reluctance to move/inability to purposefully move
- Limited ROM, decreased muscle strength control and/or mass
Desired Outcomes
- Maintain position of function as evidenced by absence of contractures.
- Maintain or increase strength and function of affected and/or compensatory body part.
- Verbalize and demonstrate willingness to participate in activities.
- Demonstrate techniques/behaviors that enable resumption of activities.
- Rationale: Promotes functional positioning of extremities and prevents contractures, which are more likely over joints.
- Rationale: Edema may compromise circulation to extremities, potentiating tissue necrosis and development of contractures.
- Rationale: It is easier to enlist participation when patient is aware of the possibilities that exist for recovery.
- Rationale: Prevents progressively tightening scar tissue and contractures; enhances maintenance of muscle and joint functioning and reduces loss of calcium from the bone.
- Rationale: Reduces muscle and tissue stiffness and tension, enabling patient to be more active and facilitating participation.
- Rationale: Increases patient’s strength and tolerance for activity.
- Rationale: Enables family/SO to be active in patient care and provides more consistent therapy.
- Rationale: Combining activities produces improved results by enhancing effects of each.
- Rationale: Promotes independence, enhances self-esteem, and facilitates recovery process.
- Rationale:Promotes independence, enhances self-esteem, and facilitates recovery process.
Knowledge Deficit
- Lack of exposure/recall
- Information misinterpretation; unfamiliarity with resources
- Questions/request for information, statement of misconception
- Inaccurate follow-through of instructions, development of preventable complications
- Verbalize understanding of condition, prognosis, and potential complications.
- Verbalize understanding of therapeutic needs.
- Correctly perform necessary procedures and explain reasons for actions.
- Initiate necessary lifestyle changes and participate in treatment regimen.
- Rationale: Provides knowledge base from which patient can make informed choices.
- Rationale: Patient frequently has a difficult and prolonged adjustment after discharge. Problems often occur (sleep disturbances, nightmares, reliving the accident, difficulty with resumption of social interactions, intimacy and sexual activity, emotional lability) that interfere with successful adjustment to resuming normal life.
- Rationale: Promotes competent self-care after discharge, enhancing independence.
- Rationale: Itching, blistering, and sensitivity of healing wounds or graft sites can be expected for an extended time, and injury can occur because of the fragility of the new tissue.
- Rationale: Promotes optimal regrowth of skin, minimizing development of hypertrophic scarring and contractures and facilitating healing process. Note: Consistent use of the pressure garment over a long period can reduce the need for reconstructive surgery to release contractures and remove scars.
- Rationale: Maintains mobility, reduces complications, and prevents fatigue, facilitating recovery process.
- Rationale: Imposed restrictions depend on severity and location of injury and stage of healing.
- Rationale: Optimal nutrition enhances tissue regeneration and general feeling of well-being. Note: Patient often needs to increase caloric intake to meet calorie and protein needs for healing.
- Rationale: Reiteration allows opportunity for patient to ask questions and be sure understanding is accurate.
- Rationale: Provides perspective to some of the problems patient and/or SO may encounter, and aids awareness that assistance is available when necessary.
- Rationale: Early detection of developing complications (infection, delayed healing) may prevent progression to more serious or life-threatening situations.
- Rationale: Long-term support with continual reevaluation and changes in therapy is required to achieve optimal recovery.
- Rationale: Provides easy access to treatment team to reinforce teaching, clarify misconceptions, and reduce potential for complications.
- Rationale: To prevent further injury.
- Rationale: Facilitates transition to home, provides assistance with meeting individual needs, and supports independence.
Disturbed Body Image
- Situational crisis: traumatic event, dependent patient role; disfigurement, pain
- Negative feelings about body/self, fear of rejection/reaction by others
- Focus on past appearance, abilities; preoccupation with change/loss
- Change in physical capacity to resume role; change in social involvement
- Incorporate changes into self-concept without negating self-esteem.
- Verbalize acceptance of self in situation.
- Talk with family/SO about situation, changes that have occurred.
- Develop realistic goals/plans for the future.
- Rationale: Traumatic episode results in sudden, unanticipated changes, creating feelings of grief over actual or perceived losses. This necessitates support to work through to optimal resolution.
- Rationale: Acceptance of these feelings as a normal response to what has occurred facilitates resolution. It is not helpful or possible to push patient before ready to deal with situation. Denial may be prolonged and be an adaptive mechanism because patient is not ready to cope with personal problems.
- Rationale: Patient and SO tend to deal with this crisis in the same way in which they have dealt with problems in the past. Staff may find it difficult and frustrating to handle behavior that is disrupting and not helpful to recuperation but should realize that the behavior is usually directed toward the situation and not the caregiver.
- Rationale: Enhances trust and rapport between patient and nurse.
- Rationale: Promotes acceptance of reality of injury and of change in body and image of self as different.
- Rationale:Promotes positive attitude and provides opportunity to set goals and plan for future based on reality.
- Rationale: Helps begin process of looking to the future and how life will be different.
- Rationale: Words of encouragement can support development of positive coping behaviors.
- Rationale: Allows patient and SO to be realistic in expectations. Also assists in demonstration of importance of and/or necessity for certain devices and procedures.
- Rationale: To opens lines of communication and provides ongoing support for patient and family
- Rationale: Promotes ventilation of feelings and allows for more helpful responses to patient.
- Rationale: Prepares patient and SO for reactions of others and anticipates ways to deal with them.
- Rationale: Helpful in identifying ways/devices to regain and maintain independence. Patient may need further assistance to resolve persistent emotional problems.
- Rationale: Reconstructive surgery can help patient gain self-esteem and confidence.
- Rationale: Reinforcing teaching can help patient achieve self-care.
Fear/Anxiety
- Situational crises: hospitalization/isolation procedures, interpersonal transmission and contagion, memory of the trauma experience, threat of death and/or disfigurement
- Expressed concern regarding changes in life, fear of unspecific consequences
- Apprehension; increased tension
- Feelings of helplessness, uncertainty, decreased self-assurance
- Sympathetic stimulation, extraneous movements, restlessness, insomnia
- Verbalize awareness of feelings and healthy ways to deal with them.
- Report anxiety/fear reduced to manageable level.
- Demonstrate problem-solving skills, effective use of resources.
- Rationale: Knowing what to expect usually reduces fear and anxiety, clarifies misconceptions, and promotes cooperation. Because of the shock of the initial trauma, many people do not recall information provided during that time.
- Rationale: Helps patient and SO know that support is available and that healthcare provider is interested in the person, not just care of the burn.
- Rationale: Promotes sense of control and cooperation, decreasing feelings of helplessness or hopelessness.
- Rationale: Initially, patient may use denial and repression to reduce and filter information that might be overwhelming. Some patients display calm manner and alert mental status, representing a dissociation from reality, which is also a protective mechanism.
- Rationale: Indicators of extreme anxiety and delirium state in which patient is literally fighting for life. Although cause can be psychologically based, pathological life-threatening causes must be ruled out.
- Rationale: Helps patient stay in touch with surroundings and reality.
- Rationale: Patient may need to tell the story of what happened over and over to make some sense out of a terrifying situation. Adjustment to the impact of the trauma, grief over losses and disfigurement can easily lead to clinical depression, psychosis, and posttraumatic stress disorder (PTSD).
- Rationale: Compassionate statements reflecting the reality of the situation can help patient and SO acknowledge that reality and begin to deal with what has happened.
- Rationale: Past successful behavior can be used to assist in dealing with the present situation.
- Rationale: Patients experience severe anxiety associated with burn trauma and treatment. These interventions are soothing and helpful for positive outcomes.
- Rationale: The family may initially be most concerned about patient’s dying and/or feel guilty, believing that in some way they could have prevented the incident.
- Rationale: Family relationships are disrupted; financial, lifestyle or role changes make this a difficult time for those involved with patient, and they may react in many different ways.
- Rationale: Maintains contact with a familiar reality, creating a sense of attachment and continuity of life.
- Rationale: Provides a wider support system and promotes continuity of care and coordination of activities.
Impaired Skin Integrity
- Disruption of skin surface with destruction of skin layers (partial-/full-thickness burn) requiring grafting
- Absence of viable tissue
- Wound Healing: Secondary Intention (NOC)
- Demonstrate tissue regeneration.
- Achieve timely healing of burned areas.
- Rationale: Provides baseline information about need for skin grafting and possible clues about circulation in area to support graft.
- Rationale: Prepares tissues for grafting and reduces risk of infection/graft failure.
Maintain wound covering as indicated
- Rationale: Nylon fabric and/or silicon membrane containing collagenous porcine peptides that adheres to wound surface until removed or sloughed off by spontaneous skin reepithelialization. Useful for eschar-free partial-thickness burns awaiting autografts because it can remain in place 2–3 wk or longer and is permeable to topical antimicrobial agents.
- Rationale: Hydroactive dressing that adheres to the skin to cover small partial-thickness burns and that interacts with wound exudate to form a soft gel that facilitates debridement.
- Rationale: Thin, transparent, elastic, waterproof, occlusive dressing (permeable to moisture and air) that is used to cover clean partial-thickness wounds and clean donor sites. Reduces swelling/limits risk of graft separation.
- Rationale: Movement of tissue under graft can dislodge it, interfering with optimal healing.
- Rationale: Areas may be covered by translucent, nonreactive surface material (between graft and outer dressing) to eliminate shearing of new epithelium and protect healing tissue. The donor site is usually covered for 4–24 hr, then bulky dressings are removed and fine mesh gauze is left in place.
- Rationale: Promotes circulation and prevents ischemia or necrosis and graft failure.
- Rationale: Evaluates effectiveness of circulation and identifies developing complications.
- Rationale: Newly grafted skin and healed donor sites require special care to maintain flexibility.
- Rationale:Fluid-filled blebs prevent graft adherence to underlying tissue, increasing risk of graft failure.
Prepare for/assist with surgical grafting or biological dressings:
- Rationale: Skin grafts obtained from living persons or cadavers are used as a temporary covering for extensive burns until person’s own skin is ready for grafting (test graft), to cover excised wounds immediately after escharotomy, or to protect granulation tissue.
- Rationale: Skin grafts may be carried out with animal skin for the same purposes as homografts or to cover meshed autografts.
- Rationale: Skin graft obtained from uninjured part of patient’s own skin and prepared in a laboratory; may be full-thickness or partial-thickness. Note: This process takes 20–30 days from harvest to application. The new CEA sheets are 1–6 cell layers thick and thus are very fragile.
- Rationale: Wound covering approved by the Food and Drug Administration (FDA) for full-thickness and deep partial-thickness burns. It provides a permanent, immediate covering that reproduces the skin’s normal functions and stimulates the regeneration of dermal tissue.
Imbalanced Nutrition
- Hypermetabolic state (can be as much as 50%–60% higher than normal proportional to the severity of injury)
- Protein catabolism
- Anorexia, restricted oral intake
- Decrease in total body weight, loss of muscle mass/subcutaneous fat, and development of negative nitrogen balance
- Demonstrate nutritional intake adequate to meet metabolic needs as evidenced by stable weight/muscle-mass measurements, positive nitrogen balance, and tissue regeneration.
- Rationale: Ileus is often associated with postburn period but usually subsides within 36–48 hr, at which time oral feedings can be initiated.
- Rationale: Appropriate guides to proper caloric intake include 25 kcal/kg body weight, plus 40 kcal per percentage of TBSA burn in the adult. As burn wound heals, percentage of burned areas is reevaluated to calculate prescribed dietary formulas, and appropriate adjustments are made.
- Rationale: Indirect calorimetry, if available, may be useful in more accurately estimating body reserves or losses and effectiveness of therapy.
- Rationale: Helps prevent gastric distension or discomfort and may enhance intake.
- Rationale: Calories and proteins are needed to maintain weight, meet metabolic needs, and promote wound healing.
- Rationale: Provides patient or SO sense of control; enhances participation in care and may improve intake.
- Rationale: Sitting helps prevent aspiration and aids in proper digestion of food. Socialization promotes relaxation and may enhance intake.
- Rationale: Clean mouth and clean palate enhances taste and helps promote a good appetite.
- Rationale: To decompress the stomach and avoid aspiration of stomach contents.
- Rationale:Monitors for development of hyperglycemia related to hormonal changes or demands or use of hyperalimentation to meet caloric needs.
- Rationale: Useful in establishing individual nutritional needs (based on weight and body surface area of injury) and identifying appropriate routes.
- Rationale: Calories (3000–5000 per day), proteins, and vitamins are needed to meet increased metabolic needs, maintain weight, and encourage tissue regeneration. Note: Oral route is preferable once GI function returns.
- Rationale: Provides continuous supplemental feedings when patient is unable to consume total daily calorie requirements orally. Note: Continuous tube feeding during the night increases calorie intake without decreasing appetite and oral intake during the day.
- Rationale: Total parenteral nutrition (TPN) maintains nutritional intake and meets metabolic needs in presence of severe complications or sustained esophageal or gastric injuries that do not permit enteral feedings.
- Rationale: Indicators of nutritional needs and adequacy of diet/therapy.
- Rationale: Elevated serum glucose levels may develop because of stress response to injury, high caloric intake, pancreatic fatigue.
Ineffective Tissue Perfusion
Risk factors may include
- Reduction/interruption of arterial/venous blood flow, e.g., circumferential burns of extremities with resultant edema
- Hypovolemia
- Maintain palpable peripheral pulses
- Rationale: Edema formation can readily compress blood vessels, thereby impeding circulation and increasing venous stasis or edema. Comparisons with unaffected limbs aid in differentiating localized versus systemic problems (hypovolemia or decreased cardiac output).
- Rationale: Promotes systemic circulation and venous return that may reduce edema or other deleterious effects of constriction of edematous tissues. Prolonged elevation can impair arterial perfusion if blood pressure (BP) falls or tissue pressures rise excessively.
- Rationale: If BP readings must be obtained on an injured extremity, leaving the cuff in place may increase edema formation and reduce perfusion, and convert partial thickness burn to a more serious injury.
- Rationale: Indicators of decreased perfusion and/or increased pressure within enclosed space, such as may occur with a circumferential burn of an extremity (compartment syndrome).
- Rationale: Promotes local and systemic circulation.
- Rationale: Cardiac dysrhythmias can occur as a result of electrolyte shifts, electrical injury, or release of myocardial depressant factor, compromising cardiac output.
- Rationale: Maximizes circulating volume and tissue perfusion.
- Rationale: Losses or shifts of these electrolytes affect cellular membrane potential and excitability, thereby altering myocardial conductivity, potentiating risk of dysrhythmias, and reducing cardiac output and tissue perfusion.
- Rationale: Altered tissue perfusion and edema formation impair drug absorption. Injections into potential donor sites may render them unusable because of hematoma formation.
- Rationale: Ischemic myositis may develop because of decreased perfusion.
- Rationale: Enhances circulation by relieving constriction caused by rigid, nonviable tissue (eschar) or edema formation.
- Destruction of skin/tissues; edema formation
- Manipulation of injured tissues, e.g., wound debridement
- Reports of pain
- Narrowed focus, facial mask of pain
- Alteration in muscle tone; autonomic responses
- Distraction/guarding behaviors; anxiety/fear, restlessness
- Report pain reduced/controlled.
- Display relaxed facial expressions/body posture.
- Participate in activities and sleep/rest appropriately.
- Rationale: Temperature changes and air movement can cause great pain to exposed nerve endings.
- Rationale: Elevation may be required initially to reduce edema formation; thereafter, changes in position and elevation reduce discomfort and risk of joint contractures.
- Rationale: Elevation of linens off wounds may help reduce pain.
- Rationale: Position of function reduces deformities or contractures and promotes comfort. Although flexed position of injured joints may feel more comfortable, it can lead to flexion contractures.
- Rationale: Movement and exercise reduce joint stiffness and muscle fatigue, but type of exercise depends on location and extent of injury.
- Rationale: Temperature regulation may be lost with major burns. External heat sources may be necessary to prevent chilling.
- Rationale: Pain is nearly always present to some degree because of varying severity of tissue involvement and destruction but is usually most severe during dressing changes and debridement. Changes in location, character, intensity of pain may indicate developing complications (limb ischemia) or herald improvement and/or return of nerve function and sensation.
- Rationale: Reduces severe physical and emotional distress associated with dressing changes and debridement.
- Rationale: Verbalization allows outlet for emotions and may enhance coping mechanisms.
- Rationale: Enhances patient’s sense of control and strengthens coping mechanisms.
- Rationale: Empathic support can help alleviate pain and/or promote relaxation. Knowing what to expect provides opportunity for patient to prepare self and enhances sense of control.
- Rationale: Promotes relaxation; reduces muscle tension and general fatigue.
- Rationale: Refocuses attention, promotes relaxation, and enhances sense of control, which may reduce pharmacological dependency.
- Rationale: Helps lessen concentration on pain experience and refocus attention.
- Rationale: Sleep deprivation can increase perception of pain/reduce coping abilities.
- Rationale: The burned patient may require around-the-clock medication and dose titration. IV method is often used initially to maximize drug effect. Concerns of patient addiction or doubts regarding degree of pain experienced are not valid during emergent/acute phase of care, but narcotics should be decreased as soon as feasible and alternative methods for pain relief initiated.
Risk for Infection
- Inadequate primary defenses: destruction of skin barrier, traumatized tissues
- Inadequate secondary defenses: decreased Hb, suppressed inflammatory response
- Environmental exposure, invasive procedures
- Achieve timely wound healing free of purulent exudate and be afebrile.
- Rationale: Dependent on type or extent of wounds and the choice of wound treatment (open versus closed), isolation may range from simple wound and/or skin to complete or reverse to reduce risk of cross contamination and exposure to multiple bacterial flora.
- Rationale: Prevents cross contamination; reduces risk of acquired infection.
- Rationale: Prevents exposure to infectious organisms.
- Rationale: Prevents cross-contamination from visitors. Concern for risk of infection should be balanced against patient’s need for family support and socialization.
- Rationale: Opportunistic infections (yeast) frequently occur because of depression of the immune system and/or proliferation of normal body flora during systemic antibiotic therapy.
- Rationale: Eyes may be swollen shut and/or become infected by drainage from surrounding burns. If lids are burned, eye covers may be needed to prevent corneal damage.
- Rationale: Prevents adherence to surface it may be touching and encourages proper healing. Note: Ear cartilage has limited circulation and is prone to pressure necrosis.
- Rationale: Identifies presence of healing (granulation tissue) and provides for early detection of burn-wound infection. Infection in a partial-thickness burn may cause conversion of burn to full-thickness injury. Note: A strong sweet, musty smell at a graft site is indicative of Pseudomonas.
- Rationale: Indicators of sepsis (often occurs with full-thickness burn) requiring prompt evaluation and intervention. Note: Changes in sensorium, bowel habits, and respiratory rate usually precede fever and alteration of laboratory studies.
- Rationale: Water softens and aids in removal of dressings and eschar (slough layer of dead skin or tissue). Sources vary as to whether bath or shower is best. Bath has advantage of water providing support for exercising extremities but may promote cross-contamination of wounds. Showering enhances wound inspection and prevents contamination from floating debris.
- Rationale: Early excision is known to reduce scarring and risk of infection, thereby facilitating healing.
- Rationale: Promotes healing. Prevents autocontamination. Small, intact blisters help protect skin and increase rate of re-epithelialization unless the burn injury is the result of chemicals (in which case fluid contained in blisters may continue to cause tissue destruction).
- Rationale: Provides baseline and documentation of healing process.
- Rationale: The following agents help control bacterial growth and prevent drying of wound, which can cause further tissue destruction.
- Rationale: Broad-spectrum antimicrobial that is relatively painless but has intermediate, somewhat delayed eschar penetration. May cause rash or depression of WBCs.
- Rationale:Antibiotic of choice with confirmed invasive burn-wound infection. Useful against Gram-negative or Gram-positive organisms. Causes burning or pain on application and for 30 min thereafter. Can cause rash, metabolic acidosis, and decreased Paco2.
- Rationale: Effective against Staphylococcus aureus, Escherichia coli, and Pseudomonas aeruginosa, but has poor eschar penetration, is painful, and may cause electrolyte imbalance. Dressings must be constantly saturated. Product stains skin/surfaces black.
- Rationale: Effective against Gram-positive organisms and is generally used for superficial and facial burns.
- Rationale: Broad-spectrum antimicrobial, but is painful on application, may cause metabolic acidosis or increased iodine absorption, and damage fragile tissues.
- Rationale: Useful for partial- and full-thickness burns; filling dead spaces, rehydrating dry wound beds, and promoting autolytic debridement. May be used when infection is present.Systemic antibiotics are given to control general infections identified by culture and sensitivity. Subeschar clysis has been found effective against pathogens in granulated tissues at the line of demarcation between viable or nonviable tissue, reducing risk of sepsis.
- Rationale: Tissue destruction and altered defense mechanisms increase risk of developing tetanus or gas gangrene, especially in deep burns such as those caused by electricity.
- Rationale: Decreased risk of infection at insertion site with possibility of progression to septicemia.
- Rationale: Allows early recognition and specific treatment of wound infection.
Related Posts
Thyrotoxicosis (thyroid storm) nursing care plan & management, colonoscopy, pulmonary embolus nursing management.

The Royal Children's Hospital Melbourne
- My RCH Portal
- Health Professionals
- Patients and Families
- Departments and Services
- Health Professionals
- Departments and Services
- Patients and Families
- Research
Nursing guidelines
- About nursing guidelines
- Nursing guidelines index
- Developing and revising nursing guidelines
- Other useful clinical resources
- Nursing guideline disclaimer
- Contact nursing guidelines
In this section
Nursing management of burn injuries

Introduction
Definition of Terms
Assessment - ABCD
Management - Fluids and Burn Dressings
Companion Documents
Evidence Table
Children are vulnerable to sustaining a burn injury due to their physiological, psychological, and developmental differences. Burn injuries have a significant impact on paediatric patients and may affect a range of body systems. The impact of these injuries on children and families is often long lasting. As the injury itself and required treatment often causes distress, pain and anxiety, appropriate management by nurses is essential in providing family centered care. Ongoing care requirements are based on the size, depth, anatomical site and mechanism of injury.
The aim of this clinical guideline is to assist and support nursing staff at The Royal Children’s Hospital to plan and deliver care to children with burn injuries, across all departments including: Emergency, Paediatric Intensive Care Unit, Inpatient Units, Theatres and Outpatients.
Definition of terms
- Burns Multidisciplinary Team – consists of Burns Consultant/Fellow, Burns Clinical Nurse Consultant, Burns registrar/resident, Nurse Coordinator, Occupational Therapist, Physiotherapist, Dietitian, Social Work, Mental Health, Child Life Therapy (CLT), Specialist Clinics Team.
- % TBSA – percentage of total body surface area burnt (not including erythema or superficial burns) calculated using the Lund Browder chart .
- Minor Burn – In paediatric burns a minor burn is considered to be less than 10% TBSA.
- Major Burn – In paediatric burns a major burn is considered to be more than 10% TBSA.
Burn injuries cause a significant insult on the body and a thorough ABCD assessment, followed by a full head to toe and focused assessment are vital to ensure clinical issues/deterioration are identified early and appropriate management initiated. See Burns- Acute management CPG for further details of burn injury assessment. Assessment of the pediatric patient with a burn injury should occur on admission and regularly throughout care. Detailed information regarding completion and documentation of ABCD, head to toe and focused assessments can be located on the Nursing Assessment Clinical Guideline . Burns specific information is outlined below.
Airway and Breathing
Assessment and monitoring of airway patency and breathing should be carefully observed as patients at risk of inhalation burns can deteriorate up to 72 hours post burn injury, particularly if they have:
- Sustained burns in an enclosed space (at risk due to smoke inhalation)
- Have facial burns
- Singed nasal hairs
- Facial swelling
- Blackened sputum
- Stridor or hoarseness of voice
- Respiratory distress/increased work of breathing
If inhalation burns are suspected high flow oxygen therapy via a Hudson mask should be administered to the patient and changes/abnormal findings reported to the treating team immediately for further assessment and management.
Circulation
Children who sustain burns injuries are at increased risk of circulatory compromise due to significant fluid loss and fluid shifts, these patients must be closely monitored for:
- Signs and symptoms of hypovolemia.
- Signs and symptoms of hypothermia.
Other circulatory concerns include:
- Circumferential burns should be identified, monitored for circulatory compromise ( neurovascular observations nursing guideline ) and the affected area elevated where ever possible.
- Consider the need for an ECG and continuous cardiac monitoring if the burn is of electrical origin.
Pain assessment
Detailed information regarding paediatric pain assessment can be located on the Pain Assessment Nursing Clinical Guideline . Information regarding procedural pain management can be located on the Procedural Pain Management Clinical Guideline .
Wound assessment
Assessment of the burn injury should occur on the initial presentation to the Royal Children’s Hospital as well as prior to completing wound care throughout the inpatient stay and outpatient visits. Burn injuries can take up to 10 days to truly present the depth and extent of injury so reassessment is vital. As burn injuries heal accurate wound assessment will ensure wound management is altered as needed to ensure appropriate wound care continues to be delivered to the patient. Wound assessment of a burn injury includes (available on Electronic medical Records):
- Assessment of Total Body Surface Area (TBSA) burnt, utilising the Lund Browder chart. Areas of erythema and superficial burns are not included in calculations of TBSA.
- Assessment of depth of burn injury.
- Assessment of wound healing.
Accurate documentation of wound assessment should be recorded. Further information regarding wound assessment in a burn injury can be located on the Burns Clinical Practice Guideline as well as the Burns Unit: Clinical Information . Further information regarding wound assessment and healing can be located on the Wound Care Clinical nursing guideline .
A thorough patient history should be collected on admission to hospital. Specific information regarding the burn injury must be obtained from the patient, family and first responders as this will inform ongoing treatment. History taking should include:
- Time of injury
- Mechanism of injury: How the burn occurred/type of burn, including length of exposure and estimated temperatures of heat source.
- Was first aid completed? If so, what type and for how long?
- Tetanus status of the patient (if not up to date consider immunisation, see Immunisation of inpatients Clinical Guideline .)
In addition to this information a detailed patient and family history should also be obtained. Further information regarding this can be located on the Nursing Assessment Nursing Clinical Guideline . Non accidental injuries must be considered when the history does not match with the injury or inconsistencies with the history/story occur. Refer to medical staff & social work. Victorian Forensic Paediatric Medical Service (VPFMS) can also be notified. For further information regarding non accidental injuries refer to the Child Abuse Clinical Guideline .
Social history
Burn injuries are traumatic and life altering events which can significantly impact the patient and their family. Early support from social work, contact with CLT and chaplains should be offered to the child, siblings and family. It may also be appropriate to consider referrals to mental health/psychology.
Management
Completion of first aid for a child who has sustained a burn injury is an important initial aspect of care as it assists with pain relief as well as minimising the progression of tissue damage. First aid is effective for up to three hours post time of injury. If appropriate first aid was not initiated and it is still within the 3 hour time frame post burn injury, first aid should be completed as outlined below, prior to any wound care:
- The area of tissue damage should be cooled with cool running water for 20 minutes.
- Ensure the unburnt areas of the patient are covered and warm to prevent hypothermia.
Further information regarding burn injury first aid including burns to the eye area and chemical burns can be found on the Burns Clinical Practice Guideline .
For initial fluid management see Burns Acute Management CPG
Burn injuries greater than 10% TBSA and including the dermis result in circulatory compromise secondary to fluid loss via damaged tissue, widespread vasodilation as well as increase capillary permeability and fluid shifts (third spacing). This can result in hypovolemia leading to burns shock. Therefore it is vital that adequate fluid is administered to the patient in combination with ongoing circulatory and fluid balance assessment.
- A Strict Fluid Balance must be maintained at all times, including all intake (both intravenous and oral) and strict measurement of all output (weigh nappies, weigh pans/bottle, measure IDC)
- Fluid resuscitation is required in patients who have >10-15% TBSA.
- Patients receiving fluid resuscitation may need two large bore Intravenous cannulas inserted
- Fluid resuscitation is calculated utilising the modified parkland formula. For further information regarding this please see the Burns Acute management CPG .
- An IDC is essential for patients receiving fluid resuscitation to allow close monitoring of fluid status and adjustment of IVT as necessary.
- Expected urine output is 1ml/kg/hr unless otherwise stated by the medical team.
- U&E’s should be monitored 8 hourly while patient is receiving fluid resuscitation.
- Fluid resuscitation rates will need to be adjusted to accommodate the patients urine output.
Burn pain can be extremely intense and distressing for paediatric patients and can also be challenging to manage due to the individual experience and its unique characteristics. Initial and ongoing pain management is vital to ensure patient comfort, maximise healing and minimise risk of mental trauma/post-traumatic stress.
- Initial pain relief should be administered immediately following an accurate pain assessment, further information regarding initial pain management can be located on the Burns Clinical Practice Guideline .
- Pre-emptive analgesia may be necessary prior to re-positioning, physiotherapy and follow up outpatient appointments.
- Reassessment and evaluation of pain management is vital, referral to Children’s Pain Management Service may be necessary.
Burn pain experienced by patients is likely to increase during procedures such as dressing changes. Management of pain during burn dressing changes is discussed in detail below ( preparing for a dressing change ).
Preparation for Burns Dressing
Preparation of patient and family.
Burn dressing changes can produce feelings of anxiety and distress in both patients and their families. It is very important that both patients and families are physically and emotionally prepared and well informed regarding the procedure and the pain management options.
- Families/primary care givers should be given a thorough explanation of the procedure, where appropriate pictures could be used to visualise the procedure along with orientation to the treatment room/bathroom to be used.
- Referral to CLT prior to the procedure may assist in explaining and preparing the patient for the dressing change. CLT are also able to empower the child to identify distraction techniques, as well as provide support and distraction throughout the procedure.
- Where possible and appropriate children should be given the opportunity to choose whether they want to participate in wound care for example assisting to remove dressings.
For further information, staff and families can access reducing children’s discomfort during tests and procedures kids health info factsheet . Assessment
Assessment
Children who are planned to undergo a burns dressing change should have an ABCD assessment completed along with pain assessment prior to the dressing change commencing. The child will require continuous ABCD monitoring and pain assessment throughout the procedure to ensure that analgesics provide are adequate and effective.
Pre Medication/ Pain Relief
Burns dressing changes can be painful and distressing for children. Nursing staff should assess the child’s pain prior to the procedure commencing and pre-emptive analgesia should be administered. Staff should re-evaluate the effectiveness prior to the procedure commencing and throughout the procedure. Choice of analgesia is an individual process and staff should take into account the % TBSA, depth, amount of debridement required as well as the pain tolerance, distress and past experience of the child. Review of analgesia/sedation requirements for previous dressing changes is essential. The Children’s Pain Management Service (CPMS) may also be utilised to assist in planning procedural pain relief for burns dressing changes . Options may include:
- Simple analgesia such as Paracetamol and NSAIDs
- Oral Analgesia such as Opioids (Oxycodone), Tramadol, Ketamine and Oral Sedatives such as Benzodiazepines e.g. Diazepam, Midazolam
- Intravenous Sedation/Analgesics including infusions, PCA or intermittent bolus (Morphine/Fentanyl/Ketamine)
- Nitrous Oxide (refer to the procedural sedation ward and ambulatory care p rocedure)
- Intranasal medications such as Intranasal Fentanyl
- Anaesthetics may be involved to provide sedation (Ketamine/Propofol) and continuous monitoring of the patient.
A combination of the above options may be ordered and utilised to provide pain relief. Further information regarding this can be located on the Procedural Sedation – ward and ambulatory care procedure or through consultation with CPMS or comfort kids.
Pain Assessment should occur continuously throughout the procedure by observing the behaviour and comfort level of the child as well as using an appropriate pain assessment scale. If analgesia and sedative agents prescribed are not providing effective pain management/sedation then the procedure should be paused until appropriate analgesia/sedation is available and pain is manageable. Escalation to the children’s pain management service or Burns resident can occur at any stage throughout the procedure. As the patient’s burn injury heals, analgesia and sedative agents utilised throughout the procedure should start to be slowly weaned with the support of CPMS, medical teams and senior nursing staff. All sedative agents should be administered in line with the Sedation and Procedural Sedation Ward and Ambulatory Areas procedure .
Staffing Requirements
To complete a burns dressing change in a safe and time efficient manner which minimises patient and family distress, staffing requirements must be considered.
- Simple analgesia: 1-2 nursing staff of which 1 is experienced in burns dressing changes.
- Oral sedation agents: 2-3 nursing staff of which 1 monitors the patient, 1 is experienced in burns dressing and 1 staff member assists.
- Nitrous Oxide: 2-4 nursing staff of which 1 is accredited in nitrous oxide administration, 1 is experienced in burns dressing and 1-2 staff members assists
- IV agents: An Anaesthetist and Anaesthetic technician are required; 2-3 nursing staff of which 1 is experienced in burns dressing and 1-2 nursing staff members to assist
All roles must be designated prior to commencement of dressing change and the patient should remain in line of sight to staff at all times. For further information refer to the Sedation and Procedural Sedation Guideline Ward and Ambulatory Care Areas procedure . Burn injuries which have a large TBSA percentage and patients with reduced mobility may require increased staff numbers to assist in dressing changes. For further information refer to the High Dependency and Special Nursing Care nursing guideline .
Preparation of environment and equipment
- For children who have larger %TBSA burn injuries (>10%) consider using a treatment area where heaters can be utilised to minimise the risk of hypothermia. These heaters should be turned on prior to the dressing change commencing. (i.e. Platypus Burns Bathroom, Theatre)
- Adequate preparation of the environment should be completed prior to the child being taken into the treatment room/bathroom.
- Physiotherapy/Occupational therapy – to review patient mobility and splinting requirements.
- Medical team – to review burn injury and wound healing.
- Clinical photography
Staff Roles
Prior to the procedure a team leader should be allocated. Other team member’s roles/responsibilities ie. Dressings nurse, sedationist, observations nurse, hygiene nurses should also be communicated. An ISBAR handover should also occur; identifying patient name, age, weight, allergies, procedure, any pre procedure medication and staff roles.
Burns dressing
Staff should adhere to the aseptic technique procedure for all aspects of wound care outlined below.
Removal of previous dressing
Removal of the previous dressing should not damage the healing burn wound and should be as atraumatic as possible. The use of an adhesive remover, normal saline or water will assist with gentle removal of previous dressings.
Wound Management
Clean the wound using a soft wipe with water, normal saline, pH neutral soap or cetrimide (please note cetrimide is not to be used on face or scalp). Enough pressure should be applied to debride the damaged skin and remove exudate, loose skin and slough. Consider the need for a wound swab and complete if necessary. Debridement of any blisters present allows for wound bed assessment and appropriate dressing application. The wound and surrounding skin should be dry before application of the dressing.
Personal Hygiene
Ensure the patient’s personal hygiene is thoroughly attended to if the burns dressing change is occurring in the bath or shower. If the patient is not having a bath use a sponge to clean non dressed areas.
Application of Burns Dressing
- A thorough wound assessment should occur with every dressing change and will determine the appropriate dressing required (see wound assessment above).
- Dressings should cover all area where tissue damage has occurred but avoid unburnt skin as maceration may occur.
- A crepe bandage/tubifast/tubigrip assists with securing dressings as well as absorbing some excess fluid. They also add pressure to support with scar management.
- Oedema is common in the initial days post burn, therefore tight circumferential bandages should not be applied. Elevation of the limb in the immediate days post injury will limit swelling.
- Dermal burns produce a large amount of exudate in the initial few days and changing of the outer bandage or tubifast may need to occur. Where possible retaping/securement of the dressing should occur unless a dressing change is scheduled.
| Common burn dressing product | |
| Acticoat™ – Note – Acticoat™ is a 3 day application Acticoat 7™ is a 7 day application Acticoat Flex is a 3 or 7 day application Commonly used on partial to full thickness burns as well as burns of indeterminable depth in initial stages of injury. | - Moisten Acticoat ™ with sterile water, not saline, to activate - Wring out excess water from Acticoat ™ using forceps. Silver or blue side to wound. - Cover Acticoat ™ with Intrasite Conformable ™ - Cover the 2 layers with cling wrap and cut to appropriate size, ensuring no overlap of cling wrap on healthy skin. - Apply dressing to wound - Secure with tape e.g. Hypafix ™ or Mefix ™ - Reinforce dressing with crepe and tubifast/tubigrip - Please review the Burns Unit: Clinical Information for pictures of an Acticoat™ dressing ( ). |
| Mepilex Ag™ Commonly used on superficial, mid dermal or deep dermal to full thickness facial burns or on areas where it is difficult to secure | - Self-adhesive Secure with tape e.g. Hypafix ™ or Mefix ™ or tubifast. |
| Bactigras™ Commonly used on superficial dermal wounds and doner site. | - Use in conjunction with gauze. - Secure with tape e.g. Hypafix ™ or Mefix ™ or tubifast. |
| Xeroform™ Commonly used on small areas of unhealed burn when Silver products are no longer required. Also used on areas of hypergranulation. | - Kenacomb™ ointment may be applied prior to xeroform™ to areas of hyper granulation. - Use in conjunction with Melolin™ - Secure with tape e.g. Hypafix ™ or Mefix ™ or tubifast. |
Additional products may be utilised on burns wounds at the discretion of medical and nursing staff.
For further information regarding the above and additional products please refer to the wound care guideline .
Specific body areas
Facial burn’s care.
Facial burns may require regular wound care including cleansing followed by application of paraffin cream. Parents should be encouraged to be involved in providing this care.
If dressings are utilised on the face balaclavas can be made from large tubifast and used to secure dressing products.
Additional information can be located on the Burns Medical Treatment .
Hand Burn’s Care
Any dressing applied to fingers, should ensure fingers are taped individually. Padding must be applied to web spaces to prevent further friction/pressure area injury. Initially fingers which have circumferential burns should be dressed with the finger tips exposed to monitor neurovascular status. Once oedema has decreased the finger tips can be enclosed in the dressing.
Referral to hand therapy is vital.
Documentation
A summary post dressing change should be documented including: pain relief/ sedation and effect, non-pharmacological techniques and effect, parental involvement, wound assessment, dressing product utilised, staff present (including allied health, interpreter etc.) and plan of ongoing care. See Nursing Documentation Clinical Guideline for further information.
Nutrition
Nutrition plays a vital role in burn healing, minimising complications of care and meeting the increased metabolic demands associated with paediatric patients with burns. A diet high in protein, calcium, energy and micronutrients (in particular Zinc and Vitamin C) has been shown to be most beneficial for wound healing. Children should be encouraged to eat and drink foods high in these nutrients and nutritional supplements such as Sustagen™ may also be required.
Insertion of a nasogastric tube and commencement of enteral feeds should be considered for children who sustain significant burn injuries and/or facial burns and are unable to tolerate adequate oral intake. Where possible feeds should commence within 6 - 8 hours of the burn injury.
Referral to the Burns Team Dietician is recommended for all patients with significant burn injuries, facial burns, infants as well as patients who are not tolerating adequate oral intake.
Management of Itch
Itching is a common and debilitating issue in the healing phase of a burn injury.
The following may assist in reducing itch:
- Advise child and parent to avoid scratching - short finger nails will assist in this.
- Consider use of antihistamines i.e. Periactin or Certizdine
- Avoid overheating the child
- Fragrance free moisturiser (Sorbolene™) may assist.
- Distraction will play a big role in patient comfort
Scar management:
Strategies to reduce scar development post burn injury include:
- Regular bathing and showering
- Massage with fragrance free moisturiser (Sorbolene™) should be massaged into the healed skin at least twice daily to daily.
- Pressure therapy in the form of tubifast/tubigrip, tapes, pressure garments and silicone may be prescribed by Physiotherapy (PT) or Occupational therapy (OT). It is often recommended that garments are worn continuously except during personal hygiene.
Physiotherapy / occupational therapy – splinting & positioning:
Physiotherapy (PT) and Occupational therapy (OT) may be necessary throughout both inpatient stay and outpatient management for patients who have sustained a burn injury. Significant burn wounds and those over joints are at high risk of contracture development. This can have an impact on both growth and mobility. Prevention of contractures needs to occur early and to assist in this PT and OT will prescribe patients with a splinting and positioning regime. To aid PT/OT in assessing the patient’s burn injury and range of movement it is often beneficial for them to attend changes of dressings. It is vital that these regimes are adhered to by nursing staff. Paediatric patients may find the splints and positioning regimes uncomfortable and distressing. It is important to educate both patient and family on the importance of splints and the positioning regimes. Strategies to support splinting and positioning regimes include:
- Regular and pre-emptive analgesia
- CLT, distraction and rewards (i.e. sticker charts)
Concerns regarding splinting and positioning regimes should be documented and reported back to PT/OT so as appropriate alterations to regimes can be initiated.
Discharge planning
The decision for a patient to be discharged should have involvement from the burns multidisciplinary team and family meetings may be beneficial for planning purposes. Early discussion regarding discharge may facilitate a smoother transition home for the family.
Children may be ready for discharge when:
- Pain is able to be appropriately managed at home
- An appropriate plan for wound care and follow up has been made
- Nutritional requirements are being met
- Mobility, positioning and splinting are able to be managed at home
The following should be discussed with the family and child prior to discharge
- Pain management and itch plan, including plan for procedures (outpatients dressing changes)
- Home care of burn wound
- Nutritional requirements
- PT/OT recommendations
- Medical review
- When to return to hospital – ED/Specialist Clinics
Companion documents
- Nursing competency workbook – burns dressing, assessment, and fluid management of burns.
- Lund Browder chart
- Nursing Assessment
- Neurovascular Observations
- Extravasation guideline
- Pain Assessment and Measurement
- Procedure Management
- Nursing Documentation
- High Dependency and Special Nursing Care
- Immunisation of inpatients
- Child Abuse
- Aseptic technique
- Procedural sedation - ward and ambulatory areas
- Clinical Information
- Burns on the face
- Burns clinic at RCH
Evidence table
The evidence table for this nursing guideline can be found here .
Please remember to read the disclaimer .
The development of this nursing guideline was coordinated by Kate Glassford, Nurse Coordinator & Clinical Nurse Specialist Platypus Ward, and approved by the Nursing Clinical Effectiveness Committee. Updated July 2022.
- Nursing care plan for burns
- Nursing care plan

Introduction
Nursing diagnosis, interventions.
Burns are one type of injury to the skin caused by heat, electricity, chemicals, sunlight, or radiation. The main types of burns include thermal (heat/flame), electrical, chemical, and radiation. Nursing care plan for burns helps to ensure that the patient’s wounds are adequately treated and monitored for infection.
- Severity: It is determined from the depth and degree of injury. The severity of the burn is assessed in terms of the percentage of the body area affected.
- Pain: The intensity of pain and its character vary, depending on the extent and depth of the burn.
- Skin temperature: The skin temperature depends on the amount of edema as well as the nature of the burn.
- Circulation: Poor circulation can lead to poor healing and delays in wound closure.
- Infection: The risk of infection increases with the spreading of bacteria into the burn. Proper hygiene is essential.
- Fluid Volume Deficit : caused by excessive fluid loss through burn damage, exudates and evaporation.
- Pain : caused by tissue damage, manipulation of the wound, dressing changes and movement.
- Skin Integrity : caused by destruction of the epidermis through thermal, electrical, chemical and radiation sources.
- Infection : caused by entry of potentially pathogenic organisms into the skin.
- The patient will be free from infection.
- The patient will experience minimal pain.
- The patient will retain adequate body fluid volume.
- The patient will maintain skin integrity.
- Administer prescribed analgesics to relieve pain.
- Assess the burn wound daily to evaluate healing.
- Monitor vital signs and intake and output.
- Provide wound care as appropriate.
- Initiate measures to maintain fluid volume balance.
- Teach proper self-care of the burn.
- Analgesics help to relieve pain and discomfort.
- Assessment of the wound helps to monitor healing progress and detect infection.
- Fluid and electrolytes may be lost resulting in imbalance.
- Wound care helps to reduce pain and limit risk of further damage.
- Patients need to be taught how to care for their burn to ensure proper healing.
Evaluation of the effectiveness of the nursing care plan will be based on the patient's pain level, fluid balance, wound healing, and general condition. The patient should be monitored regularly and adjustments to the nursing care plan should be made accordingly.
The nursing care plan for burns is an important component of the overall medical management of the patient. By providing comprehensive assessment, accurate diagnosis, and effective interventions and outcomes, it helps to ensure successful treatment and recovery.
- What are the types of burns? Thermal (heat/flame), electrical, chemical, and radiation.
- What is the main goal of Nursing care plan for burns? The main goal of Nursing care plan for burns is to ensure that the patient’s wounds are adequately treated and monitored for infection.
- How are burns assessed? Burns are assessed in terms of severity, pain, skin temperature, and circulation.
- What nursing diagnosis should be included in a nursing care plan for burns? Fluid Volume Deficit, Pain, Skin Integrity, Infection.
- What are the interventions for nursing care plan for burns? Administer prescribed analgesics, assess the burn wound daily, monitor vital signs and intake and output, provide wound care, initiate measures to maintain fluid volume balance, and teach proper self-care of the burn.

Isabella White
Hello to all nursing enthusiasts! I'm Isabella White and I'm thrilled to welcome you to this space dedicated to the exciting world of nursing. Let me share a little about myself and what we can expect together on this journey. About Me: Nursing is more than just a profession to me, it's a calling. When I'm not caring for my patients or learning more about health and wellness, you'll find me enjoying the great outdoors, exploring new trails in nature, or savoring a good cup of coffee with close friends. I believe in the balance between caring for others and self-care, and I'm here to share that philosophy with you. My Commitment to You: In this space, I commit to being your reliable guide in the world of nursing. Together, we'll explore health topics, share practical tips, and support each other on our journeys to wellness. But we'll also celebrate life beyond the hospital walls, finding moments of joy in the everyday and seeking adventures that inspire us to live fully. In summary, this is a place where nursing meets life, where we'll find support, inspiration, and hopefully a little fun along the way. Thank you for joining me on this exciting journey. Welcome to a world of care, knowledge, and connection! Sincerely, Isabella White
- Nursing care plan for mobility
- Nursing care plan for postpartum depression
Nursing care plan for adhd
Nursing care plan for anaphylaxis
Nursing care plan for intellectual disability
Nursing care plan for rhabdomyolysis
Nursing care plan for psoriasis
Nursing care plan for arthritis
Nursing care plan for lung cancer
Nursing care plan for osteoarthritis
Nursing care plan for migraine
Nursing care plan for aortic valve replacement
Nursing care plan for influenza
Leave a Reply Cancel reply
Your email address will not be published. Required fields are marked *
Save my name, email, and website in this browser for the next time I comment.
Usamos cookies Más información
- Search Extension
- All of Oklahoma State University
Burn Plan for Prescribed Burning
Burn plan instructions, pre-burn preparations, pre-burn checklist, prescribed burn notification form, producer burn plan.
A burn plan helps to determine the safest and easiest way to complete tasks before, during and after a prescribed burn. The most important reason for having a burn plan is to thoroughly think about each action before striking the match. The burn plan will help determine where the burn should be conducted, what type of management is required before burning, how to conduct the burn, when to burn and what should be done after the burn.
A burn plan is a written prescription for the prescribed fire including critical elements such as the weather conditions under which the burn will be conducted, number of personnel and duties of each, and the type, amount and placement of equipment needed to safely conduct the burn. All of this information allows the fireboss to consider all actions prior to the burn, reducing many problems and complications. A burn plan also helps the fireboss consider any social impacts of the burn such as: smoke management concerns, traffic patterns or problems, how to contact neighbors and fire departments, along with other public safety issues. In rural areas many of these issues may not be of concern, but in areas associated with urban sprawl, it can be a major problem. Finally, a well-written burn plan can help reduce liability risk, which is a major concern for most people conducting prescribed burns. A burn plan can be used to show the amount of diligence and care used in planning and conducting the burn if some type of liability issue occurs.
No burn plan is perfect and no two are alike because they are as different as the burn units for which they are written. Each burn plan may require different information or planning, with some requiring more information about a specific topic than others. A burn plan should be written to meet local needs and be adapted to the region. The more experience a person has preparing plans, the easier it will become to write good ones. When preparing a burn plan, it is important not to limit implementation by being too specific with details or prescriptions. For example using weather conditions with a range that is too narrow and cannot be followed for the duration of the burn is not a prescription for success. Be sure to include all necessary information, but do not clutter a plan with pointless information that could cause confusion, or prevent the execution of a burn, and potentially increase liability.

Figure 1 . Burn plan map
The following instructions on completing a burn plan and the sample burn plan contained in this publication will assist anyone interested in conducting a prescribed burn. This burn plan provides information appropriate for most situations.
Information
Provide basic information about the unit and landowner/manger conducting the burn.
Description of Area to be Burned
Include pasture name, legal description and dominant vegetation type in the burn unit.
Vegetation Present
Describe the main vegetation/fuels present. Example – Tallgrasses, scatted shrubs with cedars <6 ft tall in the upland and solid stands of cedar >15 ft tall along the creek.
Directions from Nearest Town
Provide directions to the burn unit. This may be needed in case of an accident or escaped fire. In emergency situations, people often forget things as simple as providing directions to the burn unit. Also, someone not familiar with the area can provide directions from the burn plan to emergency responders. Objectives: Explain what the burn will accomplish. Objectives can be singular or multiple, along with being broad or very specific. Examples – Forage production for livestock, wildlife habitat management, cedar control, brush suppression, improve forage quality, hardwood reduction, fuel reduction and wildfire suppression.
Notification
List the names of fire departments, adjoining landowners, and others that need to be notified prior to conducting the burn. This allows the planner to have all phone numbers in one place for quick reference. It also provides a place for the planner to enter the date, time and person notified, which can be helpful if problems arise or for verification of notification.
Describe what should be done before conducting burn.
Management Needed Prior to Burn
Describe management required to prepare for the burn in order to meet objectives. These practices could include grazing management, mechanical treatments to make the burn safer or more effective, or the protection of specific areas or items.
Firebreak Types and Location Around the Burn Unit
Describe the type of firebreaks used and the location of each around the burn unit. Firebreaks can be disked, dozed, roads, cultivated fields or natural breaks like creeks. Example- Firebreaks on the west and north side of the burn unit are disked strips 15 feet in width and the east and south firebreaks are comprised of a two-track pasture road.
For more information about firebreaks see Extension Fact Sheet NREM-2890 , Firebreaks for Prescribed Burning.
Fuel Conditions
Record the amount and continuity of fine fuel (herbaceous vegetation) desired for the burn and actual amount in the burn unit on the day of the burn. Fine Fuel Amounts: Determined by visual estimation or by clipping and weighing samples.
Fuel Continuity
Describes the amount of coverage or distribution of fuels. This is important for fire spread. Many times there may be adequate fuel amounts, but fuel continuity will not allow the fire to spread or carry across the burn unit.
Prescribed Weather Conditions
Define the weather conditions needed to safely and effectively conduct the burn.
Desired Range
Describes ideal weather conditions for the burn.
Maximum Range
Upper and lower weather conditions allowable for the burn. These ranges allow flexibility in order to account for daily weather variation. Example- Relative humidity desired range 40 percent to 60 percent, maximum range 20 percent to 80 percent.
For more information about weather conditions for prescribed burning, see Extension Fact Sheet NREM-2878 , Fire Prescriptions for Maintenance and Restoration of Native Plant Communities.
Smoke Management Considerations
Identify and list smoke sensitive areas around the burn unit and with what wind direction and dispersion conditions will be needed to reduce smoke impacts. Example- Due to road on west side of burn unit and homes to the south of burn unit, a west or southwest wind is needed to reduce smoke impacts. Attach a smoke dispersion forecast map to the burn plan. Smoke sensitive areas can be roads, communities, airports and houses.
Other Smoke Management Considerations
Category day can be determined from the National Weather Service Fire Weather websites Go to www.weather.gov , select your region from map, then select fire weather).
Dispersion Condition
Information can be found at sites like OK-Fire or Kansas Flint Hills Smoke Management .
For more information about smoke management see Extension circular E-1008, Smoke Management for Prescribed Burning.
This allows the planner to determine if there are potential problems within or around the burn unit and what could be done to reduce or eliminate them. Example – Brush piles are present along firebreaks and will be pushed a minimum of 300 feet inside the burn unit.
Observed Weather
On the day of the burn, record on-site weather conditions before, during and after the burn.
List equipment that is needed or might be needed to conduct the burn. It also provides area for recording what was actually on the burn.
Crew Members
List the number of people needed to safely conduct the burn. On the day of the burn, record names of the people comprising the burn crew.
Ignition Plan
Describe the ignition sequence(s) required to ignite the burn safely. This forces the planner to consider in what sequence the burn crew(s) will move around the burn unit igniting the fire and potential problems or hazardous areas that should be addressed. Describe each sequence in writing and draw them on a map of the burn unit. See sample plan on how to write ignition plan and draw an ignition plan map.
Go-No Go Check List
List items needed and tasks to be done prior to conducting the burn. The fireboss should review this list prior to conducting the burn to make sure everything is in order.
Escaped Fire Plan
This is a step-by-step action plan describing what should be done if the fire escapes and the proper procedures for controlling an escaped fire.
Signature Box
Signed and dated by the preparer when the plan is finished.
In Oklahoma, this form should be completed and attached to the burn plan. Doing so may limit liability in the event of an escaped fire. A copy of this form should also be filed with the nearest rural volunteer fire department and if in the forestry protection area, a copy must be provided to the local Forestry Services Division office or representative. This portion of the electronic fire plan version will automatically be filled in with information from the fire plan. The only blank that will need to be filled in is the date of previous burn. For more information see Forestry Services Division publication “Notification Requirements and Considerations for Safe and Lawful Prescribed Burning in Oklahoma.”
The following sample prescribed burn plan is to show how the burn plan is filled out, along with examples of smoke management, written and mapped ignition plans.
Figure 2a . First page of prescribed burn plan
Figure 2b . Second page of prescribed burning plan
Figure 2c . Third page of prescribed burning plan
Figure 2d . Fourth page of prescribed burning plan
Figure 2f . Fifth page of prescribed burning plan
Figure 2g . Sixth page of prescribed burning plan
Figure 3 . Burn map attachment
With a southwest wind ignition will start in the northeast corner at point A (see attachment C). Crew will be divided into two groups, crew 1 (east) and crew 2 (west). Equipment will be divided between both groups with 1 UTV and the 200 gallon pumper going with Crew 1 since that firebreak is rough and harder to traverse. The 300 gallon pumper and other UTV will go along the north line. Ignition will consist of strip heaffires using a minimum of 2 torches starting at Point A with Crew 1 going south along the east line stopping at Point B and Crew 2 going west along the north line stopping at Point C. A blackened area of 300 ft wide minimum will need to be established before either Crew can proceed. The UTV’s will patrol their respective lines, while the pumpers will be positioned in problem areas and moved as needed. Once adequate black is established one torch from each crew will begin igniting the headfire and meet at Point D. While the headfire is being ignited equipment and crew will continue to monitor the east and north lines. Equipment will be moved to the west and south lines as needed. Crew 2 should take extra caution along the west side due to traffic on Coyle Road.
Figure 4.
Producer burn plan form
John R Weir Research Associate Natural Resource Ecology and Management
J. Derek Scasta Graduate Research Associate Natural Resource Ecology and Management
Russell Stevens Wildlife and Range Consultant Samuel Roberts Noble Foundation
Terrence G Bidwell Extension Range Specialist Natural Resource Ecology and Management
Was this information helpful?
By Ryan DeSantis. Learn the best methods to use firewood as an indoor heating source in Oklahoma.
By Ryan DeSantis. Learn about factors that affect stumpage prices, 2023-2024 price trends and the 2024 marketing outlook.
By Hannah M. Baker, Hannah E. Shear, Derrell S. Peel, Kellie Curry Raper, Samuel D. Fuhlendorf. Learn about the implementation, cost and benefits of patch-burn grazing.
By Dwayne Elmore, Don Wolfe, Kevin Allen. Learn about the effects of lead ammunition and sinkers on wildlife.
- Practice Test
- Fundamentals of Nursing
- Anatomy and Physiology
- Medical and Surgical Nursing
- Perioperative Nursing
- Psychiatric Mental Health Nursing
- Maternal & Child Nursing
- Community Health Nursing
- Pathophysiology
- Nursing Research
- Study Guide and Strategies
- Nursing Videos
- Work for Us!
- Privacy Policy
- Nursing Care Plan
Patients Suffering from Burns Nursing Care Plan [Actual and Risk Diagnoses]

Burns, or burn injuries, result from tissue damage due to heat transfer from one site to another. In most cases, this heat is much more than the skin can withstand, leading to disruption in the skin’s integrity and other problems such as fluid loss, increased risk for infection, ineffective thermoregulation, and aesthetic appearance and body image issues of the patient.
Among patients at the highest risk for developing complications related to burn injuries are those who are very young and very old. This is due to the percentage of body fluids among these patients, their ability to heal from tissue injuries, and the existence of other comorbid conditions such as coronary artery diseases, diabetes mellitus , cancer, and others. Also, because the severity of the burn injuries worsens the longer it persists, there is a need for the nurse to properly assess and diagnose patients’ needs that require immediate attention while ensuring that problems at the highest risk to develop are prevented if not eliminated.
Burns are classified according to their thickness and degree of injury. These are made to denote the extent of tissue injury and destruction and help in planning interventions to minimize the complications that the injury can bring about to the patient. Classification according to thickness include:
- Superficial partial-thickness burns- in this type of injury, only the epidermis is damaged, but some portions of the dermis may also be injured.
- Deep partial-thickness burns- this type is characterized by the full injury of the epidermis, and involvement of the upper layer and deeper portions of the dermis.
- Full-thickness burns – as the name implies, full-thickness burns involve the destruction of both the dermal and epidermal layers as well as the involvement of the surrounding tissues, muscles and even bones.
Burns may also be classified according to the degree of tissue involvement (see Fig.1 for representation). These are:
- First Degree Burns- this classification is made when the burn injury only affects the outer layer of the skin and is characterized by the presence of red, painful and dry skin surrounding the injury. This is the most painful of all types of injury because of the exposure of naked nerve endings.
- Second Degree Burns- this involves damage to the entire epidermis and some portions of the dermis that is characterized by the presence of red, painful and oftentimes blistered areas. In some cases, edema and swelling are also part of the assessment findings.
- Third Degree Burns- also called full-thickness burns, involves the destruction of both the dermis and the epidermis and sometimes goes into the innermost layers of the skin. The burnt site usually looks whitish, charred or even blackened.
- Fourth Degree Burns- this type of burn injury goes through all layers of the skin, muscles and bone. In this type of injury, there is eschar formation and the patient usually does not feel anything at the site of injury.

While the problem with burns is mostly integumentary, there are also other nursing problems that can be seen among patients.
Burns Nursing Care Plan
There are a number of nursing diagnoses (both risk and actual problems) for burns that the nurse can identify based on assessment findings such as:
- Ineffective airway clearance
- Impaired gas exchange
- Impaired/Alteration in skin integrity
- Risk for/Fluid volume deficit
Risk for Infection
- Body Image Disturbance
Assessment of the patient will need to be structured to ensure that the patient will not be stressed unnecessarily and that the nurse will be able to fully identify the signs and symptoms indicative of the health problem. Moreover, the assessment for potential or at risk health problems should be made thoroughly and any intervention to prevent it must be aligned to the overall care plan for the patient. Below are examples of care plans for 2 actual and 2 potential/risk problems for patients suffering from burns .
Ineffective Airway Clearance
Ineffective airway clearance related to increased/increasing congestion in the airway passages secondary to smoke inhalation as evidenced by presence of inspiratory and expiratory wheezing, sooty sputum production, persistent cough and use of accessory muscles when breathing.
Desired Outcomes
After nursing interventions, the patient is expected to:
- Demonstrate improved airway patency as evidenced by clear breath sounds
- Have decreased coughing episodes
- ABGs and other laboratory values within normal limits
| Assess vital signs, focusing on respiratory rate and rhythm, depth of respirations and symmetrical chest expansions | Vital signs assessment can help provide the nurse information on the extent of airway impairment that the injury causes to the patient. This also helps set the baseline for evaluation of care. |
| Observe the patient for other signs of inhalation injury such as damage to the circumoral mucosa, burns along the nostrils, face or neck. | These surrounding structures are also important in air exchange and may cause disruptions in airway clearance when injured or damaged. |
| Position the patient in semi-Fowler’s or high Fowler’s position. | Positioning the patient this way helps in promoting optimal lung expansion and removal of secretions. It also allows the patient to be positioned comfortably. |
| Provide the patient with oxygen therapy when needed. | Humidified oxygen therapy helps meet the needs of the patient for tissue perfusion and reduces the risk for hypoxia. |
| If the patient is on oxygen therapy, monitor the ABGs as needed. | ABGs are a good indicator of the oxygenation status of the patient along with the pulse oximetry readings. Changes in these readings should be documented and reported to the physician when needed. |
| Instruct patient and significant others on how to turn patient properly on bed, coughing and deep breathing exercises and use of incentive spirometer. | These all help in establishing a patent airway, maintaining optimum lung capacity and promote independence for self-care. |
Alteration/Impairment in Skin Integrity
Impaired skin integrity related to damage to the skin and surrounding tissues sec0ndary to burn injury as evidenced by (indicate the signs seen on patient depending on the thickness/degree of the burn injury).
- Manifest increased capacity for wound healing
- Cooperate with a plan of care for burn wounds
- Have reduced risk to develop infections secondary to wounds
| Assess the status of the burned area, noting the degree of tissue involvement and extent of the damage. | Knowing exactly the wound coverage helps in planning for care of the patient. |
| Determine the type of irritating agent that caused the wound. | There are specific care requirements for some type of wounds depending on the nature of injury (i.e., thermal vs. chemical). Knowing these would help the nurse in planning appropriate care for the patient. |
| Provide patient support during the initial phases of wound care. | In some cases, the initial phases of wound care for burns may be painful and distressing to the patient, especially when these involve debridement. Providing the patient support eases stress and anxiety and helps the patient to cooperate in his care plan. |
| Involve the patient and his significant others in performing wound care and dressing changes. | This action helps to promote independent self-care for the patient and collaboration between the patient, his significant others and the members of the health team. |
| Administer medications as prescribed. | These substances are prescribed to the patient to help promote tissue growth, wound healing and in some cases, prevent the formation of keloids. |
| Stress the importance of asepsis, especially when handling wounds. | This helps prevent infections at the wound site. |
| Make a referral to physical/occupational therapy when needed. | In cases where a wound affects the functionality of a certain part of the body, the patient may need to be referred to a PT/OT to help promote optimal functioning. |
| Consider referring to cosmetic/aesthetic surgery and/or other support groups when needed. | Severe damage to the skin may need to be aesthetically reconstructed and the patient may need counseling or therapy to help deal with the potential for body image problems later on. |
Risk for Fluid Volume Deficit
Risk for fluid volume deficit related to loss of fluids through abnormal routes secondary to burn injury
Note: “evidenced by” is not usually applicable for a risk diagnosis since the presence of signs and symptoms already makes the nursing problem an actual diagnosis.
After nursing interventions, the patient is expected to (choose the factor that is related to the factor that poses as a risk):
- Establish normal fluid volume
- Minimize unnecessary fluid losses
- Increase intake of oral fluids (if allowed, and/or tolerated)
| Monitor vital signs while paying close attention to monitoring the hourly urine output, central venous pressures, cardiac output and pulmonary artery pressures. | These are indicative of the hemodynamic status of the patient and would alert the nurse if the patient suffers from dehydration or overhydration. |
| If needed, calculate fluid volume replacement needs by the patient and infuse accordingly. | During the initial stages after a burn injury, there is a need to ensure that fluid volume need replacement is established. In some cases, Parkland Formula is used to calculate the fluid needs for the first 24 hours:
BSA (% burned) x 4 x Body Weight (in kg)
The resulting volume will then be divided by 2, with the first 50% of the volume infused over an 8 hour period, while the remaining 50% infused in a 16-hour timeframe. |
| Ensure patency of IV lines and encourage the patient to take fluids orally (if not contraindicated) and document. | This helps ensure adequate fluid volumes are restored and maintained and the risk for fluid volume deficit is minimized. |
| Monitor serum electrolyte levels regularly. | To help determine developing electrolyte imbalances and to correct them early on. |
| Position patient comfortably on the bed and maintain the room temperature at a comfortable level. | This helps relax the patient while ensuring that room temperature does not promote drying of the skin or excessive sweating |
| Notify physician immediately when the patient assessment reveals reduced urine output, reduction in blood pressure or lowering of other indicators of hemodynamic status. | Early identification of these symptoms can help the health care team address any hemodynamic imbalances on the patient and restore normal fluid volume. |
Risk for infection related to decreased primary defenses secondary to burn injury
After the nursing interventions, the patient is expected to:
- Have reduced risk for developing wound infections
- Verbalize knowledge on maintaining aseptic technique in handling wounds
- Manifest enhanced capacity to promote wound healing
| Institute the use of the aseptic technique in handling wounds. | This helps ensure that infective agents and microorganisms are limited from coming in contact with the wound site and the risk of infection is reduced. |
| Adhere to the wound changing and dressing schedule, noting carefully the times when dressings need to be changed. | This helps promote adequate wound healing and avoid infection by ensuring that the dressings remain free of moisture so it does not harbor microorganisms. |
| Remind the patient to avoid touching the wound, only touching it during wound dressings. | The hand is one of the worst contaminants of wounds and frequent touching increases the risk of infections. Only touching it during wound dressings would reduce the risk for infection dramatically. |
| Prevent the skin surfaces from rubbing together and ensure that the surrounding skin is kept clean and dry, | Excessive moisture or dryness of the skin can cause further breaks in skin integrity and rubbing skin surfaces together may cause micro lacerations which can eventually become a portal of entry for other microorganisms. |
| Increase intake of foods rich in protein and vitamin C. | Protein is essential for tissue growth and repair while vitamin C can help restore vessel integrity and increase immune system response. |
- Doenges, M. E., Moorhouse, M. F., & Murr, A. C. (2019). Nurse’s pocket guide: Diagnoses, prioritized interventions, and rationales. Philadelphia: F.A. Davis.
- Carpenito, L. (2016). Handbook of Nursing Diagnosis (15th ed.).
- Herdman, T., & Kamitsuru, S. (2018). NANDA International, Inc. nursing diagnoses (11th ed.).
- Brunicardi, F., & Anderson, D. (2015). Schwartz’s principles of surgery. (includes DVD) . New York: McGraw-Hill.
RELATED ARTICLES MORE FROM AUTHOR
Diarrhea nursing care plan 2024 updates, urinary tract infection nursing care plan, anemia nursing care plan, hiatal hernia nursing care plan, pulmonary embolism nursing care plan, pleural effusion nursing care plan.
Thank you for this, i used your content for my class presentation and it was great
Thank you for the great content! Will cite your work in a discussion board.
Thanks, it’s very usefull
i am a third year nursing student and i fine the information to be very informative
I really appreciate the website and its content.
thank you very informative
LEAVE A REPLY Cancel reply
Save my name, email, and website in this browser for the next time I comment.

Initial assessment and management of burn patients
Your quick action can help decrease morbidity and mortality, shorten hospital stays, and reduce costs..
- Large total body surface area burns require immediate and aggressive assessment and management from well-trained nurses in a variety of settings.
- Patients’ responses to treatment need to be carefully and frequently monitored to prevent complication and improve survival.
In 2016, more than 200,000 people in the United States were hospitalized with injuries from smoke, fire, or flame exposure; more than 6,000 died. (See Facts and figures .) Burns damage skin and underlying tissue, disrupting the skin’s regulatory functions. Patients with acute burns require significant and costly interprofessional care that includes nurses, advanced practitioners, surgeons, pharmacists, physical and occupational therapists, and social workers.

The ABCDEs of emergency burn care
Excessive opioids lead to a close call for a burn patient
How to recognize and respond to hypovolemic shock
Proper initial management of a patient with serious burns can have significant impact on his or her long-term health outcomes. (See Skin and burns .)

Primary assessment
Primary assessment of patients with acute burns starts with airway patency and cervical spine protection (in cases of a suspected spinal cord injury or if the patient is un-conscious and you have no other sources of information about the accident). Assess breathing, central and peripheral circulation, and cardiac status; stabilize any disability, deficit, or gross deformity; and remove clothing to assess the extent of burns and concurrent injuries.
Airway assessment includes visualizing the upper airway to look for obstructions, edema, or evidence of burn (soot; singed nasal hairs, eyebrows, facial hairs; raspy voice; cough). Place an oral pharyngeal device to protect an unconscious patient’s airway. If you see edema or evidence of burn in the upper airways, assess whether an endotracheal (ET) tube is needed to maintain the airway. There may be only a small window of opportunity to easily place an ET tube because edema from burn shock may obstruct the airway. If you suspect cervical spine injury, apply immobilization with a collar before doing anything that will flex or extend the neck.
Auscultate breath sounds and inspect and palpate the patient’s chest wall. Unless an ET tube is required, start high-flow oxygen at 15 L on a non-rebreather mask with concurrent partial pressure of carbon di- oxide monitoring on every patient with burns. Circumferential burns at the neck or torso may impair ventilation, and other conditions (such as pneumothorax) may cause respiratory distress. Help advanced practice providers perform procedures (bedside escharotomies to release constrictive eschar, needle decompression to relieve a tension pneu- mothorax, chest tube placement to drain fluid buildup) to improve the patient’s work of breathing.
Vital signs
Monitoring vital signs and the color of unburned skin can help you assess the patient’s circulatory and cardiac status. Carefully check pulses in any extremity with circumferential burns. These burns can act as tourniquets as burn-associated edema begins, leading to compartment syndrome. Heart rate (HR) in most adult burn patients will be elevated to 100 to 120 beats per minute (bpm) because of increased circulating catecholamines and hypermetabolism; HR higher than that may indicate hypovolemia from trauma, inadequate oxygenation, or uncontrolled pain and anxiety. Blood pressure and other vital signs in early stages of burn resuscitation should be the same as the patient’s baseline. Arrhythmias may be seen in electrical burn injuries, electrolyte imbalances, or underlying cardiac abnormalities. Begin interventions as ordered to avoid complications.
Neurologic assessment
In most cases, neurologic status won’t be altered in the early stages of burn injury. Determine if the patient is alert, responsive to verbal and pain stimuli, or unconscious. If the patient isn’t alert and oriented upon arrival, consider an associated injury, carbon monoxide poisoning, substance abuse, hypoxia, or preexisting medical conditions and intervene as appropriate. Use the Glasgow Coma Scale to trend the patient’s neurologic status throughout resuscitation.
Skin exposure
To prevent increased depth of injury, remove any causative burn agent from the skin and immediately flush the affected area with tepid water. However, use caution to pre- vent a rapid drop in body temperature and subsequent ventricular fibrillation or asystole. Don’t use ice to cool the area; it can further damage the skin or cause hypothermia. Remove all of the patient’s clothing, jewelry, shoes, diapers, and contact lenses to stop the burning process and prevent the items from becoming tourniquets when edema develops. To preserve core body temperature, cover the patient and the burn wounds with clean sheets or blankets, use warmed fluids, and maintain a warm environment.
If the patient needs more care or resources than currently available, prepare him or her for transport to the nearest burn center. Critically ill and multiple trauma patients, specialty population patients (such as children), and those who need additional technology may require transfer. The American Burn Association (ABA) has identified patients who are best served at a burn center .
Secondary assessment
The secondary assessment shouldn’t begin until the primary assessment is complete; resuscitative efforts are underway; and lines, tubes, and catheters are placed. (See Supporting the patient with burns .) This assessment includes a complete history, such as information about the burn injury, head-to-toe physical examination, accurate calculation of the percentage total body surface area (%TBSA) affected, fluid resuscitation requirements, and wound care.

If you can’t gather a history from the patient, interview family members, friends, or those who were at the scene. In addition to the patient’s medical history, record detailed information about the circumstances and mechanism of the injury. Additional questioning will be necessary if the patient was found in an enclosed space, has potential orthopedic injuries associated with the burns, or had clothing on fire. Data collected in these circumstances can significantly change your plan of care. For example, inhalation in closed spaces may involve toxins, which will prompt the provider to order additional tests. And burns to the face may significantly impact the airway. You’ll also want to gather addition- al information if an accelerant was used, an explosion was witnessed, the burn is related to a motor vehicle accident, or the reported circumstances are inconsistent with the burn pattern (suspected abuse).
Lab work and tests
A variety of laboratory tests will be needed within the first 24 hours of a patient’s admission (some during the initial resuscitative period and others after the patient is stab lized). Every patient will have complete blood count, electrolytes, blood urea nitrogen, creatinine, and glucose levels drawn. If the burn occurred in an enclosed space, arterial blood gas and carboxyhemo- globin levels will be needed because toxins in the air can cause carbon dioxide to displace oxygen in red blood cells; an arterial blood gas is also helpful if an inhalation injury is suspected.
Other tests include:
electrocardiogram— done at baseline before fluids are started because cardiac arrhythmias may occur during early stages of resuscitation for large burns
chest X-ray— to detect fluid accumulation, position of the ET tube (if intubation is required), or atelectasis caused by large-volume fluid resuscitation
serum lactate— helps detect acid-base imbalance and may help in predicting survival
cyanide level— done if unexplained lactic acidosis occurs; patients with smoke inhalation are at risk for cyanide toxicity
blood type and crossmatch— for patients with severe trauma in addition to burns who might need blood or blood products
urine myoglobin, serum creatine kinase— help detect injuries to kidneys or muscles and used to help diagnose rhabdomyolysis, which can occur with electrical or extensive third-degree burns. Tetanus immunization should be administered in any patient with burns deeper than superficial.
Burns create a large open wound in which normal skin flora can begin to colonize. Left untreated, this can lead to severe cellulitis or sepsis. Wound care is essential to prevent infection and should be performed immediately after completing primary and secondary assessments and any life-or limb-threatening conditions are treated. After pre-medicating the patient with an analgesic agent to reduce pain, thoroughly wash the area with water and skin disinfectants or antibacterial soap. Clean away materials found on the wound and debride large ruptured blisters. Using a strip pattern, apply antibacterial ointment and nonadherent gauze to any open areas. Keep the gauze loose enough to allow for swelling and secure it with tape.
Additional interventions to prevent infection include:
- give daily baths with skin disinfectants
- perform wound care wearing isolation gown, mask, and surgical cap
- implement strict staff and visitor handwashing policies
- change lines every few days per institutional policy
- minimize performing interventions through nonintact skin.
If the patient develops a high fever, he or she may be pancultured and prescribed broad-spec- trum antibiotics until a specific organism is identified.
Fluid resuscitation
Most burn centers use a modified Parkland formula to calculate total fluid volume requirements, taking into account %TBSA and the patient’s body weight. (See Parkland formula .) This formula helps determine fluid needed from loss and shifts related to the injury, as well as insensible losses, and loss through nonintact skin.

After a total volume is calculated, half of that volume is given in the first 8 hours after the time of the injury, 25% in the second 8 hours, and the final 25% in the last 8 hours. If you don’t see the patient until 2 to 3 hours after he or she sustained the injury, you’ll have to catch up quickly. Use the patient’s urine output and physiologic response to determine if the volume is adequate for resuscitation. Consistently reassess for treatment effectiveness and make adjustments as necessary. Count fluids given via other methods (including I.V. medication diluents and nasogastric tube feeding) in the fluid calculation.
Fluid shifting that occurs with large %TBSA burns are a result of shock, which moves the circulating volume into the soft tissue and creates hypovolemia in the first 48 hours after the injury. Rapid and aggressive fluid resuscitation is needed to replace intravascular volume and maintain end-organ perfusion. The fluid in the damaged area will exit via the open wound, increasing the amount of fluid needed by the whole body to maintain homeostasis. Although crystalloids like lactated Ringers are the preferred volume-replacement therapy, some patients will require colloids, such as albumin, to retain as much fluid as possible inside the vessels. During initial resuscitation (the first 24 hours), reassess the patient’s responsiveness to treatment hourly and follow protocols for adjusting fluid based on urine output. In the case of delayed resuscitation, assess the patient’s volume status every 24 hours, looking for fluid overload and other complications, such as rhabdomyolysis, rising lactate levels, acid-base imbalances, and compartment syndrome resulting from all the fluids given during resuscitation.
Pain and anxiety
Pain at the secondary assessment will vary based on injury depth and the amount of nerve involvement; a variety of nonpharmacologic interventions can reduce pain and allow you and other members of the healthcare team to provide treatments and therapies, such as dressing changes and physical and occupational therapy, that many burn patients can’t tolerate without medication. If no contraindications exist, the head of the bed should be elevated at least 30 degrees throughout resuscitation. In addition, elevate affected extremities above the level of the heart to de- crease edema and subsequent pain. Wounds, especially partial thickness and superficial burns, will be most painful when ex- posed to air, so perform dressing changes efficiently with only one exposed area at a time. Premedicating the patient (for example, with I.V. fentanyl or hydromorphone) and warming the room will improve the experience for both you and the patient. When possible, group painful interventions to be performed at the same time.
Psychosocial and the resulting responses to burn trauma vary. Be prepared to provide emotional sup- port throughout the resuscitation process. To help you engage in therapeutic communication and develop a rapport with the patient, talk him or her through interventions, refrain from making judgmental comments or giving unsolicited advice, and acknowledge rather than trivialize feelings of depression, guilt, fear, or anger. Advocate for psychiatric support by helping to connect the patient with survivor and family support groups; information is available at the ABA website .
Act quickly
When a patient presents with a deep burn or a burn covering a large %TBSA, quickly assess and intervene to prevent systemic and localized complications. Your interventions will be based on the type, extent, depth, and degree of the burn, as well as concurrent injuries. Early diagnosis and treatment lead to improved morbidity and mortality, shorter hospital stays, and decreased costs.
The authors work at the University of Cincinnati College of Nursing in Cincinnati, Ohio. Sarah Strauss is a nurse practitioner in the division of plastics, reconstructive, burn, and hand surgery. Gordon L. Gillespie is an associate professor.
American Burn Association (ABA). Advanced Burn Life Support Course: Provider Manual, 2017 Update . Chicago: ABA; 2017.
American Burn Association. Burn incidence and treatment in the United States: 2016 . 2017.
Herndon DN. Total Burn Care . 5th ed. London, England: Elsevier; 2018.
Lai-Cheong JE, McGrath JA. Structure and function of skin, hair and nails. Medicine . 2017;45(6):347-351.
1 Comment .
Excellent article. It was helpful since it was directed more toward nursing.
Comments are closed.

NurseLine Newsletter
- First Name *
- Last Name *
- Hidden Referrer
*By submitting your e-mail, you are opting in to receiving information from Healthcom Media and Affiliates. The details, including your email address/mobile number, may be used to keep you informed about future products and services.
Test Your Knowledge
Recent posts.

From Retirement to Preferment: Crafting Your Next Chapter

States Set Minimum Staffing Levels for Nursing Homes. Residents Suffer When Rules Are Ignored or Waived

Diabetic foot ulcers in ambulatory settings
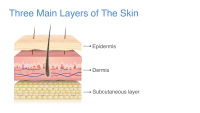
Skin integrity and steroid medications

Lyme carditis: A clinical case report

Examining Public Perception of Nurses

From the Midwest to the Middle East
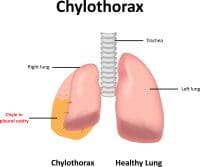
Chylothorax: A stepwise approach to care

Aortic dissection

Known fallers

Florence Nightingale overcame the limits set on proper Victorian women – and brought modern science and statistics to nursing

Bird flu is bad for poultry and dairy cows. It’s not a dire threat for most of us — yet.

Knowledge of intravascular determination

Chronic traumatic encephalopathy and traumatic brain injury

Nearly 100 measles cases reported in the first quarter, CDC says
Taking Care of Patients with Burn Injury: Episode 180
How to Write a Nursing Care Plan
Nursing care plan components, nursing care plan fundamentals.

Knowing how to write a nursing care plan is essential for nursing students and nurses. Why? Because it gives you guidance on what the patient’s main nursing problem is, why the problem exists, and how to make it better or work towards a positive end goal. In this article, we'll dig into each component to show you exactly how to write a nursing care plan.
Popular Online RN-to-BSN Programs
Enrollment: Nationwide

WGU's award-winning online programs are created to help you succeed while graduating faster and with less debt. WGU is a CCNE accredited, nonprofit university offering nursing bachelor's and master's degrees.

- RN to BSN - Global Studies

When you earn an ASU nursing degree, you are gaining skills from a respected and accredited institution. Our online nursing degrees are accredited by the Arizona State Board of Nursing and the Commission on Collegiate Nursing Education.

A nursing care plan has several key components including,
- Nursing diagnosis
- Expected outcome
- Nursing interventions and rationales
Each of the five main components is essential to the overall nursing process and care plan. A properly written care plan must include these sections otherwise, it won’t make sense!
- Nursing diagnosis - A clinical judgment that helps nurses determine the plan of care for their patients
- Expected outcome - The measurable action for a patient to be achieved in a specific time frame.
- Nursing interventions and rationales - Actions to be taken to achieve expected outcomes and reasoning behind them.
- Evaluation - Determines the effectiveness of the nursing interventions and determines if expected outcomes are met within the time set.
>> Related: What is the Nursing Process?
Get 10% OFF Nursing School Study Guides From nurseinthemaking.com ! Fill out the form to get your exclusive discount.
Before writing a nursing care plan, determine the most significant problems affecting the patient. Think about medical problems but also psychosocial problems. At times, a patient's psychosocial concerns might be more pressing or even holding up discharge instead of the actual medical issues.
After making a list of problems affecting the patient and corresponding nursing diagnosis, determine which are the most important. Generally, this is done by considering the ABCs (Airway, Breathing, Circulation). However, these will not ALWAYS be the most significant or even relevant for your patient.
Step 1: Assessment
The first step in writing an organized care plan includes gathering subjective and objective nursing data . Subjective data is what the patient tells us their symptoms are, including feelings, perceptions, and concerns. Objective data is observable and measurable.
This information can come from,
Verbal statements from the patient and family
Vital signs
Blood pressure
Respirations
Temperature
Oxygen Saturation
Physical complaints
Body conditions
Head-to-toe assessment findings
Medical history
Height and weight
Intake and output
Patient feelings, concerns, perceptions
Laboratory data
Diagnostic testing
Echocardiogram
Step 2: Diagnosis
Using the information and data collected in Step 1, a nursing diagnosis is chosen that best fits the patient, the goals, and the objectives for the patient’s hospitalization.
According to North American Nursing Diagnosis Association (NANDA), defines a nursing diagnosis as “a clinical judgment about the human response to health conditions/life processes, or a vulnerability for that response, by an individual, family, group or community.”
A nursing diagnosis is based on Maslow’s Hierarchy of Needs pyramid and helps prioritize treatments. Based on the nursing diagnosis chosen, the goals to resolve the patient’s problems through nursing implementations are determined in the next step.
Get 5 FREE study guides from Simplenursing.com - fill out the form for instant access! 1. Fluid & Electrolytes study guide 2. EKG Rhythms study guide 3. Congestive Heart Failure study guide 4. Lab Values study guide 5. Metabolic Acidosis & Alkalosis study guide

By clicking download, you agree to receive email newsletters and special offers from Nurse.org & Simplenursing.com. You may unsubscribe at any time by using the unsubscribe link, found at the bottom of every email.
Your request has been received. Thanks!
There are 4 types of nursing diagnoses.
Problem-focused - Patient problem present during a nursing assessment is known as a problem-focused diagnosis
Risk - Risk factors require intervention from the nurse and healthcare team prior to a real problem developing
Health promotion - Improve the overall well-being of an individual, family, or community
Syndrome - A cluster of nursing diagnoses that occur in a pattern or can all be addressed through the same or similar nursing interventions
After determining which type of the four diagnoses you will use, start building out the nursing diagnosis statement.
The three main components of a nursing diagnosis are:
Problem and its definition - Patient’s current health problem and the nursing interventions needed to care for the patient.
Etiology or risk factors - Possible reasons for the problem or the conditions in which it developed
Defining characteristics or risk factors - Signs and symptoms that allow for applying a specific diagnostic label/used in the place of defining characteristics for risk nursing diagnosis
PROBLEM-FOCUSED DIAGNOSIS
Problem-Focused Diagnosis related to ______________________ (Related Factors) as evidenced by _________________________ (Defining Characteristics).
RISK DIAGNOSIS
The correct statement for a NANDA-I nursing diagnosis would be: Risk for _____________ as evidenced by __________________________ (Risk Factors).
Step 3: Outcomes and Planning
After determining the nursing diagnosis, it is time to create a SMART goal based on evidence-based practices. SMART is an acronym that stands for,
It is important to consider the patient’s medical diagnosis, overall condition, and all of the data collected. A medical diagnosis is made by a physician or advanced healthcare practitioner. It’s important to remember that a medical diagnosis does not change if the condition is resolved, and it remains part of the patient’s health history forever.
Examples of medical diagnosis include,
Chronic Lung Disease (CLD)
Alzheimer’s Disease
Endocarditis
Plagiocephaly
Congenital Torticollis
Chronic Kidney Disease (CKD)
It is also during this time you will consider goals for the patient and outcomes for the short and long term. These goals must be realistic and desired by the patient. For example, if a goal is for the patient to seek counseling for alcohol dependency during the hospitalization but the patient is currently detoxing and having mental distress - this might not be a realistic goal.
Step 4: Implementation
Now that the goals have been set, you must put the actions into effect to help the patient achieve the goals. While some of the actions will show immediate results (ex. giving a patient with constipation a suppository to elicit a bowel movement) others might not be seen until later on in the hospitalization.
The implementation phase means performing the nursing interventions outlined in the care plan. Interventions are classified into seven categories:
Physiological
Complex physiological
Health system interventions
Some interventions will be patient or diagnosis-specific, but there are several that are completed each shift for every patient:
Pain assessment
Position changes
Fall prevention
Providing cluster care
Infection control
Step 5: Evaluation
The fifth and final step of the nursing care plan is the evaluation phase. This is when you evaluate if the desired outcome has been met during the shift. There are three possible outcomes,
Based on the evaluation, it can determine if the goals and interventions need to be altered. Ideally, by the time of discharge, all nursing care plans, including goals should be met. Unfortunately, this is not always the case - especially if a patient is being discharged to hospice, home care, or a long-term care facility. Initially, you will find that most care plans will have ongoing goals that might be met within a few days or may take weeks. It depends on the status of the patient as well as the desired goals.
Consider picking goals that are achievable and can be met by the patient. This will help the patient feel like they are making progress but also provide relief to the nurse because they can track the patient’s overall progress.
>> Show Me Online RN-to-BSN Programs
Nursing care plans contain information about a patient’s diagnosis, goals of treatment, specific nursing interventions, and an evaluation plan. The nursing plan is constantly updated with changes and new subjective and objective data.
Key aspects of the care plan include,
Outcome and Planning
Implementation
Through subjective and objective data, constantly assessing your patient’s physical and mental well-being, and the goals of the patient/family/healthcare team, a nursing care plan can be a helpful and powerful tool.
*This website is provided for educational and informational purposes only and does not constitute providing medical advice or professional services. The information provided should not be used for diagnosing or treating a health problem or disease.

Kathleen Gaines (nee Colduvell) is a nationally published writer turned Pediatric ICU nurse from Philadelphia with over 13 years of ICU experience. She has an extensive ICU background having formerly worked in the CICU and NICU at several major hospitals in the Philadelphia region. After earning her MSN in Education from Loyola University of New Orleans, she currently also teaches for several prominent Universities making sure the next generation is ready for the bedside. As a certified breastfeeding counselor and trauma certified nurse, she is always ready for the next nursing challenge.

Plus, get exclusive access to discounts for nurses, stay informed on the latest nurse news, and learn how to take the next steps in your career.
By clicking “Join Now”, you agree to receive email newsletters and special offers from Nurse.org. You may unsubscribe at any time by using the unsubscribe link, found at the bottom of every email.
Nursing Care Plans (NCP) Ultimate Guide and List

Writing the best nursing care plan requires a step-by-step approach to complete the parts needed for a care plan correctly. This tutorial will walk you through developing a care plan. This guide has the ultimate database and list of nursing care plans (NCP) and nursing diagnosis samples for our student nurses and professional nurses to use—all for free! Care plan components, examples, objectives, and purposes are included with a detailed guide on writing an excellent nursing care plan or a template for your unit.
Table of Contents
Standardized care plans, individualized care plans, purposes of a nursing care plan, three-column format, four-column format, student care plans, step 1: data collection or assessment, step 2: data analysis and organization, step 3: formulating your nursing diagnoses, step 4: setting priorities, short-term and long-term goals, components of goals and desired outcomes, types of nursing interventions, step 7: providing rationale, step 8: evaluation, step 9: putting it on paper, basic nursing and general care plans, surgery and perioperative care plans, cardiac care plans, endocrine and metabolic care plans, gastrointestinal, hematologic and lymphatic, infectious diseases, integumentary, maternal and newborn care plans, mental health and psychiatric, musculoskeletal, neurological, pediatric nursing care plans, reproductive, respiratory, recommended resources, references and sources, what is a nursing care plan.
A nursing care plan (NCP) is a formal process that correctly identifies existing needs and recognizes a client’s potential needs or risks. Care plans provide a way of communication among nurses, their patients, and other healthcare providers to achieve healthcare outcomes. Without the nursing care planning process, the quality and consistency of patient care would be lost.
Nursing care planning begins when the client is admitted to the agency and is continuously updated throughout in response to the client’s changes in condition and evaluation of goal achievement. Planning and delivering individualized or patient-centered care is the basis for excellence in nursing practice .
Types of Nursing Care Plans
Care plans can be informal or formal: An informal nursing care plan is a strategy of action that exists in the nurse ‘s mind. A formal nursing care plan is a written or computerized guide that organizes the client’s care information.
Formal care plans are further subdivided into standardized care plans and individualized care plans: Standardized care plans specify the nursing care for groups of clients with everyday needs. Individualized care plans are tailored to meet a specific client’s unique needs or needs that are not addressed by the standardized care plan.
Standardized care plans are pre-developed guides by the nursing staff and health care agencies to ensure that patients with a particular condition receive consistent care. These care plans are used to ensure that minimally acceptable criteria are met and to promote the efficient use of the nurse’s time by removing the need to develop common activities that are done repeatedly for many of the clients on a nursing unit.
Standardized care plans are not tailored to a patient’s specific needs and goals and can provide a starting point for developing an individualized care plan .
Care plans listed in this guide are standard care plans which can serve as a framework or direction to develop an individualized care plan.
An individualized care plan care plan involves tailoring a standardized care plan to meet the specific needs and goals of the individual client and use approaches shown to be effective for a particular client. This approach allows more personalized and holistic care better suited to the client’s unique needs, strengths, and goals.
Additionally, individualized care plans can improve patient satisfaction . When patients feel that their care is tailored to their specific needs, they are more likely to feel heard and valued, leading to increased satisfaction with their care. This is particularly important in today’s healthcare environment , where patient satisfaction is increasingly used as a quality measure.
Tips on how to individualize a nursing care plan:
- Perform a comprehensive assessment of the patient’s health, history, health status, and desired goals.
- Involve the patient in the care planning process by asking them about their health goals and preferences. By involving the client, nurses can ensure that the care plan is aligned with the patient’s goals and preferences which can improve patient engagement and compliance with the care plan.
- Perform an ongoing assessment and evaluation as the patient’s health and goals can change. Adjust the care plan accordingly.
The following are the goals and objectives of writing a nursing care plan:
- Promote evidence-based nursing care and render pleasant and familiar conditions in hospitals or health centers.
- Support holistic care , which involves the whole person, including physical, psychological, social, and spiritual, with the management and prevention of the disease.
- Establish programs such as care pathways and care bundles. Care pathways involve a team effort to reach a consensus regarding standards of care and expected outcomes. In contrast, care bundles are related to best practices concerning care for a specific disease.
- Identify and distinguish goals and expected outcomes.
- Review communication and documentation of the care plan.
- Measure nursing care.
The following are the purposes and importance of writing a nursing care plan:
- Defines nurse’s role. Care plans help identify nurses’ unique and independent role in attending to clients’ overall health and well-being without relying entirely on a physician’s orders or interventions.
- Provides direction for individualized care of the client. It serves as a roadmap for the care that will be provided to the patient and allows the nurse to think critically in developing interventions directly tailored to the individual.
- Continuity of care. Nurses from different shifts or departments can use the data to render the same quality and type of interventions to care for clients, therefore allowing clients to receive the most benefit from treatment.
- Coordinate care. Ensures that all members of the healthcare team are aware of the patient’s care needs and the actions that need to be taken to meet those needs preventing gaps in care.
- Documentation . It should accurately outline which observations to make, what nursing actions to carry out, and what instructions the client or family members require. If nursing care is not documented correctly in the care plan, there is no evidence the care was provided.
- Serves as a guide for assigning a specific staff to a specific client. There are instances when a client’s care needs to be assigned to staff with particular and precise skills.
- Monitor progress. To help track the patient’s progress and make necessary adjustments to the care plan as the patient’s health status and goals change.
- Serves as a guide for reimbursement. The insurance companies use the medical record to determine what they will pay concerning the hospital care received by the client.
- Defines client’s goals. It benefits nurses and clients by involving them in their treatment and care.
A nursing care plan (NCP) usually includes nursing diagnoses , client problems, expected outcomes, nursing interventions , and rationales . These components are elaborated on below:
- Client health assessment , medical results, and diagnostic reports are the first steps to developing a care plan. In particular, client assessment relates to the following areas and abilities: physical, emotional, sexual, psychosocial, cultural, spiritual/transpersonal, cognitive, functional, age-related, economic, and environmental. Information in this area can be subjective and objective.
- Nursing diagnosis . A nursing diagnosis is a statement that describes the patient’s health issue or concern. It is based on the information gathered about the patient’s health status during the assessment.
- Expected client outcomes. These are specific goals that will be achieved through nursing interventions . These may be long and short-term.
- Nursing interventions . These are specific actions that will be taken to address the nursing diagnosis and achieve expected outcomes . They should be based on best practices and evidence-based guidelines.
- Rationales. These are evidence-based explanations for the nursing interventions specified.
- Evaluation . These includes plans for monitoring and evaluating a patient’s progress and making necessary adjustments to the care plan as the patient’s health status and goals change.
Care Plan Formats
Nursing care plan formats are usually categorized or organized into four columns: (1) nursing diagnoses, (2) desired outcomes and goals, (3) nursing interventions, and (4) evaluation. Some agencies use a three-column plan where goals and evaluation are in the same column. Other agencies have a five-column plan that includes a column for assessment cues.
The three-column plan has a column for nursing diagnosis, outcomes and evaluation, and interventions.

This format includes columns for nursing diagnosis, goals and outcomes, interventions, and evaluation.

Below is a document containing sample templates for the different nursing care plan formats. Please feel free to edit, modify, and share the template.
Download: Printable Nursing Care Plan Templates and Formats
Student care plans are more lengthy and detailed than care plans used by working nurses because they serve as a learning activity for the student nurse.

Care plans by student nurses are usually required to be handwritten and have an additional column for “Rationale” or “Scientific Explanation” after the nursing interventions column. Rationales are scientific principles that explain the reasons for selecting a particular nursing intervention.
Writing a Nursing Care Plan
How do you write a nursing care plan (NCP)? Just follow the steps below to develop a care plan for your client.
The first step in writing a nursing care plan is to create a client database using assessment techniques and data collection methods ( physical assessment , health history , interview, medical records review, and diagnostic studies). A client database includes all the health information gathered . In this step, the nurse can identify the related or risk factors and defining characteristics that can be used to formulate a nursing diagnosis. Some agencies or nursing schools have specific assessment formats you can use.
Critical thinking is key in patient assessment, integrating knowledge across sciences and professional guidelines to inform evaluations. This process, crucial for complex clinical decision-making , aims to identify patients’ healthcare needs effectively, leveraging a supportive environment and reliable information
Now that you have information about the client’s health, analyze, cluster, and organize the data to formulate your nursing diagnosis, priorities, and desired outcomes.
Nursing diagnoses are a uniform way of identifying, focusing on and dealing with specific client needs and responses to actual and high-risk problems. Actual or potential health problems that can be prevented or resolved by independent nursing intervention are termed nursing diagnoses.
We’ve detailed the steps on how to formulate your nursing diagnoses in this guide: Nursing Diagnosis (NDx): Complete Guide and List .
Setting priorities involves establishing a preferential sequence for addressing nursing diagnoses and interventions. In this step, the nurse and the client begin planning which of the identified problems requires attention first. Diagnoses can be ranked and grouped as having a high, medium, or low priority. Life-threatening problems should be given high priority.
A nursing diagnosis encompasses Maslow’s Hierarchy of Needs and helps to prioritize and plan care based on patient-centered outcomes. In 1943, Abraham Maslow developed a hierarchy based on basic fundamental needs innate to all individuals. Basic physiological needs/goals must be met before higher needs/goals can be achieved, such as self-esteem and self-actualization. Physiological and safety needs are the basis for implementing nursing care and interventions. Thus, they are at the base of Maslow’s pyramid, laying the foundation for physical and emotional health.
Maslow’s Hierarchy of Needs
- Basic Physiological Needs: Nutrition (water and food), elimination (Toileting), airway (suction)-breathing (oxygen)-circulation (pulse, cardiac monitor, blood pressure ) (ABCs), sleep , sex, shelter, and exercise.
- Safety and Security: Injury prevention ( side rails , call lights, hand hygiene , isolation , suicide precautions, fall precautions, car seats, helmets, seat belts), fostering a climate of trust and safety ( therapeutic relationship ), patient education (modifiable risk factors for stroke , heart disease).
- Love and Belonging: Foster supportive relationships, methods to avoid social isolation ( bullying ), employ active listening techniques, therapeutic communication , and sexual intimacy.
- Self-Esteem: Acceptance in the community, workforce, personal achievement, sense of control or empowerment, accepting one’s physical appearance or body habitus.
- Self-Actualization: Empowering environment, spiritual growth, ability to recognize the point of view of others, reaching one’s maximum potential.

The client’s health values and beliefs, priorities, resources available, and urgency are factors the nurse must consider when assigning priorities. Involve the client in the process to enhance cooperation.
Step 5: Establishing Client Goals and Desired Outcomes
After assigning priorities for your nursing diagnosis, the nurse and the client set goals for each determined priority. Goals or desired outcomes describe what the nurse hopes to achieve by implementing the nursing interventions derived from the client’s nursing diagnoses. Goals provide direction for planning interventions, serve as criteria for evaluating client progress, enable the client and nurse to determine which problems have been resolved, and help motivate the client and nurse by providing a sense of achievement.

One overall goal is determined for each nursing diagnosis. The terms “ goal outcomes “ and “expected outcome s” are often used interchangeably.
According to Hamilton and Price (2013), goals should be SMART . SMART stands for specific, measurable, attainable, realistic, and time-oriented goals.
- Specific. It should be clear, significant, and sensible for a goal to be effective.
- Measurable or Meaningful. Making sure a goal is measurable makes it easier to monitor progress and know when it reaches the desired result.
- Attainable or Action-Oriented. Goals should be flexible but remain possible.
- Realistic or Results-Oriented. This is important to look forward to effective and successful outcomes by keeping in mind the available resources at hand.
- Timely or Time-Oriented. Every goal needs a designated time parameter, a deadline to focus on, and something to work toward.
Hogston (2011) suggests using the REEPIG standards to ensure that care is of the highest standards. By this means, nursing care plans should be:
- Realistic. Given available resources.
- Explicitly stated. Be clear about precisely what must be done, so there is no room for misinterpretation of instructions.
- Evidence-based. That there is research that supports what is being proposed.
- Prioritized. The most urgent problems are being dealt with first.
- Involve. Involve both the patient and other members of the multidisciplinary team who are going to be involved in implementing the care.
- Goal-centered. That the care planned will meet and achieve the goal set.
Goals and expected outcomes must be measurable and client-centered. Goals are constructed by focusing on problem prevention, resolution, and rehabilitation. Goals can be short-term or long-term . Most goals are short-term in an acute care setting since much of the nurse’s time is spent on the client’s immediate needs. Long-term goals are often used for clients who have chronic health problems or live at home, in nursing homes, or in extended-care facilities.
- Short-term goal . A statement distinguishing a shift in behavior that can be completed immediately, usually within a few hours or days.
- Long-term goal . Indicates an objective to be completed over a longer period, usually weeks or months.
- Discharge planning . Involves naming long-term goals, therefore promoting continued restorative care and problem resolution through home health, physical therapy, or various other referral sources.
Goals or desired outcome statements usually have four components: a subject, a verb, conditions or modifiers, and a criterion of desired performance.

- Subject. The subject is the client, any part of the client, or some attribute of the client (i.e., pulse, temperature, urinary output). That subject is often omitted in writing goals because it is assumed that the subject is the client unless indicated otherwise (family, significant other ).
- Verb. The verb specifies an action the client is to perform, for example, what the client is to do, learn, or experience.
- Conditions or modifiers. These are the “what, when, where, or how” that are added to the verb to explain the circumstances under which the behavior is to be performed.
- Criterion of desired performance. The criterion indicates the standard by which a performance is evaluated or the level at which the client will perform the specified behavior. These are optional.
When writing goals and desired outcomes, the nurse should follow these tips:
- Write goals and outcomes in terms of client responses and not as activities of the nurse. Begin each goal with “Client will […]” help focus the goal on client behavior and responses.
- Avoid writing goals on what the nurse hopes to accomplish, and focus on what the client will do.
- Use observable, measurable terms for outcomes. Avoid using vague words that require interpretation or judgment of the observer.
- Desired outcomes should be realistic for the client’s resources, capabilities, limitations, and on the designated time span of care.
- Ensure that goals are compatible with the therapies of other professionals.
- Ensure that each goal is derived from only one nursing diagnosis. Keeping it this way facilitates evaluation of care by ensuring that planned nursing interventions are clearly related to the diagnosis set.
- Lastly, make sure that the client considers the goals important and values them to ensure cooperation.
Step 6: Selecting Nursing Interventions
Nursing interventions are activities or actions that a nurse performs to achieve client goals. Interventions chosen should focus on eliminating or reducing the etiology of the priority nursing problem or diagnosis. As for risk nursing problems, interventions should focus on reducing the client’s risk factors. In this step, nursing interventions are identified and written during the planning step of the nursing process ; however, they are actually performed during the implementation step.
Nursing interventions can be independent, dependent, or collaborative:

- Independent nursing interventions are activities that nurses are licensed to initiate based on their sound judgement and skills. Includes: ongoing assessment, emotional support, providing comfort , teaching, physical care, and making referrals to other health care professionals.
- Dependent nursing interventions are activities carried out under the physician’s orders or supervision. Includes orders to direct the nurse to provide medications, intravenous therapy , diagnostic tests, treatments, diet, and activity or rest. Assessment and providing explanation while administering medical orders are also part of the dependent nursing interventions.
- Collaborative interventions are actions that the nurse carries out in collaboration with other health team members, such as physicians, social workers, dietitians, and therapists. These actions are developed in consultation with other health care professionals to gain their professional viewpoint.
Nursing interventions should be:
- Safe and appropriate for the client’s age, health, and condition.
- Achievable with the resources and time available.
- Inline with the client’s values, culture, and beliefs.
- Inline with other therapies.
- Based on nursing knowledge and experience or knowledge from relevant sciences.
When writing nursing interventions, follow these tips:
- Write the date and sign the plan. The date the plan is written is essential for evaluation, review, and future planning. The nurse’s signature demonstrates accountability.
- Nursing interventions should be specific and clearly stated, beginning with an action verb indicating what the nurse is expected to do. Action verb starts the intervention and must be precise. Qualifiers of how, when, where, time, frequency, and amount provide the content of the planned activity. For example: “ Educate parents on how to take temperature and notify of any changes,” or “ Assess urine for color, amount, odor, and turbidity.”
- Use only abbreviations accepted by the institution.
Rationales, also known as scientific explanations, explain why the nursing intervention was chosen for the NCP.

Rationales do not appear in regular care plans. They are included to assist nursing students in associating the pathophysiological and psychological principles with the selected nursing intervention.
Evaluation is a planned, ongoing, purposeful activity in which the client’s progress towards achieving goals or desired outcomes is assessed, and the effectiveness of the nursing care plan (NCP). Evaluation is an essential aspect of the nursing process because the conclusions drawn from this step determine whether the nursing intervention should be terminated, continued, or changed.
The client’s care plan is documented according to hospital policy and becomes part of the client’s permanent medical record, which may be reviewed by the oncoming nurse. Different nursing programs have different care plan formats. Most are designed so that the student systematically proceeds through the interrelated steps of the nursing process , and many use a five-column format.
Nursing Care Plan List
This section lists the sample nursing care plans (NCP) and nursing diagnoses for various diseases and health conditions. They are segmented into categories:
Miscellaneous nursing care plans examples that don’t fit other categories:
Care plans that involve surgical intervention .
| Surgery and Perioperative Care Plans |
|---|
Nursing care plans about the different diseases of the cardiovascular system :
| Cardiac Care Plans |
|---|
Nursing care plans (NCP) related to the endocrine system and metabolism:
| Endocrine and Metabolic Care Plans |
|---|
| Acid-Base Imbalances |
|---|
| Electrolyte Imbalances |
|---|
Care plans (NCP) covering the disorders of the gastrointestinal and digestive system :
| Gastrointestinal Care Plans |
|---|
Care plans related to the hematologic and lymphatic system:
| Hematologic & Lymphatic Care Plans |
|---|
NCPs for communicable and infectious diseases:
| Infectious Diseases Care Plans |
|---|
All about disorders and conditions affecting the integumentary system:
| Integumentary Care Plans |
|---|
Nursing care plans about the care of the pregnant mother and her infant. See care plans for maternity and obstetric nursing:
| Maternal and Plans |
|---|
Care plans for mental health and psychiatric nursing:
| Mental Health and Psychiatric Care Plans |
|---|
Care plans related to the musculoskeletal system:
| Musculoskeletal Care Plans |
|---|
Nursing care plans (NCP) for related to nervous system disorders:
| Neurological Care Plans |
|---|
Care plans relating to eye disorders:
| Care Plans |
|---|
Nursing care plans (NCP) for pediatric conditions and diseases:
| Pediatric Nursing Care Plans |
|---|
Care plans related to the reproductive and sexual function disorders:
| Reproductive Care Plans |
|---|
Care plans for respiratory system disorders:
| Respiratory Care Plans |
|---|
Care plans related to the kidney and urinary system disorders:
| Urinary Care Plans |
|---|
Recommended nursing diagnosis and nursing care plan books and resources.
Disclosure: Included below are affiliate links from Amazon at no additional cost from you. We may earn a small commission from your purchase. For more information, check out our privacy policy .
Ackley and Ladwig’s Nursing Diagnosis Handbook: An Evidence-Based Guide to Planning Care We love this book because of its evidence-based approach to nursing interventions. This care plan handbook uses an easy, three-step system to guide you through client assessment, nursing diagnosis, and care planning. Includes step-by-step instructions showing how to implement care and evaluate outcomes, and help you build skills in diagnostic reasoning and critical thinking.

Nursing Care Plans – Nursing Diagnosis & Intervention (10th Edition) Includes over two hundred care plans that reflect the most recent evidence-based guidelines. New to this edition are ICNP diagnoses, care plans on LGBTQ health issues, and on electrolytes and acid-base balance.

Nurse’s Pocket Guide: Diagnoses, Prioritized Interventions, and Rationales Quick-reference tool includes all you need to identify the correct diagnoses for efficient patient care planning. The sixteenth edition includes the most recent nursing diagnoses and interventions and an alphabetized listing of nursing diagnoses covering more than 400 disorders.

Nursing Diagnosis Manual: Planning, Individualizing, and Documenting Client Care Identify interventions to plan, individualize, and document care for more than 800 diseases and disorders. Only in the Nursing Diagnosis Manual will you find for each diagnosis subjectively and objectively – sample clinical applications, prioritized action/interventions with rationales – a documentation section, and much more!

All-in-One Nursing Care Planning Resource – E-Book: Medical-Surgical, Pediatric, Maternity, and Psychiatric-Mental Health Includes over 100 care plans for medical-surgical, maternity/OB, pediatrics, and psychiatric and mental health. Interprofessional “patient problems” focus familiarizes you with how to speak to patients.

Recommended reading materials and sources for this NCP guide:
- Björvell, C., Thorell-Ekstrand, I., & Wredling, R. (2000). Development of an audit instrument for nursing care plans in the patient record. BMJ Quality & Safety , 9 (1), 6-13. [ Link ]
- DeLaune, S. C., & Ladner, P. K. (2011). Fundamentals of nursing: Standards and practice . Cengage learning .
- Freitas, F. A., & Leonard, L. J. (2011). Maslow’s hierarchy of needs and student academic success . Teaching and learning in Nursing , 6 (1), 9-13.
- Hamilton, P., & Price, T. (2007). The nursing process, holistic. Foundations of Nursing Practice E-Book: Fundamentals of Holistic Care , 349.
- Lee, T. T. (2004). Evaluation of computerized nursing care plan: instrument development . Journal of Professional Nursing , 20 (4), 230-238.
- Lee, T. T. (2006). Nurses’ perceptions of their documentation experiences in a computerized nursing care planning system . Journal of Clinical Nursing , 15 (11), 1376-1382.
- Rn , B. O. C., Rn, H. M., Rn, D. T., & Rn, F. E. (2000). Documenting and communicating patient care : Are nursing care plans redundant?. International Journal of Nursing Practice , 6 (5), 276-280.
- Stonehouse, D. (2017). Understanding the nursing process . British Journal of Healthcare Assistants , 11 (8), 388-391.
- Yildirim, B., & Ozkahraman, S. (2011). Critical thinking in nursing process and education . International journal of humanities and social science , 1 (13), 257-262.
69 thoughts on “Nursing Care Plans (NCP) Ultimate Guide and List”
This page is helpful!
Thank you! Hope we’ve helped you write better nursing care plans!
Will definitely use this site to help write care plans. How should I cite this link when using APA format. Thank You
HI Can some one help me to do assignment on Impaired renal perfusion. 1.Goal 2.Related Action 3.Rational 4.Evaluate outcome
Wow God bless plenty Nurseslabs really relieve my burdens 😊😊
Thank you for all this useful info! I have been looking for something like this online.
You’re welcome! :)
Quite educative thank you
The notes were indeed useful
I hope to learn more and improve my skills towards nursing
Thank you so so much! This website is of great assistance to me. God bless you.
It’s so great for nursing student
Very beautiful ,Good work keep it up
Nice work. Well done
Very helpful
Great job,thank you
Thanks so much , it’s of much support for students .
Risk for ineffective thermoregulation would be a good one for you to do next for newborn.
Hi, i have learnt a lot THANK YOU. i would kindly like to learn more on paper 1 since am yet to sit for my nursing council exams and feel challenged on the paper.please do assist me thank you.
This site is a total lifesaver!
What is a nursing care plan a mother in second stage of labour?
Please see: 36 Labor Stages, Induced and Augmented Labor Nursing Care Plans
What is the nursing care plan for pulmonary oedema?
I m interest in receiving a blank nursing care plan template for my students to type on. I was wondering if it was available and if so can you please direct me on where to find it?
Hi! You can download it here: Nursing Care Plan Template
I love this website!!! Is there a textbook version of the Nurseslabs that I can purchase??
Thank you Nurseslabs. This is a wonderful note you’ve prepared for all nurses. I would like a pdf of this. Thanks.
I wish I had had this resource when i was in nursing school 2008!!
Yeah! It’s nice
Thanks for this information!
God bless you sis…Thank you for all this useful info!
This is the kind of step-by-step guidance that I needed. Thank you!
Thank you. I have learned a lot!
Wow! This is a hidden treasure!
Thanks a lot for this, it is really helpful!
Hi Matt! I would like to purchase a textbook of your nursing care plan. Where I can purchase pls help!
Hi Criselda,
Sorry, we don’t have a textbook. All of our resources are here on the website and free to use.
Good day, I would like to know how can I use your website to help students with care plans.
Sincerely, Oscar A. Acosta DNP, RN
Oh I love your works. Your explanations
I’m glad I’ve met your website. It helps me a lot. Thank you
I love this, so helpful.
These care plans are great for using as a template. I don’t have to reinvent the wheel, and the information you provided will ensure that I include the important data without leaving things out. Thanks a million!
Hi, I have learnt a lot, this is a wonderful note you’ve prepared for all nurses thank you.
Matt, this page is very informative and I especially appreciate seeing care plans for patients with neurological disorders. I notice, though, that traumatic brain injury is not on your list. Might you add a care plan page for this?
Thanks alot I had gained much since these are detailed notes 🙏🙏
OMG, this is amazing!
Wow very helpful.thank you very much🙏🙏
Hi, is there a downloadable version of this, pdf or other files maybe this is awesome!
Hi Paul, on your browser go to File > Print > Save as PDF. Hope that helps and thanks for visiting Nurseslabs!
Matt, I’m a nursing instructor looking for tools to teach this. I am interested in where we can find “rules” for establishing “related to” sections…for example –not able to utilize medical diagnosis as a “related to” etc. Also, resources for nursing rationale.
Hello, please check out our guide on how to write nursing diagnoses here: https://nurseslabs.com/nursing-diagnosis/
Nursing care plan is very amazing
Thanks for your time. Nursing Care Plan looks great and helpful!
complete knowledge i get from here
great resource. puts it all together. Thank for making it free for all
Hello Ujunwa, Thanks a lot for the positive vibes! 🌟 It’s super important to us that everyone has access to quality resources. Just wondering, is there any specific topic or area you’d love to see more about? We’re always looking to improve and add value!
Great work.
Hi Abbas, Thank you so much! Really glad to hear you found the nursing care plans guide useful. If there’s a specific area or topic you’re keen on exploring more, or if you have any suggestions for improvement, feel free to share. Always aiming to make our resources as helpful as possible!
It has been good time me to use these nursing guides.
What is ncp for acute pain
For everything you need to know about managing acute pain, including a detailed nursing care plan (NCP), definitely check out our acute pain nursing care plan guide . It’s packed with insights on assessment, interventions, and patient education to effectively manage and alleviate acute pain.
Good morning. I love this website
what is working knowledge on nursing standard, and Basic Life Support documentation?
Thank you for the website, it is awesome. I just have one question about the 1st set of ABG (Practice Exam) – The following are the values: pH 7.3, PaCO2 68 mm Hg, HCO3 28 mmol/L, and PaO2 60 mm Hg…Definitely Respiratory Acidosis, but the HC03 is only 28 mmol/L..I thought HC03 of 28 mmol/L would be within the normal range and thus, no compensation, but the correct answer has partial compensation because of the HC03 value. What value ranges are you using for HC03. Thanks, EK Mickley, RN BSN
welcome to you can get the best way to days after the holiest month
Intra operative care ncp
Leave a Comment Cancel reply

- Subscribe to journal Subscribe
- Get new issue alerts Get alerts
Secondary Logo
Journal logo.
Colleague's E-mail is Invalid
Your message has been successfully sent to your colleague.
Save my selection
Caring for patients with burn injuries
Culleiton, Alicia L. DNP, RN, CNE; Simko, Lynn M. PhD, RN, CCRN
At Duquesne University's School of Nursing in Pittsburgh, Pa., Alicia L. Culleiton is an assistant clinical professor and Lynn M. Simko is an associate clinical professor.
The authors and planners have disclosed that they have no financial relationships related to this article.
Patients with severe burns require prompt and appropriate nursing care to minimize the risk of death or disability. This article reviews types of burns and discusses how to provide initial resuscitative care for a patient who can't be immediately transferred to a designated burn center or burn ICU.

BURN INCIDENCE has decreased slightly over the years, but burn injuries still occur all too often, with an estimated 3,400 fire and burn deaths each year (this figure includes deaths from smoke inhalation and toxicity). 1 This article reviews types of burns and discusses how to provide initial resuscitative care for a patient who can't be immediately transferred for treatment in a designated burn center or burn ICU.
About 45,000 patients who sustain burn injuries require medical treatment or hospitalization yearly. According to the American Burn Association (ABA), hospital admission based on the type of burn breaks down as follows:
- fire or burn injury, 44%
- scald injury, 33%
- injury from contact with hot objects, 9%
- electrical burns, 4%
- chemical burns, 3%
- miscellaneous causes, 7%. 1
Burn injuries are among the most expensive catastrophic injuries to treat. For instance, a burn injury of 30% of total body surface area (TBSA) can cost as much as $200,000 in initial hospitalization costs; in addition, significant costs related to reconstructive surgery and rehabilitation are associated with more extensive burns. 2 Mortality is higher for children younger than age 4 (especially from birth to age 1), and for adults over age 65. 3
Breaching a protective barrier
One of the largest organs of the body, the skin has many functions. Besides providing a protective barrier against physical injury and microorganisms, it's crucial for thermoregulatory control, prevention of fluid loss, synthesis of vitamin D, and sensory contact with the environment.
The skin has two layers: an outer epidermis and an inner dermis, separated by a basement membrane. (See Skin layers and structures .) Burn injuries involving the partial or complete destruction of the skin and its appendages (hair follicles, nails, and sweat glands) cause local and systemic disturbances, such as compromised immunity, hypothermia, severe fluid loss, infection, and changes in appearance, function, and body image.

A burn injury is described based on its cause: thermal, chemical, electrical, radiation, smoke or inhalation, or frostbite.
- Thermal burns result from contact with hot substances, including flame, hot liquids, hot solid objects, and steam, that cause cell injury by coagulative necrosis. 4 The longer the skin is in contact with these hot substances, the deeper the wound. Because oil-based liquids such as grease and cooking oil have higher boiling points, they cause deeper burns than scalds with water or other liquids. 5 Burns from hot solid objects such as solid metal, hot plastic, glass, or stone are all considered thermal burns.
- Chemical burns destroy tissue and continue to do damage for up to 72 hours unless neutralized. Causes of chemical burns are strong acids, alkalis, and organic compounds. Acids , common in household cleaners such as rust removers and bathroom cleaners, cause protein coagulation, which results in less extensive injuries. Alkalis such as oven cleaners and fertilizers cause deeper burns due to liquefactive necrosis, which lets the chemical penetrate deeper into tissues. Organic compounds that cause chemical burns include gasoline and chemical disinfectants, which can cause severe coagulative necrosis and produce a layer of thick, nonviable tissue called eschar, which is normally present in full-thickness burns. 6
- Electrical burns are classified as low voltage (under 1,000 V) or high voltage (1,000 V or higher). 6 Electrical injuries can cause death by triggering ventricular fibrillation or paralyzing respiratory muscles. Although dysrhythmias can be triggered by low-voltage injuries, they're more common in high-voltage injuries.
The extent of damage from an electrical burn may initially appear minor—the patient may have only small entry and exit wounds. Extensive damage can appear within several days to weeks—a phenomenon known as the iceberg effect because the skin shows little injury on the surface and hides massive injury beneath. 6
Instead of conducting the electricity, bones, muscle, tendon, and fat respond to electrical injury by producing heat. Most injuries occur to muscles surrounding the long bones. 6
- Radiation burns can result from exposure to radiofrequency energy or ionizing radiation such as sunlight, tanning booths, X-rays, or nuclear emissions or explosions. Ionizing radiation can produce tissue damage directly by striking a vital molecule such as DNA. 5 Sunburn usually causes a first-degree or superficial burn, but radiation therapy can cause full-thickness burns.
- Smoke and inhalation burns can occur concurrently with thermal or chemical burns. If the patient has thermal burns, look for signs of inhalation burns: facial burns, hoarseness, soot in the nose or mouth, carbon in the sputum, lip edema, and singed eyebrows or nasal hair. Manufacturing illegal methamphetamine can cause thermal and chemical burns and associated inhalation burns. 6 Regardless of the cause of the inhalation injury, the patient needs immediate interventions such as endotracheal intubation, bronchoscopy, and measurement of carboxyhemoglobin (COHb) levels.
- Frostbite is temporary or permanent tissue damage resulting from exposure to very cold temperatures. Any area of the body left uncovered in very cold temperatures can become frostbitten, but the most commonly affected areas are the fingers, toes, chin, earlobes, cheeks, and nose. 7 Without treatment, frostbite can progress to cellular necrosis, gangrene, hypothermia, and cardiac arrest. Because frostbite damages the skin, some patients are treated in the ICU as burn patients, although initial treatment for frostbite is different than that for other burns.

Depth of injury
Burns are also categorized according to the depth of injury. In the past, burn injuries were classified as first, second, third, and occasionally fourth degree. In recent years, the ABA has recommended a more precise classification of burns, categorizing them according to depth of tissue injury:
- epidermal or superficial (first degree)
- partial-thickness (second degree), which may also be classified as superficial or deep partial-thickness
- full-thickness (third degree), which may also be classified as deep full-thickness (fourth degree). 8
For details, see Classifying burn injuries .

Size matters
The size of the burn is expressed as the percentage of TBSA. A partial-thickness burn of more than 10% TBSA is serious and requires referral to a burn center. (See Should the patient go to a burn center? )
Estimate the TBSA burned on an adult by using 9 or multiples of 9, known as the rule of nines. The rule of nines varies between infants and adults because infants' heads are proportionally larger compared to adults. (See Rule of nines: Estimating burn size in adults .) Although the rule of nines provides a rapid method for calculating the size of the burn injury, it can lead to an overestimation of the TBSA burned, so follow facility protocol for estimating the extent of a burn injury. Most burn centers repeat the estimation of TBSA burned in 72 hours, when burns and their depth are more clearly demarcated and the burned area can be more easily quantified. 9
Other common methods for measuring burn size include the Lund-Browder chart and the palm method.
- The Lund-Browder method is highly recommended because it corrects for the large head-to-body ratio of infants and children. 10
- The palm method is used for small scattered burns such as grease and scald burns. Often, the rule of palms will be completed first as a quick assessment until the Lund and Browder assessment can be completed. The patient's palm (not including the fingers or wrist) equals 0.5% of TBSA. The entire palm including the fingers equals 1% in children and adults. 4
Location matters too
Depending on a burn injury's location, the patient may be predisposed to initial complications or complications during wound healing. 11 Circumferential burns of the extremities, for example, can lead to vascular compromise resulting in compartment syndrome (see Ring of fire ). Circumferential burns to the thorax can impair chest wall expansion, causing pulmonary insufficiency. Burns of the chest, head, and neck are also associated with pulmonary complications.
Facial burns are associated with corneal abrasions and burns of the ears with auricular chondritis. Burns of the perineal area are prone to autocontamination by urine and feces. 11,12
Burns over joints immediately affect the patient's range of motion, which may be exacerbated later by hypertrophic scarring (see Troublesome scars ). Intensive therapy to prevent permanent disability is crucial.
Taking an inside look
Understanding the pathophysiology of a major burn injury (sometimes called burn shock) is key to effective management. Different causes lead to different burn injury patterns, which require different management.
The body's compensatory mechanisms start with the inflammatory response, which is initiated by cellular injury. The most important activator of the inflammatory response is the mast cell, which releases biochemical mediators, such as histamine and chemotactic factors, and synthesizes other mediators, such as prostaglandins and leukotrienes. 13 Histamine, the major vasoactive amine released by the mast cells, increases capillary permeability and exudation, resulting in edema at the burn injury site, decreased intravascular volume, hypotension, tachypnea, tachycardia, oliguria, and shock. 13
The sympathetic nervous system (SNS) is stimulated and the fight-or-flight response activated, causing thirst, gastrointestinal hypomotility (ileus), adrenal gland stimulation (causing increased circulating catecholamines, increased metabolic rate, and increased aldosterone secretion), hepatic stimulation (causing release of glycogen stores and elevated blood glucose levels), and vasoconstriction. 13

A major burn injury affects every body system.
- Respiratory system effects include direct airway injury; inhalation injury; carbon monoxide poisoning; smoke inhalation (damage to epithelial cells in the lower respiratory tract secondary to inhaling oxides, the products of combustion); alveolar damage; pulmonary edema; and decreased oxygen diffusion. 5
- Cardiovascular system effects include fluid volume deficit, decreased mean arterial pressure, decreased cardiac output, hypovolemic shock (secondary to extensive fluid shifts), and decreased myocardial contractility (impaired cardiac function improves 24 to 30 hours postinjury). Electrical burns can cause ECG changes, myocardial infarction, and cardiac dysrhythmias including ventricular fibrillation. 6
- R e nal system effects are indirect. Decreased cardiac output leads to decreased renal perfusion and oliguria that can culminate in acute kidney injury (AKI). In addition, after a burn injury, damaged red blood cells release hemoglobin and potassium, and skeletal muscle cells release myoglobin. Both hemoglobin and myoglobin are filtered by the glomerulus and degraded, releasing heme pigment. Heme pigment, especially in the setting of fluid volume deficit, can cause AKI. 14 Marked release of hemoglobin or myoglobin usually causes red or brown urine.
- Gastrointestinal system effects include ileus secondary to SNS activation. Stress ulcer formation is triggered by the stress response and the histamine released in the acute inflammatory response. Intra-abdominal hypertension and abdominal compartment syndrome can damage the gut, kidneys, and liver. 6,9
- Neuroendocrine system effects include increased metabolic rate to compensate for the initial low core body temperature due to loss of skin. The increased metabolic rate increases caloric needs and leads to catabolism and a negative nitrogen balance that slows tissue building and healing. 6 Increased cortisol levels may cause insulin resistance and hyperglycemia. 13
- Immune system effects include immunosuppression secondary to the immediate, prolonged, and severe immunologic and inflammatory response to a major burn injury. 13
- Musculoskeletal system effects include contractures and complications secondary to immobility and scar tissue formation during the healing process.
Initial assessment and management
Emergency management of a patient with a burn injury begins with the initial assessment and treatment of life-threatening injuries. Stabilize the patient's cervical spine if this hasn't already been done. The true mechanism of injury may not be clear (for example, the patient may have been burned and propelled in an explosion).
Follow these specific aspects of the ABCDE (Airway, Breathing, Circulation, Disability, and Exposure/Environmental control) assessment: 6,9,15
- A irway. Maintaining the airway is the primary concern, especially if a patient has an inhalation injury. Assess for stridor (an ominous sign that suggests the patient's upper airway is at least 85% narrowed), facial burns, soot in the nares or mouth, singed facial hair or nasal hair, edema of the lips and oral cavity, coughing, hoarse voice, and circumferential neck burns. 6 , 9
- B reathing. Determine adequacy of ventilation by assessing the patient's respiratory rate and depth and observing for dyspnea. Auscultate the lungs, noting any adventitious breath sounds. Obtain a pulse oximetry reading (remembering that it may be inaccurate in the presence of carbon monoxide), and a co-oximetry reading if indicated and available. 6,9,15
- C irculation. Observe for obvious arterial bleeding. Assess for the presence, symmetry, amplitude, rate, and rhythm of pulses; evaluate capillary refill time, skin color, and temperature. 9
- D isability. Use the AVPU (Alert, Verbal, Pain stimuli, Unresponsive) scale to determine the patient's level of consciousness and carefully evaluate any abnormalities. (See Reading the AVPU scale .) Assess for hypoxia, decreased cerebral perfusion related to hypovolemia, and cerebral injury resulting from head trauma. Assess the patient's pupillary response to light and sensory and motor function. 3,6
- E xposure/environmental control. Gently remove the patient's nonadherent clothing and jewelry to prevent continued tissue damage. If the patient's face is burned, remove glasses or contact lenses. Cover the patient with a dry sterile sheet to prevent further contamination of the burn wounds and to provide warmth. 3,9,10,15
Obtain vital signs and establish I.V. access with two large-bore catheters if the patient has burns over 15% of TBSA. Under ABA practice guidelines, fluid resuscitation is indicated for any patient with nonsuperficial burns covering more than 15% of TBSA. 1,16 Elevate burned extremities above heart level to decrease edema. Administer I.V. analgesia as prescribed and assess its effectiveness often, using a valid and reliable pain intensity rating scale.

Obtaining a history
After the initial focused assessment is completed and the patient is stabilized, obtain a history of the events while performing a comprehensive physical assessment. The main priorities are to determine the potential for an inhalation injury, presence of concomitant injuries or trauma, and any preexisting conditions that may influence the physical assessment or patient outcomes. A simple way to initially accomplish this is to use the SAMPLE mnemonic: S igns and symptoms, A llergies, current M edications (including illegal substances or alcohol), P ertinent history, L ast oral intake, and E vents leading up to the injury. 17
After determining the extent and depth of the burn, ask the following questions:
- What's the patient's chief complaint (for example, dyspnea or pain)?
- Did the burn occur in an enclosed space?
- Were explosives or chemicals involved?
- What was the source of the burning agent (for example, liquid, metal, or chemicals)?
- What's the status of the patient's tetanus immunization? 10
Stages of burn management
Care for a patient with burn injuries is organized into three stages: emergent (resuscitative), acute (wound healing), and rehabilitative (restorative). 9 The assessment and management of specific problems overlap and may span two or three stages. For example, rehabilitation begins on the first day after the burn injury, although the formal rehabilitative phase begins when the burn wound is almost healed. 15
About fluid resuscitation
Fluid resuscitation efforts are started as soon as possible for patients with burns covering more than 15% of TBSA; otherwise, the patient may experience hypovolemic shock. 6 Insert an indwelling urinary catheter to closely monitor urinary output. Fluid resuscitation is usually accomplished with an isotonic crystalloid such as lactated Ringer's solution; the lactate helps to buffer the metabolic acidosis commonly seen with hypoperfusion and burn shock. 6 Several fluid resuscitation formulas are available (for example, the Parkland formula) and usually is prescribed by the burn trauma surgeon. All formulas are based on the percentage of TBSA burned, the patient's weight in kilograms (kg), and the patient's age.
Half of the prescribed fluid volume is administered in the first 8 hours postburn, and the remainder is given over the next 16 hours. The ABA recommends titrating the fluids to maintain a urine output of 30 to 50 mL/hour in adults and 1 mL/kg/hour in children weighing less than 30 kg (66.1 lb). 6 (The adult guideline is used for children weighing 30 kg or more.) In the case of a patient who's sustained a high-voltage electrical burn, the target range for urine output is 75 to 100 mL/hour to prevent renal tubular obstruction from heme pigment. 6 Monitor the patient's mental status, vital signs, hourly urine output, and urine specific gravity; these are valuable indicators of the patient's response to fluid resuscitation.
Because of the massive volumes of I.V. fluids administered to patients with burns (rates of 1,000 mL/hour are common), closely monitor the patient's hemodynamic status to prevent fluid overload. Signs and symptoms of “fluid creep,” or fluid resuscitation in excess of that predicted by the Parkland formula, include abdominal compartment syndrome, extremity compartment syndrome, and acute respiratory distress syndrome. 18,19
Fluid resuscitation after the first 24 hours is accomplished with isotonic crystalloids as well as colloids. Dextrose solutions and electrolyte replacement (especially potassium replacement) is initiated. Lactated Ringer's solution is isotonic and doesn't increase intravascular oncotic pressure. Because of increased capillary permeability in patients with burns, only 25% of the lactated Ringer's solution infused in the initial fluid resuscitation will actually stay in the intravascular space. This is one reason for the large fluid volumes needed in fluid replacement. 6
Once capillary permeability has decreased (8 to 12 hours after the burn injury), colloids such as albumin may be given to help restore intravascular volume. By increasing oncotic pressure in the vascular space, colloids pull interstitial fluid into blood vessels. This also helps decrease the edema associated with burn injuries.
Interventions for specific burn types
For all patients, monitor level of consciousness, respiratory status, cardiac rate and rhythm, vital signs, and oxygen saturation. Identify and treat associated injuries, such as head injury, pneumothorax, or fractures. In addition, initiate specific interventions for these common burn types.
- Thermal . Assess the patient for inhalation injuries. For adults with burns of more than 15% of TBSA, begin fluid replacement as prescribed and insert an indwelling urinary catheter.
- Chemical . Assess the patient's ABCs before starting decontamination procedures. Patients with significant inhalation injuries or circumferential full-thickness burns to the neck or chest may need endotracheal intubation and mechanical ventilation. Remove dry chemicals from the patient's skin, then use saline or tap water to flush chemicals from the burn. Protect yourself and others from exposure and contact the poison control center for more information about the chemical involved. 9,15
- Electrical . Closely monitor pulses distal to the burn. Because many electrical injuries affect the extremities, depending on where the current entered and exited, patients must be watched for development of compartment syndrome. 6
Also monitor for myoglobinemia (myoglobin released from injured muscle tissue and hemoglobin from damaged red blood cells). To prevent renal failure from renal tubular obstruction, large amounts of fluid are needed to maintain urine output at 100 ml/hour. Be prepared to administer I.V. mannitol, an osmotic diuretic, to maintain urine output, and I.V. sodium bicarbonate to alkalinize the urine. 6,9,15
Because the patient is at high risk for dysrhythmias, initiate continuous cardiac monitoring. Cervical collars and backboards should be used and kept in place until X-rays rule out spinal injury—many electrical injuries occur from contact with high voltage wires, causing a fall. 6
- Inhalation . Obtain an arterial blood gas analysis, COHb level, and chest X-ray. Prepare the patient for fiberoptic bronchoscopy or endotracheal intubation if indicated.
Effective interventions
By understanding the types of burns and how to assess and manage them, nurses can immediately implement effective interventions while arrangements are made for patient transfer to a burn specialty center.
Should the patient go to a burn center? 21
Patients with burn injuries who should be referred to a burn center include:
- All patients under age 1.
- All patients ages 1 to 2 with burns over 5% or more of TBSA.
- Patients of any age with full-thickness burns of any size.
- Patients over age 2 with partial-thickness burns greater than 10% of TBSA.
- Patients with burns of special areas such as the face, hands, feet, genitalia, perineum, or major joints.
- Patients with electrical burns, including lightning injuries.
- Patients with chemical burns.
- Patients with inhalation injury resulting from a fire or hot liquid burn.
- Patients with circumferential burns of the limbs or chest.
- Patients with preexisting medical conditions that could complicate burn management, prolong recovery, or affect survival.
- Patients with burns and concomitant trauma.
- Children with burns who are suspected to be victims of child abuse.
- Patients with septic burn wounds.
- Patients whose burns require treatment that exceeds the capabilities of the referring facility.
Reading the AVPU scale
The AVPU scale can be used to determine a patient's level of consciousness.
Alert: Patient is alert, awake, responds to voice, and is oriented to time, place, and person.
Verbal: The patient opens his or her eyes to verbal stimuli, but isn't fully oriented to time, place, or person.
Painful: The patient responds to painful or noxious stimuli, such as nail bed pressure or a sternal rub, but doesn't respond to verbal stimuli.
Unresponsive: The patient is nonverbal and doesn't respond to painful stimuli.
Source: http://www.ahrq.gov/research/esi/esi2.htm .
- + Favorites
- View in Gallery
Readers Of this Article Also Read
Early warning systems: the next level of rapid response, dealing with hypertensive emergency and urgency: your patient's blood pressure..., drawing blood through a central venous catheter, making referrals.
Nursing Care of the Burn Patient
- First Online: 22 December 2020
Cite this chapter

- Judy Knighton 4
1371 Accesses
1 Citations
Nursing the burn-injured patient and supporting his/her family throughout recovery is a complex and demanding but, ultimately rewarding, professional role. The repertoire of required nursing skills is varied and includes comprehensive critical care, complex wound care, pain and anxiety management, psychosocial support and community re-integration. Nurses are a consistent presence and can positively impact all phases of a patient’s care. Burn nursing care continues to be driven by evidence-based practices and improved upon by both quantitative and qualitative nursing research. This book chapter is intended to assist the nurse in providing comprehensive, evidence-based care to the burn patient and his/her family.
This is a preview of subscription content, log in via an institution to check access.
Access this chapter
Subscribe and save.
- Get 10 units per month
- Download Article/Chapter or eBook
- 1 Unit = 1 Article or 1 Chapter
- Cancel anytime
- Available as PDF
- Read on any device
- Instant download
- Own it forever
- Available as EPUB and PDF
- Compact, lightweight edition
- Dispatched in 3 to 5 business days
- Free shipping worldwide - see info
- Durable hardcover edition
Tax calculation will be finalised at checkout
Purchases are for personal use only
Institutional subscriptions
Similar content being viewed by others

Nursing Management of the Burn Patient

Nursing Management of the Burn-Injured Person

Burned Beyond Recognition: Ethics of Care
American Burn Association (2019) Burn incidence and treatment in the U.S.—2016 . http://www.ameriburn.org/who-we-are/media/burn-incidence-fact-sheet . Accessed 7 Jan 2019
Institute for Clinical and Evaluative Services (2019) Injuries in Ontario ICES Atlas—2005. https://www.ices.on.ca/flip-publication/injuries-in-ontario . Accessed 7 Jan 2019
WHO International (2019) Burn fact sheet—March 6, 2018. https://www.who.int/news-room-fact-sheets/detail/burns . Accessed 7 Jan 2019
Ward J, Phillips G, Radotra I, Smailes S, Martin N (2018) Frailty: an independent predictor of burns mortality following inpatient admission. Burns 44:1895–1902. https://doi.org/10.1016/j.burns.2018.09.022
Article PubMed Google Scholar
Jeschke MG, Pinto R, Costford SR, Amini-Nik S (2016) Threshold age and burn size associated with poor outcomes in the elderly after burn injury. Burns 42:276–281. https://doi.org/10.1016/j.burns.2015.12.008
Article PubMed PubMed Central Google Scholar
Wearn C, Hardwicke J, Kitsios A, Siddons V, Nightingale P, Moiemen N (2015) Outcomes of burns in the elderly: revised estimates from the Birmingham Burn Centre. Burns 41:161–168. https://doi.org/10.1016/j.burns.2015.04.008
Article Google Scholar
Chin TL, Carrougher GJ, Amtmann D, McMullen K, Gibran NS (2018) Trends 10 years after burn injury: a Burn Model System National Database study. Burns 44:1882–1886. https://doi.org/10.1016/j.burns.2018.09.033
Butz DR, Zach Collier BA, O’Connor A, Magdziak M, Gottlieb LJ (2015) Is palmar surface area a reliable tool to estimate burn surface areas in obese patients? J Burn Care Res 36:87–91. https://doi.org/10.1097/BCR.0000000000000146
Thom D (2017) Appraising current methods for preclinical calculation of burn size—a pre- hospital perspective. Burns 43:127–136. https://doi.org/10.1016/j.burns.2016.07.003
Parvizi D, Girezlehner M, Wurzer P, Klein LD, Shoham Y et al (2016) BurnCare 3D software validation study; burn size measurement accuracy and inter-rater reliability. Burns 42:329–335. https://doi.org/10.1016/j.burns.2016.01.008
Goverman J, Bittner EA, Friedstat JS, Moore M, Nozari A, Ibrahim AE (2015) Discrepancy in initial pediatric burn estimates and its impact on fluid resuscitation. J Burn Care Res 36:574–579. https://doi.org/10.1097/BCR.0000000000000185
Crouzet C, Nguyen JQ, Ponticorvo A, Bernal NP, Durkin AJ, Choi B (2015) Acute discrimination between superficial-partial and deep-partial thickness burns in a pre-clinical model with laser speckle imaging. Burns 41:1058–1063. https://doi.org/10.1016/j.burns.2014.11.018
Duke JM, Randall SM, Fear MW, Boyd JH, O’Halloran E, Rea S, Wood FM (2016) Increased admissions for diabetes mellitus after burn. Burns 42:1734–1739. https://doi.org/10.1016/j.burns.2016.06.005
Sayampanathan AA (2016) Systematic review of complications and outcomes of diabetic patients with burn trauma. Burns 42:1644–1651. https://doi.org/10.1016/j.burns.2016.06.023
Article CAS PubMed Google Scholar
ISBI Guidelines Committee (2016) ISBI practice guidelines for burn care. Burns 42:953–1021. https://doi.org/10.1016/j.burns.2016.05.013
Wiktor AJ, Madsen I, Carmichael H, Smith T, Zanyk S (2018) Multilingual utilization of a mobile device app for triage and transfer of burn patients. J Burn Care Res 39:858–862. https://doi.org/10.1093/jbcr/iry041
Garcia DI, Howard R, Cina RP, Patel S, Ruggiero K (2018) Expert outpatient burn care in the home through mobile health technology. J Burn Care Res 39:680–684. https://doi.org/10.1093/jbcr/iry013
Martinez R, Rogers AD, Rode H (2018) The value of WhatsApp communication in pediatric burn care. Burns 44:947–955. https://doi.org/10.1016/j.burns.2017.11.005
Egro FM (2017) Basic burns management e-learning: a new teaching tool. J Burn Care Res 38:715–721. https://doi.org/10.1097/BRC.0000000000000462
Sen S, Johnston C, Greenhalgh D, Palmieri T (2016) Ventilator-associated pneumonia prevention bundle significantly reduces the risk of ventilator-associated pneumonia in critically ill burn patients. J Burn Care Res 37:166–171. https://doi.org/10.1097/BCR.0000000000000228
Friedman BC, Mian MAH, Mullins RF, Hassan Z, Shaver JR, Johnston KK (2015) Five-lumen antibiotic-impregnated femoral central venous catheters in severely-burned patients: an investigation of device utility and catheter-related bloodstream infection rates. J Burn Care Res 36:493–499. https://doi.org/10.1097/BCR.0000000000000186
Austin RE, Shahrokhi S, Bolourani S, Jeschke MG (2015) Peripherally-inserted central venous catheter safety in burn care: a single-center retrospective cohort review. J Burn Care Res 36:111–117. https://doi.org/10.1097/BCR.0000000000000207
Issler-Fisher AC, McKew G, Fisher OM, Harish V, Gottlieb T, Maitz PKM (2015) Risk factors and the effect of MRSA colonization on the clinical outcome of severely burnt patients. Burns 41:1212–1220. https://doi.org/10.1016/j.burns.2015.03.003
Heyneman A, Hoeksema H, Vandekerckhove D, Pirayesh A, Monstrey S (2016) The role of silver sulphadiazene in the conservative treatment of partial-thickness burn wounds: a systematic review. Burns 42:1377–1386. https://doi.org/10.1016/j.burns.2016.03.029
Haith LR, Stair-Buchmann ME, Ackerman BH, Herder D, Reigart CL, Stoering M et al (2015) Evaluation of Aquacel ® Ag for autogenous skin donor sites. J Burn Care Res 36:602–606. https://doi.org/10.1097/BCR.0000000000000212
Jeschke MG, Shahrokhi S, Finnerty CC, Branski LK, Dibildox M (2018) Wound coverage technologies in burn care: established techniques. J Burn Care Res 39:313–318. https://doi.org/10.1097/BCR.0b013e3182926129
Gee Kee EL, Kimble RM, Cuttle L, Khan A, Stockton KA (2015) Randomized controlled trial of three burns dressings for partial-thickness burns in children. Burns 41:946–955. https://doi.org/10.1016/j.burns.2014.11.005
Phelan I, Furness PJ, Fehily O, Thompson AR, Babiker NT, Lamb MA, Lindley SA (2019) A mixed-methods investigation into acceptability, usability and perceived effectiveness of active and passive virtual reality scenarios in managing pain with experimental conditions. J Burn Care Res 40:85–90. https://doi.org/10.1093/jbcr/iry052
Provencal S-C, Bond S, Rizkallah E, El-Baalbaki G (2018) Hypnosis for burn wound care pain and anxiety: a systematic review and meta-analysis. Burns 44:1870–1881. https://doi.org/10.1016/j.burns.2018.04.017
Scapin S, Echevarria-Guanilo ME, Fuculo PRB Jr, Goncalves N, Rocha PK, Coimbra R (2018) Virtual reality in the treatment of burn patients: a systematic review. Burns 44:1403–1416
Ford CG, Manegold EM, Randall CL, Aballay AM, Duncan CL (2018) Assessing the feasibility of implementing low-cost virtual reality therapy during routine burn care. Burns 44:886–895
McSherry T, Aterbury M, Gartner S, Helmond E, Searles D (2018) Randomized crossover study of immersive virtual rality to decrease opioid use during painful wound care procedures in adults. J Burn Care Res 39:278–285. https://doi.org/10.1097/BRC.0000000000000589
Nedelec B, Carrougher GJ (2017) Pain and pruritus post-burn injury. J Burn Care Res 38:142–145. https://doi.org/10.1097/BCR.0000000000000534
Hylan EJ, D’Cruz R, Harvey JG, Moir J, Parkinson C, Holland AJA (2015) An assessment of early child life therapy pain and anxiety management: a prospective randomized controlled trial. Burns 41:1642–1652. https://doi.org/10.1016/j.burns.2015.05.017
Singleton A, Preston RJ, Cochran A (2015) Sedation and analgesia for critically ill pediatric burn patients: the current state of practice. J Burn Care Res 36:440–445. https://doi.org/10.1097/BCR.0000000000000165
Wibbenmeyer L, Eid A, Kluesner K, Heard J, Zimmerman B, Kealey GP, Brennan T (2015) An evaluation of factors related to postoperative pain control in burn patients. J Burn Care Res 36:580–586. https://doi.org/10.1097/BCR.0000000000000199
Pham CH, Collier ZJ, Webb AB, Garner WL (2018) How long are burn patients really NPO in the perioperative period and can we effectively correct the calorie deficit using an enteral feeding, “catch-up” protocol? Burns 44:2006–2010. https://doi.org/10.1016/j.burns.2018.07.005
Ng JWG, Cairns SA, O’Boyle CP (2016) Management of the lower gastrointestinal system in burns: a comprehensive review. Burns 42:728–737. https://doi.org/10.1016/j.burns.2015.08.007
Stoecklin P, Delodder F, Pantet O, Berger MM (2016) Moderate glycemic control safe in critically ill adult burn patients: a 15 year cohort study. Burns 42:63–70. https://doi.org/10.1016/j.burns.2015.10.025
Kurmis R, Greenwood J, Aromataris E (2016) Trace element supplementation following severe burn injury: a systematic review and meta-analysis. J Burn Care Res 37:143–159. https://doi.org/10.1097/BCR.0000000000000259
Mushin OP, Bogue JT, Esquenazi MD, Toscano N, Bell DE (2017) Use of a home vacuum-assisted closure device in the burn population is both cost-effective and efficacious. Burns 43:490–494. https://doi.org/10.1016/j.burns.2016.03.038
Schulz A, Shoham Y, Rosenberg L, Rothermund I, Perbix W, Fuchs C, Lipensky A, Schiefer JL (2017) Enzymatic versus traditional surgical debridement of severely burned hands: a comparison of selectivity, efficacy, healing time and three month scar quality. J Burn Care Res 38:745–755. https://doi.org/10.1097/BCR.000000000000047
Fischer S, Wall J, Pomahae B, Riviello R, Halvorson EG (2016) Extra-large negative pressure wound therapy dressings for burns—initial experience with technique, fluid management and outcomes. Burns 42:457–465. https://doi.org/10.1016/j.burns.2015.08.034
Schulz A, Depner C, Lefering R, Kricheldorff J, Kastner S, Fuchs PC, Demir E (2016) A prospective clinical trial comparing Biobrane™ Dressilk and PolyMem ® dressings on partial-thickness skin donor sites. Burns 42:345–355. https://doi.org/10.1016/j.burns.2014.12.016
Tan H, Wasiak J, Paul E, Cleland H (2015) Effective use of Biobrane™ as a temporary wound dressing prior to definitive split-skin graft in the treatment of severe burn: a retrospective analysis. Burns 41:969–976. https://doi.org/10.1016/j.burns.2014.07.015
Austin RE, Merchant N, Shahrokhi S, Jeschke MG (2015) A comparison of Biobrane™ and cadaveric allograft for temporizing the acute burn wound: cost and procedural time. Burns 41:749–753. https://doi.org/10.1016/j.burns.2014.10.003
Nguyen TQ, Franczyk M, Lee JC, Grieves MR, O’Connor A, Gottlieb LJ (2015) Prospective randomized controlled trial comparing two methods of securing skin grafts using negative pressure wound therapy: vacuum-assisted closure and gauze suction. J Burn Care Res 36:324–328. https://doi.org/10.1097/BCR.0000000000000089
Parry I, Sen S, Pamieri T, Greenhalgh D (2019) Current trends in practice for early mobility with the burn population. J Burn Care Res 40:29–33. https://doi.org/10.1013/jbcr/iry049
McAleavey AA, Wyka K, Peskin M, Difede J (2018) Physical, functional and psychosocial recovery from burn injury are related and their relationship changes over time: a Burn Model System Study. Burns 44:793–799. https://doi.org/10.1016/j.burns.2017.12.011
Serghiou MA, Niszczak J, Parry I, Richard R (2016) Clinical practice recommendations for positioning of the burn patient. Burns 42:267–275. https://doi.org/10.1016/j.burns.2015.10.007
Voon K, Silberstein I, Eranki A, Phillips M, Wood FM, Edgar DW (2016) Xbox Kinect™ based rehabilitation as a feasible adjunct for minor upper limb burns rehabilitation: a pilot RCT. Burns 42:1797–1804. https://doi.org/10.1016/j.burns.2016.06.007
Parry I, Painting L, Bagley A, Lawada J, Molitor F, Sen S et al (2016) A pilot prospective randomized control trial comparing exercises using videogame therapy to standard physical therapy: 6 months follow-up. J Burn Care Res 36:534–544. https://doi.org/10.1097/BCR.0000000000000165
McGarry S, Burrows S, Ashoorian T, Pallathil T, Ong K, Edgar DW, Wood F (2016) Mental health and itch in burns patients: potential associations. Burns 42:763–768. https://doi.org/10.1016/j.burns.2016.01.016
Van Loey NE, Hofland HW, Hendrickx H, Van de Steenoven J, Boekelaar A, Nieuwenhuis MK (2016) Validation of the burns itch questionnaire. Burns 42:526–534. https://doi.org/10.1016/j.burns.2015.08.001
Everett T, Parker K, Fish J, Pehora C, Budd D, Kelly C et al (2015) The construction and implementation of a novel post-burn pruritus scale for infants and children aged five years or less: introducing the Toronto itch scale. J Burn Care Res 36:44–49. https://doi.org/10.1097/BCR.0000000000000129
Gauffin E, Oster C, Gerdin B, Ekselius L (2015) Prevalence and prediction of prolonged pruritus after severe burns. J Burn Care Res 36:405–413. https://doi.org/10.1097/BCR.0000000000000152
Brewin MP, Homer SJ (2018) The lived experience and quality of life with burn scarring—the results from a large-scale online survey. Burns 44:1801–1810. https://doi.org/10.1016/j.burns.2018.04.007
Martin L, Byrnes M, McGarry S, Rea S, Wood F (2017) Social challenges of visible scarring after severe burn: a qualitative analysis. Burns 43:76–83. https://doi.org/10.1016/j.burns.2016.07.027
Coghlan N, Copley J, Aplin T, Strong J (2017) Patient experience of wearing compression garments post-burn injury: a review of the literature. J Burn Care Res 38:260–269. https://doi.org/10.1097/BCR.0000000000000506
Tredget EE, Shupp JW, Schneider JC (2017) Scar management following burn injury. J Burn Care Res 38:146–147. https://doi.org/10.1097/BRC.0000000000000548
Issler-Fisher AC, Fisher OM, Smialkowski AO, Li F, VanSchalkwyk CP, Haertsch P, Maitz PKM (2016) Ablative fractional CO 2 laser for burn scar reconstruction: an extensive subjective and objective short-term outcome analysis of a prospective treatment cohort. Burns 43:573–582. https://doi.org/10.1016/j.burns.2016.09.014
Anthonissen M, Daly D, Janssens T, Van den Kerckhove E (2016) The effects of conservative treatments on burn scars: a systematic review. Burns 42:508–518. https://doi.org/10.1016/j.burns.2015.12.006
Holavanahalli RK, Helm PA, Kowalske KJ (2016) Long-term outcomes in patients surviving large burns: the musculoskeletal system. J Burn Care Res 37:243–254. https://doi.org/10.1097/BRC.0000000000000257
Sharp PA, Pan B, Yakuboff KP, Rothchild P (2016) Development of a best evidence statement for the use of pressure therapy for management of hypertrophic scarring. J Burn Care Res 37:255–264. https://doi.org/10.1097/BCR.0000000000000253
Nedelec B, Carter A, Forbes L, Hsu SCC, McMahon M, Parry I et al (2015) Practice guidelines for the application of non-silicone or silicone gels and gel sheets after burn injury. J Burn Care Res 36:345–374. https://doi.org/10.1097/BCR.0000000000000124
Simko LC, Espinoza LF, McMullen K, Herndon DN, Sumen O (2018) Fatigue following burn injury: a burn model system national database study. J Burn Care Res 39:450–456. https://doi.org/10.1097/BCR0000000000000625
Toh C, Li M, Finlay V, Jackson T, Burrows S, Wood FM, Edgar DW (2015) The brief fatigue inventory is reliable and valid for the burn patient cohort. Burns 41:990–997. https://doi.org/10.1016/j.burns.2014.11.014
O’Brien KH, Lustin V (2019) Examining the impact of psychological factors on hospital length-of-stay for burn survivors: a systematic review. J Burn Care Res 40:12–20. https://doi.org/10.1093/jbcr/iry040
Kornhaber R, Childs C, Cleary M (2018) Experiences of guilt, shame and blame in those affected by burns: a qualitative systematic review. Burns 44:1026–1039. https://doi.org/10.1016/j.burns.2017.11.012
Abrams TE, Ogletree RJ, Ratnapradipa D, Newmeister MW (2016) Adult survivors’ lived experience of burns and post-burn health: a qualitative analysis. Burns 42:152–162. https://doi.org/10.1016/j.burns.2015.09.011
Cockerham ES, Cili S, Stopa L (2016) Investigating the phenomenology of imagery following traumatic burn injuries. Burns 42:853–862. https://doi.org/10.1016/j.burns.2015.02.020
Attoe C, Pounds-Cornish E (2015) Psychosocial adjustment following burns: an integrative literature review. Burns 41:1375–1384. https://doi.org/10.1016/j.burns.2015.02.020
Bond S, Gourlay C, Desjardins A, Bodson-Clermont P, Boucher M-E (2017) Anxiety, depression and PTSD-related symptoms in spouses and close relatives of burn survivors: when the supporter needs to be supported. Burns 43:592–601. https://doi.org/10.1016/j.burns.2016.09.025
Reimer RB, Bay RC, Alam NB, Sadler IJ, Richey KJ, Foster KN et al (2015) Measuring the burden of pediatric burn injury for parents and caregivers: informed burn center staff can help to lighten the load. J Burn Care Res 36:421–427. https://doi.org/10.1097/BCR.0000000000000095
Hobbs K (2015) Which factors influence the development of post-traumatic stress disorder in patients with burn injuries? A systematic review of the literature. Burns 41:421–430. https://doi.org/10.1016/j.burns.2014.10.018
Cukor J, Wyka K, Leahy N, Yurt R, Difede J (2015) The treatment of posttraumatic stress disorder and related psychosocial consequences of burn injury: a pilot study. J Burn Care Res 36:184–192. https://doi.org/10.1097/BCR.0000000000000177
Martin L, Byrnes M, McGarry S, Rea S, Wood F (2017) Posttraumatic growth after burn in adults: an integrative literature review. Burns 43:459–470. https://doi.org/10.1016/j.burns.2016.09.021
Levi B, Krapt CT, Shapior GD, Trinh NHT, Dore EC (2018) The associations of gender with social participation of burn survivors: a life impact burn recovery evaluation profile study. J Burn Care Res 39:915–922. https://doi.org/10.1093/jbcr/iry007
Ohrtman EA, Shapiro GD, Simco LC, Doredy E, Slavin MD (2018) J Burn Care Res 39:1022–1028. https://doi.org/10.1093/jbcr/iry038
Baldwin S, Yuon H, Liao J, Grieve B, Heard J (2018) Burn survivor quality of life and barriers to support program participation. J Burn Care Res 39:823–830. https://doi.org/10.1093/jbcr/irx058
Dekel B, van Niekerk A (2018) Women’s recovery, negotiation of appearance and social re-integration following a burn. Burns 44:841–849. https://doi.org/10.1016/j.burns.2017.12.004
Waqas A, Turk M, Naveed S, Amin A, Chaudhry A (2018) Perceived social support among patients with burn injuries: a perspective from the developing world. Burns 44:168–174. https://doi.org/10.1016/j.burns.2017.06.014
Barnett BS, Mulenga M, Kisa MM, Charles AG (2017) Qualitative analysis of a psychological supportive counseling group for burn survivors and families in Malawi. Burns 43:602–607. https://doi.org/10.1016/j.burns.2016.09.027
Papamikrouli E, Van Schie CMH, Schoenmaker J, Boekelaar-vd Berge A, Gebhardt WA (2017) Peer support needs among adults with burns. J Burn Care Res 38:112–120. https://doi.org/10.1097/BCR.0000000000000424
Nguyen NT, Lorrain M, Pognon-Hanna JN, Elfassy C, Calva V, de Oliveira A, Nedelec B (2016) Barriers and facilitators to work reintegration and burn survivors’ perspectives on educating work colleagues. Burns 42:1477–1486. https://doi.org/10.1016/j.burns.2016.05.014
Arshad SN, Gaskell SL, Baker C, Ellis N, Potts J, Concill T et al (2015) Measuring the impact of a burns school reintegration program on the time taken to return to school: a multi-disciplinary team intervention for children returning to school after a significant burn injury. Burns 41:727–734. https://doi.org/10.1016/j.burns.2014.10.015
Palmu R, Partonen T, Suiminen K, Vuola J, Isometsa E (2015) Return to work six months after burn: a prospective study at the Helsinki burn centre. Burns 41:1152–1160. https://doi.org/10.1016/j.burns.2015.06.010
Pham TN, Carrougher GJ, Martinez E, Lezotte D, Rietschel C, Holavanahalli R et al (2015) Predictors of discharge disposition in older adults with burns: a study of the burn model systems. J Burn Care Res 36:607–612. https://doi.org/10.1097/BCR.0000000000000216
Markiewitz N, Cox C, Krout K, McColl M, Caffrey JA (2019) Examining the rates of anxiety, depression and burnout among providers at a regional burn center. J Burn Care Res 40:39–43. https://doi.org/10.1093/jbcr/iry042
Shoham DA, Mundt MP, Gamelli RL, McGaghie WC (2015) The social network of a burn unit team. J Burn Care Res 36:551–557. https://doi.org/10.1097/BCR.0000000000000218
Van Fosson CA, Jones TL, Yoder LH (2018) Monthly variation of unfinished nursing care at the US Army Burn Center. Burns 44:1910–1919. https://doi.org/10.1016/j.burns.2018.03.008
Christiansen M, Wallace A, Newton J, Caldwell N, Mann-Salinas E (2017) Improving teamwork and resilience of burn center nurses through a standardized staff development program. J Burn Care Res 38:708–714. https://doi.org/10.1097/BCR.0000000000000299
Olszewski A, Yanes A, Stafford J, Greenhalgh DG, Palmieri TL, Sen S, Tran N (2016) Development and implementation of an innovative burn nursing handbook for quality improvement. J Burn Care Res 37:20–24. https://doi.org/10.1097/BCR.0000000000000299
Download references
Author information
Authors and affiliations.
Sunnybrook Health Sciences Centre, Toronto, ON, Canada
Judy Knighton
You can also search for this author in PubMed Google Scholar
Corresponding author
Correspondence to Judy Knighton .
Editor information
Editors and affiliations.
Ross Tilley Burn Centre, Sunnybrook Health Sciences Centre, Toronto, ON, Canada
Marc G. Jeschke
Division of Plastic, Aesthetic and Reconstructive Surgery Department of Surgery, Medical University of Graz, Graz, Austria
Lars-Peter Kamolz
Department of Surgery, Division of Plastic and Reconstructive Surgery, University of Toronto, Toronto, ON, Canada
Shahriar Shahrokhi
Rights and permissions
Reprints and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter
Knighton, J. (2021). Nursing Care of the Burn Patient. In: Jeschke, M.G., Kamolz, LP., Shahrokhi, S. (eds) Burn Care and Treatment. Springer, Cham. https://doi.org/10.1007/978-3-030-39193-5_9
Download citation
DOI : https://doi.org/10.1007/978-3-030-39193-5_9
Published : 22 December 2020
Publisher Name : Springer, Cham
Print ISBN : 978-3-030-39192-8
Online ISBN : 978-3-030-39193-5
eBook Packages : Medicine Medicine (R0)
Share this chapter
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Publish with us
Policies and ethics
- Find a journal
- Track your research

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Indian J Plast Surg
- v.43(Suppl); 2010 Sep
The pivotal role of nursing personnel in burn care
Elisabeth greenfield.
Colonel (Retired), United States Army Nurse Corps,
The nurses play an important role in the overall management of a burn patient. They must be well versed with the various protocols available that can be used to rationally manage a given situation. The management not only involves medical care but also a psychological assessment of the victim and the family. The process uses a scientific method to combine systems theory with the art of nursing, entailing both problem solving techniques and a decision making process. It involves assessment of the patient to arrive at a diagnosis and then determining the patient goals.An action plan is implemented and is evaluated in the context of patient response. The article discusses many such scenarios in burn patients and outlines the nursing care plans.
Optimal care of the burn patient requires a distinctive multidisciplinary approach. Positive patient outcomes are dependent on the composition of the burn care team and close collaboration among its members. At the centre of this team is the burn nurse, the coordinator of all patient care activities. The complexity and multisystem involvement of the burn patient demand that the burn nurse possess a broad-based knowledge of multisystem organ failure, critical care techniques, diagnostic studies and rehabilitative and psychosocial skills. The nurse oversees the total care of the patient, coordinating activities with other disciplines such as occupational and physical therapy, social services, nutritional services and pharmacy. At the same time, the burn nurse is also a specialist in wound care. As a burn wound heals, either spontaneously or through excision and grafting, the nurse is responsible for wound care and for noting subtle changes that require immediate attention, prevention of infection and pain management. The nurse’s role is continuously expanding. Nurses are conducting nursing research and contributing to evidence-based practice of burn care. Practice guidelines, critical pathways and nursing care plans are all tools that help define and refine the nurse’s role in burn care.
EVIDENCE-BASED PRACTICE
Recent advances in health care technology, public disclosure and published information as well as a realization that we are obligated to reduce prohibitive health care costs are some of the several factors that have promoted the interest in and development of evidence-based practice or a more objective, scientific approach to health care. Previous standards of care, based largely on experience, are now being used as a control in randomized clinical trials. Both are evaluated using specific endpoints such as cost, benefit and risk.[ 1 ] Barnsteiner and Provost[ 2 ] suggest that there are both research and nonresearch elements in evidence-based practice. Clinical judgment and critical thinking are equally vital to the process.
PRACTICE GUIDELINES
Practice guidelines have evolved from the evidence-based practice revolution. They are intended to provide recommendations based on critical reading and interpretation of the current literature for managing specific problems. They attempt to define not only the best but also the most cost-effective treatment. When correctly written, practice guidelines can help minimize practice variances that lead to poor patient outcomes and high health care costs. Because burn centres are few in number and are geographically scattered, there are few burn-focused multicentre trials. Many burn research studies involve only one centre, animal models and small sample sizes. Their limited strength of any demonstrated findings and study conclusions is obvious. There are currently a minimal number of randomized controlled clinical trials that have validated burn clinical care practices. Of the few that do exist, many have been extrapolated from research performed in other critical care patient populations. Recent efforts by the American Burn Association to initiate and support collaboration between burn centres to conduct multicentre trials are on-going. The resulting research studies should generate evidence-based practice and greatly impact future burn care. Additionally, the American Burn Association Committee on Organization and Delivery of Burn Care has published updated Practice Guidelines that were originally published in 2000 as a supplement to the Journal of Burn Care and Rehabilitation . The revised and updated recommendations represent the work of the 2004 to 2006 Committee on the Organization and Delivery of Burn Care.[ 3 ]
CRITICAL PATHWAYS
Critical pathways that were developed in the late 1990s as another measure to guide medical and nursing practice are more detailed disease and institution-specific protocols that are usually based on practice guidelines. They define the sequence of standardized, multidisciplinary processes or critical events that must occur in order for a particular patient to move toward desired outcomes within a defined period of time. The goal is to use an interdisciplinary perspective to identify expectations of patient care, improve quality care as demonstrated by improving patient outcomes, decreasing length of stay, decreasing readmissions, decreasing costs and increasing patient satisfaction.[ 4 ] They define anticipated length of stay, delineate desired outcomes and goals, provide directions for care, identify the best practice model for a specific group of patients, promote collaboration between disciplines and provide an opportunity for continuous improvement in care delivery.
Critical pathways represent the standard of care in average cases and were developed in response to economic incentives and pressures as they encourage the proper use of resources, which in turn reduces waste of time, energy and material. They promote well-coordinated, well-communicated continuity of care through collaborative practice and facilitate adherence to regulations imposed by regulatory bodies, reduce length of stay and resource utilization and reduce practice variances and adverse outcomes. Table 1 summarizes some of the various purposes that are served by critical pathways.
Purposes of critical pathways
| Improve clinical outcomes |
| Reduce adverse outcomes |
| Greater consistency in the delivery of patient care |
| Improve staff skill levels |
| Improve basis for performance evaluation |
| Reduce exposure to liability |
| Better preparation for accreditation and American Burn Association |
| Verification |
| Increase efficiency and productivity |
Implementation of critical pathways is challenged by many pros and cons. While they provide a useful guideline in assessment, intervention and evaluation, they must be constantly monitored and updated based on the patient’s response to therapy. Further, they must be individualized for each patient’s needs.[ 5 ] They should not to be construed as a cookbook mentality. They are not laws that must be rigidly followed. Contrary to popular belief, they do not annihilate individuality. It is important to remember that they are guidelines that outline the current standards of care. They also provide a useful educational tool for all members of the burn care team as they reflect each team member’s responsibilities. The nurse spends the most time with a patient and is in the best position to monitor progress, report changes and coordinate activities of other team members. Critical pathways are most commonly depicted along two axes, one representing time and one representing aspects of care, including laboratory studies, consult services, nutrition, pharmaceutical support, patient education, etc.
Another useful element of critical pathways is their ability to identify variances, or unexpected events, both positive and negative. The analysis of these variances provides an excellent framework for a quality improvement program and can help focus improvement efforts in any of the four major areas: caregiver or provider, hospital or system, patient or family and/or community variance.
NURSING DIAGNOSES AND CARE PLANS
During all phases of injury, assessment by the nurse must focus on early detection or prevention of complications associated with moderate to severe burn injury. Frequent monitoring is required to assess indices of essential organ function. A list of the more common actual or potential nursing diagnoses for patients with thermal injuries in the resuscitative, acute and rehabilitative phases of care is presented in Table 2 .[ 6 ]
Nursing diagnoses
| Ineffective Airway Clearance | Tracheal edema due to inhalation injury |
| Impaired gas exchange | Interstitial pulmonary edema |
| Fluid volume deficit | Fluid shifts, dieresis, or evaporative water loss |
| Altered tissue perfusion | Impaired extremity vascular perfusion with circumferential burns |
| Risk for infection | Invasive therapy and loss of integument |
| Hypothermia | Decreased heat production and increased heat loss secondary to thermal injury |
| Pain | Thermal injury |
| Ineffective coping | Acute stress from injury and life-threatening crisis |
| Altered nutrition, less than body requirements | Increased metabolic demands |
| Impaired skin integrity | Thermal injury |
| Self-Care deficit | Contractures, therapeutic splinting and positioning |
| Altered family processes | Potential life style and role changes |
| Altered body image and self-esteem | Disfigurement or dysfunction following burn injury |
The nurse’s goal is to deliver patient-focused care using a holistic approach. In order to accomplish this, the nursing process was introduced in the 1950s and has served as the framework for nursing care delivery ever since. The process uses a scientific method to combine systems theory with the art of nursing. It entails both problem-solving techniques and a decision-making process.[ 7 ] The nursing process consists of five steps, which together facilitate the delivery of high-quality, individualized patient care. The five steps are as follows:
Assessment is the first step of the process and is a systemic approach to collecting information about the patient. It includes not only symptoms and physiologic factors but also social, cultural, psychological and spiritual aspects of the patient’s life.
Diagnosis, the second step, is the nurse’s analysis of the assessment. It is sometimes also referred to as needs identification.
Outcomes/planning uses the two previous steps to determine patient goals, both long- and short term, desired outcomes and appropriate nursing interventions. These outcomes and interventions are written as the nursing care plan and serve as a written guide for all health care professionals. An example of a written nursing care plan for the patient in the resuscitative and acute care phases of a major burn injury is provided in by Molter et.al and Ahrns-Klas.[ 8 , 9 ]
Implementation is the action portion of the nursing process and care plan.
Evaluation of both the patient’s response to interventions and progress toward achieving outcome goals is critical. Both need to be documented and the plan of care modified accordingly.
The nursing process is both dynamic and interactive. It is a continuous cycle of logical progression from one step to the next. Because each step relies of the accuracy of the previous step, data must be validated. Clearly, the plan that is developed from the nursing process must be adjusted based on the interactions with other disciplines in order to meet the continuously changing needs of the patient. In creating the care plan, the nurse uses theory, nursing judgment and clinical expertise. In many ways, the nursing process and written plan of care help define the nurse’s role. By using the nursing process, the nurse is able to establish autonomy and a common ground within the practice of nursing through nursing diagnoses. The continuous review of the care plan facilitates evaluation and documentation of outcomes and helps provide the basis for establishing standards of care.
NURSING DIAGNOSIS 1
Ineffective airway clearance and impaired gas exchange related to tracheal oedema or interstitial oedema secondary to inhalation injury and/or circumferential torso burn manifested by hypoxemia and hypercapnia
Patient outcomes
- Adequate airway clearance and gas exchange.
- Partial pressure of oxygen >90 mmHg; partial pressure of arterial carbon dioxide <45 mmHg; oxygen saturation >95%.
- Respiration rate 16–20 breaths/min and unlaboured; breath sounds present and clear in all lobes; chest wall excursion symmetrical and adequate.
- Mentation clear; patient mobilises secretions, which are clear to white.
Nursing interventions
- Monitor oxygen saturation every hour, arterial blood gases as needed; Chest X-ray as ordered
If not intubated, assess for stridor, hoarseness and wheezing every hour
- Administer humidified oxygen as ordered
Suction every 1–2 h or as needed
Monitor sputum characteristics and amount
- Turn every 2 h to mobilize secretions
- Elevate head of bed
- Schedule activities to avoid fatigue
- Assess oxygenation and ventilation
- Evaluate respiratory status and Response to treatment
- Expedite elimination of carbon monoxide and prevent/treat hypoxemia
- Promote lung expansion, ventilation, clearing of secretions and clear airway
- Facilitate lung expansion
- Decrease ventillatory effort and dyspnea
NURSING DIAGNOSIS 2
Adequate fluid volume
Deficient fluid volume secondary to fluid shifts into the interstitium and evaporative loss of fluids from the injured skin
- Heart rate 80–120 beats/min; blood pressure adequate in relation to pulse and urine output; optimal tissue perfusion; nonburn skin warm and pink
- Hourly urine output 30–50 ml/h; 75–100 ml/h in electrical injury; 1 ml/kg/h in children <30 kg body weight
- Weight gain based on volume of fluids given in the first 48 h, followed by diuresis over the next 3–5 days
- Laboratory values within normal limits; urine negative for glucose and ketones
- Monitor: vital signs and urine output q1h until stable; mental status every hour for at least 48 h.
- Titrate fluid requirements to maintain urinary output and haemodynamic stability
- Record daily weight and hourly intake/output measurements; evaluate trends
- Assess perfusion and oxygenation status
- Restore intravascular volume.
- Evaluate fluid loss and replacement.
- Monitor serum electrolytes, glucose, creatinine, haematocrit, blood urea nitrogen as required by patient status
- Evaluate need for fluid and electrolyte replacement resulting from large fluid and protein shifts.
NURSING DIAGNOSIS 3
Ineffective tissue perfusion related to compression and impaired vascular circulation in the extremities with circumferential burns, as demonstrated by decreased or absent peripheral pulses.
- Adequate tissue perfusion, as manifested by strong peripheral pulses.
- No tissue injury in the extremities secondary to inadequate perfusion from oedema or eschar.
- Assess peripheral pulses every hour for 72 h. Notify the physician of changes in pulses, capillary refill or pain capillary refill or pain
- Elevate upper and lower extremities
- Be prepared to assist with escharotomy or fasciotomy
- Assess peripheral perfusion and the need for escharotomy
- Decrease oedema formation
- Allows oedema expansion and restore peripheral perfusion
NURSING DIAGNOSIS 4
Acute pain related to burn trauma.
- Relief of pain.
- Identifies factors that contribute to pain. Verbalizes improved comfort level.
- Physiological parameters within normal limits and remain stable after administration of narcotic analgesia.
- Monitor physiological responses to pain, such as increased blood pressure increased heart rate, restlessness and nonverbal cues. Use validated tools in each patient to assess pain and anxiety
- Assess response to analgesics or other interventions
- Evaluate effectiveness of interventions
- Administer analgesic and/or anxiolytic medication as ordered; administer IV during critical care phases
- Medicate patient before bathing, dressing changes and major procedures as needed
- Use nonpharmacological pain-reducing methods as appropriate
- Pain responses are variable and unique to each patient
- Facilitate pain relief. Intramuscular/ intravenous, during critical care phases, medications not consistently absorbed
- Assist patient to perform at higher level as needed of the function
- Reduce need for narcotics
NURSING DIAGNOSIS 5
Risk for infection related to loss of skin, impaired immune response and invasive therapies.
- Absence of infection.
- No inflamed burn wound margins.
- No evidence of burn wound, donor site or invasive catheter site infection.
- Autograft or allograft skin is adherent to granulation tissue.
- Body temperature and white blood cell count within normal limits.
- Sputum, blood and urine cultures negative.
- Glycosuria, vomiting, ileus,and/or change in mentation absent.
- Assess temperature and vital signs and characteristics of urine and sputum every 1–4 hours
- Monitor white blood cells, burn wound healing status and invasive catheter sites
- Ensure appropriate protective isolation; provide meticulous wound care; educate visitors in burn unit guidelines
- Facilitate early detection of developing infections
- Prevent infection by decreasing exposure, to pathogens
NURSING DIAGNOSIS 6
Risk for injury.
Gastrointestinal bleeding related to stress response.
Imbalanced nutrition
Less than body requirements related to paralytic ileus and increased metabolic demands secondary to physiological stress and wound healing.
- Absence of injury and adequate nutrition.
- Decreased gastric motility and ileus resolved.
- No evidence of gastrointestinal haemorrhaging.
- Enteral feedings absorbed and tolerated.
- Daily requirement of nutrients consumed.
- Positive nitrogen balance.
- Progressive wound healing.
- 90% of preburn weight maintained.
- Place nasogastric tube for gastric decompression in >20% TBSA burns
- Assess abdomen and bowel sounds every 8 hours
- Assess NG aspirate (color, quantity, pH, and hemocult blood); monitor stool for hemocult blood
- Administer stress ulcer prophylaxis
Provide high-calorie/protein supplements
Record all oral intake and count calories
- Schedule interventions and activities to avoid interrupting feeding times
- Monitor weight daily or biweekly
- Prevent nausea, emesis, and aspiration from ileus
- Evaluate resolution of decreased gastric motility
- Facilitate early detection of development of gastrointestinal ulcer
- Prevent stress ulcer development
- Caloric/protein intake must be adequate to maintain positive nitrogen balance and promote healing
- Pain, fatigue, or sedation interferes with desire to eat
- Assess tolerance and response to feeding interventions
NURSING DIAGNOSIS 7
Risk for hypothermia related to loss of skin and/or external cooling.
Patient outcome
Normothermia.
Rectal/core temperature 37°C (98.6°F)–38.3°C (101°F).
- Monitor and document rectal/core temperature every 1 to 2 hours; assess for shivering
- Minimize skin exposure; maintain environmental temperatures
- For temperature <37° C (98.6° F), institute rewarming measures
- Evaluate body temperature status
- Prevent evaporative and conductive losses
- Prevent complications
NURSING DIAGNOSIS 8
Impaired physical mobility and self-care deficit related to burn injury, therapeutic splinting and immobilization requirements after skin graft and/or contractures.
- Physical mobility.
- Demonstrates ability to care for burn wounds.
- No evidence of permanent decreased joint function.
- Verbalises understanding of plan of care.
- Vocation resumed without functional limitations or adjustment to new vocation.
- Perform active and passive range of motion exercises to extremities every 2 hours while awake. Increase activity as tolerated. Reinforce importance of maintaining proper joint movement/function, alignment with splints
- Elevate extremities
- Provide pain relief measures before self-care activities and occupational and physical therapy
- Explain procedures, interventions, and tests in clear, simple, age-appropriate language
- Promote use of adaptive devices as needed to assist in self-care and mobility
- Prevent contractures and loss of
- Decrease edema and promote range of motion and mobility
- Facilitate mobility; assist performance at a higher level of function
- Patient more likely to participate and adhere if understands purpose
- Decrease dependency
NURSING DIAGNOSIS 9
Risk for ineffective individual coping and disabled family coping related to acute stress of critical injury and potential life-threatening crisis.
- Effective coping.
- Verbalises goals of treatment regimen.
- Demonstrates knowledge of support systems.
- Able to express concerns and fears.
- Patient’s and family’s coping is functional and realistic for the phase of hospitalisation.
- Orient patient and family to unit guidelines and support services; provide written information and reinforce frequently; involve in plan of care. Support adaptive and functional coping mechanisms
- Use interventions to reduce fatigue and pain
- Use social worker for assistance in discharge planning
- Consult psychiatric services for inadequate coping skills or substance abuse treatment
- Promote use of group support sessions
- Decrease fear and anxiety
- Adequate pain control and rest facilitate patient coping
- Provide expert consultation and intervention.
- Assist patient and family in understanding experiences, reactions, and methods of coping
The importance of a multidisciplinary approach to patient care cannot be overstated. At the centre of this team is the nurse. The burn nurse’s assessments, observations and evaluations of the patient’s response to interventions are crucial to preventing complications and make the critical difference in patient outcomes.
Source of Support: Nil
Conflict of Interest: None declared.
Lippincott ® NursingCenter ®
- Journal Index
Nursing made Incredibly Easy!
- Nursing assessment and care...
Nursing assessment and care of major burn injuries

January/February 2023, Volume 21 Number 1 , p 6 - 13
Earn 1.5 Contact Hours
- Miller, Nichole DNP, AGACNP-BC
Prioritize the patient's airway, the cause of the burn, burn depth, and the affected body surface area during the initial assessment to decrease the risk of burn shock.
Article Content
Major burn injuries are one of the worst insults the body can endure and require intense specialty care. Whereas burns are traditionally thought of as a skin injury, a major burn can impact every system in the body within minutes of injury. In the US, a burn injury requires medical intervention every 30 minutes and between 4,000 and 6,000 people die from burn-related injuries each year. 1 There are approximately 120 burn centers in the US and only half of these hold certification by the American Burn Association. 2 This means that most people don't have direct access to a burn center and need to be stabilized at a local hospital after their initial injury. Therefore, it's important that everyone working in the acute setting, especially the nurse who's the first point of care, has some basic understanding of burn assessment and treatment.
| Figure. No caption available. |
Factors such as geographic location, gender, and extremes of age increase the risk of sustaining a burn injury. 1 It's a common misconception that most major burn injuries are the result of house fires; these incidents only account for approximately 4% of all burn admissions. 1 The Southeastern US has the highest incidence of major burn injuries. Men are twice more likely than women to sustain a major burn injury. Common causes of adult burn injuries include electrical injuries, work-related accidents, automobile fires, or burning trash or yard debris. 2 At-risk populations such as children, older adults, and persons with a disability are more likely to suffer burn injuries due to mobility restrictions and decreased coordination.
Burn classifications
Burns are classified in several different ways. To treat a burn injury appropriately, you'll need to know the cause of the injury, the depth of the burn, and the total skin involvement. Burn causes include thermal, chemical, and electrical contact. The depth of a burn is measured by the depth that the burn extends. Depth is separated into partial-thickness and full-thickness burns. Burns can also be classified in degree of injury from first through fourth. Partial-thickness burns include first- and second-degree burns, and full-thickness burns include third- and fourth-degree burns. 3
Partial-thickness burns
First-degree burns are superficial burns that only involve the epidermis. First-degree burns appear red without any blistering. The skin may feel tight, irritated, and painful. The skin will blanche when pressure is applied. 3 Sunburn is the most common example of a first-degree burn injury. First-degree burns are often uncomfortable but are self-limiting and generally don't require medical intervention unless there are additional complications, such as dehydration, or they encompass a large surface area.
Second-degree burns involve the epidermis and the dermis. Second-degree burns can be superficial or extend deeper into the dermis. Skin with second-degree burns can appear red with fluid-filled or open blisters. Deep second-degree burns may appear red, pale pink, or yellow in color. 3 The wound bed may be wet or dry. Deep second-degree burns are often difficult to distinguish from third-degree burns and often take an extended period to heal without surgical intervention.
Full-thickness burns
Third-degree or full-thickness burns extend through the dermis and into the subcutaneous tissue. In full-thickness burns, the entire skin surface has been damaged. These types of burns appear pale white, gray, yellow, dark red, or even charred. 3 The skin is often tight, appears "leathery," and provides little flexibility. The areas don't blanche with pressure and likely won't heal without surgical intervention.
Fourth-degree burns aren't often discussed but are an important classification for nurses to distinguish. Fourth-degree burns include any burn that involves damage to the deeper structures such as tendon and bone. 3 Fingers and toes are more susceptible to fourth-degree burns. Most fourth-degree burns will result in amputation due to bone injury.
Sizing of a burn injury
The size and depth of a burn injury directly impacts the level of care that the patient will require. Large burns require extensive specialized care for the best possible outcomes. Estimation of the total affected body surface area is one of the most important initial assessments when caring for a burn injury. Burn size will dictate many aspects of care, such as the fluid volume the patient will need for resuscitation and potential resources that'll be required to appropriately care for the patient. An accurate estimation of burn size is important but can often be difficult for nurses who don't frequently assess patients with burn injuries. 4 Clinicians are more likely to overestimate the total body surface area (TBSA) of a burn injury than underestimate, but both can increase patient mortality.
There are several different methods of estimating the percentage of body surface area covered by burns, the most common being the rule of nines (see Rule of nines ). This model divides the body into different sections and assigns each section with a percentage. In the rule of nines, the entire head is worth 9%, the torso is worth 36%, the arms through the hands are worth 9%, each leg is worth 18%, and the genitals are worth 1%. The percentage is assigned to the entire area. If only part of the area is burned, then only part of the percentage would be awarded. The rule of nines is also used with children; however, surface area percentage is calculated differently due to the difference in body ratios.
Initial burn management
The first 48 hours are the most critical period in the care of patients with burns. Nursing priorities in the initial management of patients with burns include airway protection, fluid resuscitation, warming measures, and evaluation of the burned tissue. 1 Airway evaluation and protection are priorities for patients who may have sustained an inhalation injury or burns to the airways. Patients involved in structure fires, automobile fires, or fires in any enclosed spaces are at risk for inhalation injury.
Airway and inhalation injuries
Patients with inhalation injuries may present with respiratory symptoms such as shortness of breath, cough, and hypoxia. Other symptoms include hoarse voice, soot in the nose or mouth, or soot in airway secretions. Inhalation injuries often accompany facial burns. Patients with facial burns should be assessed immediately for potential inhalation injury and monitored closely for changes. Airway protection is important due to the risk of airway swelling. Patients with facial burns and inhalation injuries often require intubation and mechanical ventilation for airway protection. 1
Patients involved in structure fires, especially in enclosed spaces, are also at risk for carbon monoxide and cyanide poisoning. When objects burn, they release carbon monoxide, which has a stronger bond than oxygen to the hemoglobin, leading to severe hypoxia and death. Carbon monoxide levels, otherwise known as carboxyhemoglobin, should be drawn as soon as poisoning is suspected. Spo 2 isn't an accurate assessment in a patient with carbon monoxide poisoning and shouldn't be used to determine oxygenation.
Patients with carbon monoxide poisoning or suspected poisoning should be placed on 100% Fio 2 for 12 to 24 hours. Patients with elevated levels of carbon monoxide will likely require intubation due to inhalation injury, but all patients should be placed on 100% FiO 2 even if not intubated. 5 Repeat carboxyhemoglobin testing should be checked 5 to 8 hours after the initial test to ensure complete washout. In severe cases of carbon monoxide poisoning, hyperbaric oxygenation should be considered.
| Figure. Rule of nines |
Another point for nurses to consider is cyanide. If a patient has carbon monoxide poisoning or was in a building for a prolonged time, it's important to consider the risk of cyanide poisoning. 1 Cyanide is released when plastics and coated textiles burn. These are often present in burns involving mobile homes, RVs, and campers with plastic walls, or upholstery and rugs that contain plastic or coated fibers. Treatment should be given if the carbon monoxide level is significantly elevated or if there's a high suspicion of cyanide toxicity.
Burn shock and fluid resuscitation
Within minutes of a major burn injury, the permeability of the vascular changes causes a significant fluid shift from the intravascular space to the tissues. This shift leads to burn shock. Patients with burns require large amounts of I.V. fluids to prevent and manage burn shock. Rapid infusion of I.V. fluids is required to maintain perfusion to organs and prevent organ failure. The patient with burns can require several liters of fluid an hour in the first 24 to 48 hours. Lactated Ringer's solution is the most common fluid used in the resuscitation process. 6,7
Burn resuscitation in the first 24 hours is key to decreasing mortality and morbidity. Too little or too much fluid can have a detrimental effect on patient outcome. There are many different tools to estimate the volume of fluid required to resuscitate a patient with burns. 8 The Parkland Formula for Burns is considered the standard (see Parkland calculation example ). The formula is based on burn size, TBSA, and patient weight to calculate the requirements. Half of the required fluid is administered to the patient within the first 8 hours. Time is calculated from the point of injury, not the time the patient presents to the hospital. This method requires accurate estimation of burn size.
Large burn injuries often require aggressive fluid resuscitation for the first 24 to 48 hours after the initial burn injury to prevent hypovolemic shock. Many patients will also require vasopressors for hemodynamic support. 9 These should be used for shock management and shouldn't be used as a replacement for adequate fluid resuscitation. Norepinephrine is recommended as the first-line vasopressor in patients with burns. Vasopressin is often added as a second-line agent.
The nurse should monitor urine output hourly in any patient requiring fluid resuscitation. Place a urinary catheter to facilitate accurate measurements. Fluids may need to be adjusted in patients with shock symptoms or low urine output. 4 If a patient's urine output doesn't respond to fluid resuscitation, they may require emergent renal replacement therapy. 7,10 Most significant burn injuries will have some level of acute kidney injury.
Temperature management
Burn injuries cause significant injury to the skin, leading to loss of body heat and difficulty with temperature regulation. 1 Patients with burns can develop hypothermia quickly; therefore, continuous temperature monitoring should be performed when possible. Significant hypothermia can lead to bradycardia, hypotension, and coagulopathy. Patients should be kept warm with regular blankets, shock blankets, airflow warming blankets such as a Bair Hugger device, and/or head covers. Any wet clothing should be removed immediately on initial presentation. If the patient doesn't respond to the conventional methods, of warming detailed above, other methods, such as esophageal warming probes or centrally placed warming catheters, may be required.
Pain management
Pain management is an important part of the initial care of large burns. Burn injuries are extremely painful and pain should be treated. Most large burn injuries will require intubation and mechanical ventilation to allow for continuous infusion of medications for pain control and sedation. Some patients may even require intubation for pain control and care.
As there are no standard recommendations for what medications to use for pain management in burn injuries, a multi-modality approach is often used to target multiple methods of pain control. Nonsteroidal anti-inflammatory drugs are often avoided in large burns because of the risk of acute kidney injury and bleeding. Propofol isn't recommended for sedation in burn injuries because it's been shown to cause fatty liver disease in patients with burns.
Fentanyl and versed infusions are often used in the first 24-48 hours for sedation and pain management, respectively. 11,12 Dexmedetomidine can be used to treat pain in smaller burn injuries, nonintubated patients, or later in the clinical treatment when patients must be more alert and interactive. Enteral medications can be introduced 24 to 48 hours after the injury. Methadone or other long-acting narcotics can be added to the analgesic routine. Gabapentin or pregabalin are often used in combination with narcotics to target pain related to damaged nerves.
Initial wound management
The initial burn management depends on the size, depth, and location of the burns. Full-thickness, circumferential burns can lead to compartment syndrome due to restrictive burn tissue. Circumferential burns to the extremities can lead to loss of limbs if the pressure isn't released. Escharotomies are an emergent intervention that require a surgeon to make incisions in the tissue to release restrictive burn tissue. 1 Escharotomies are commonly performed on the limbs but may also be performed on the chest and abdomen.
Patients with major burn injuries should be transferred to a certified burn center for the best outcome (see Burn center referral criteria ). They will require multiple surgical interventions. Initial wound management can vary depending on the facility's capabilities. The priority is to keep the patient warm and to avoid hypothermia. If the patient is warm, they can be put into moist sterile dressings. Moisten dressings with saline or an antimicrobial such as Dakin solution. If the patient is hypothermic, you can cover the patient with sterile towels or a sterile sheet until the patient is warm.
Nonsurgical management
Minor burn injuries are superficial partial-thickness burns that total less than 10% of the body. Some minor burns may be treated with topical management alone. This usually involves topical antimicrobials such as silver sulfadiazine. Oral antibiotics aren't usually required for minor burn injuries unless the wound is infected or there's a delayed presentation. Patients should receive a tetanus vaccine if they haven't received one in the last 5 years.
Special consideration should be given to burns to the hands, face, genitals, over joints, and any circumferential burns. According to the American Burn Association, burns to these locations should be evaluated in a certified burn center. Even small burns to these areas should be referred because there's a substantial risk of complications, including scarring and loss of mobility.
Surgical management
Major burns will require multiple surgical procedures over weeks to months depending on size of the burn and comorbidities. Major burns are at risk for infection until the burned areas are healed. The goal for large burn injuries is to undergo initial surgical excision within 48 hours of injury. Removal of the burned tissue decreases the risk of infection and allows for the preservation of viable tissue. 1 The wound bed is then usually covered in a temporary skin substitute called an allograft. This helps protect the wound bed and prepare it for a permanent autograft. Autograft will allow for healing of the burn injury. The sooner the skin closure is obtained, the better the outcome for the patient.
Allografts are temporary grafts that act as a skin substitute. This is often cadaver skin that's donated and sterilized. Because it's human skin, it provides an ideal environment for the wound bed to granulate and mature in order to receive an autograft. Allografts help maintain moisture that's lost through dressing application and prevent infection by providing a barrier. There are other types of allografts including porcine skin, also known as xenograft, and several types that use placental stem cells. 1
Autografts are grafts that originate from the patient's own skin. These include full- and split-thickness grafts. This graft type is permanent and is used primarily in full-thickness burn injuries or burns that have failed other treatment attempts. During an autografting procedure, the surgeon will remove a layer of healthy skin and place it over the burned area to provide skin for that area to heal. The area the skin is taken from, called the donor site, must then be cared for as a new wound. The donor site should heal in approximately 2 weeks. In large burns, there may be no place to obtain donor sites. In these cases, a biopsy is obtained, and the patients' own skin is grown in a lab. These are called cultured epithelial autografts and are used in a similar manner as the patient's own skin. 13
Quality care makes the difference
Patients with burn injuries are complex and have high mortality. Burns are traumatic injuries that cause profound shock within minutes and can affect every body system. Nurses must prioritize assessment of the airway, the cause of burn, depth, and TBSA during the initial screening. These assessments are important to appropriately resuscitate the patient and decrease the risk of burn shock. Patients with burns are at considerable risk for infection and hypothermia. Nurses should keep patients warm and transfer them to a certified burn center as soon as possible for the best outcomes. Providing early, quality nursing care to patients with burns will make all the difference in the outcome.
Parkland calculation example
A patient sustained a 55% burn. The patient weighs 72 kg.
(surface area) x (patient weight) x (mL)
55x72x4 = 15,840 mL
Total fluid required over first 24 hours
Total fluid required over first 8 hours (half total volume)
15,840/2 = 7,920 mL
Infusion rate (first 8 hours)
7,920/8 = 990 mL/h
Infusion rate (second 16 hours)
7,920/16 = 495 mL/h
Burn center referral criteria
* Second-degree burns (>10%)
* Burns to the genitals or perineum
* Burns to the face
* Burns to major joints
* Burns to hands or feet
* Third-degree burns
* Electrical burns
* Trauma where the burn injury poses the greater risk to the patient
* Patients with inhalation injuries
* Patients with preexisting medical conditions that could increase the risk of death
* Hospital doesn't have the capability to care for the burned patient
INSTRUCTIONS Nursing assessment and care of major burn injuries
Test instructions.
* Read the article. The test for this nursing continuing professional development (NCPD) activity is to be taken online at http://www.nursingcenter.com/CE .
* You'll need to create an account (it's free!) and log in to access My Planner before taking online tests. Your planner will keep track of all your Lippincott Professional Development online NCPD activities for you.
* There's only one correct answer for each question. A passing score for this test is 7 correct answers. If you pass, you can print your certificate of earned contact hours and access the answer key. If you fail, you have the option of taking the test again at no additional cost.
* For questions, contact Lippincott Professional Development: 1-800-787-8985.
* Registration deadline is December 5, 2025 .
PROVIDER ACCREDITATION
Lippincott Professional Development will award 1.5 contact hours for this nursing continuing professional development activity.
Lippincott Professional Development is accredited as a provider of nursing continuing professional development by the American Nurses Credentialing Center's Commission on Accreditation.
This activity is also provider approved by the California Board of Registered Nursing, Provider Number CEP 11749 for 1.5 contact hours. Lippincott Professional Development is also an approved provider of continuing nursing education by the District of Columbia, Georgia, West Virginia, New Mexico, South Carolina, and Florida, CE Broker #50-1223. Your certificate is valid in all states.
Payment: The registration fee for this test is $17.95.
1. Herndon DN. Total Burn Care . 5th ed. Edinburgh: Elsevier; 2017:19-222. [Context Link]
2. American Burn Association. Find a Burn Center. https://ameriburn.org/resources/find-a-burn-center . [Context Link]
3. Simko LC, Culleiton AL. Burn injuries in the ICU. Nurs Crit Care . 2017;12(2):12-22. [Context Link]
4. Osborn K. Nursing burn injuries. Nurs Manage . 2003;34(5):49-56. [Context Link]
5. Rose JJ, Wang L, Xu Q, et al Carbon monoxide poisoning: pathogenesis, management, and future directions of therapy. Am J Respir Crit Care Med . 2017;195(5):596-606. [Context Link]
6. Perel P, Roberts I, Ker K. Colloids versus crystalloids for fluid resuscitation in critically ill patients. Cochrane Database Syst Rev . 2013;(2):CD000567. [Context Link]
7. Kao Y, Loh E-W, Hsu C-C, et al Fluid resuscitation in patients with severe burns: a meta-analysis of randomized controlled trials. Acad Emerg Med . 2018;25(3):320-329. [Context Link]
8. Shah A, Pedraza I, Mitchell C, Kramer GC. Fluid volumes infused during burn resuscitation 1980-2015: a quantitative review. Burns . 2020;46(1):52-57. [Context Link]
9. Yeong E-K, O'Boyle CP, Huang H-F, et al Response of a local hospital to a burn disaster: contributory factors leading to zero mortality outcomes. Burns . 2018;44(5):1083-1090. [Context Link]
10. Culnan DM, Farner K, Bitz GH, et al Volume resuscitation in patients with high-voltage electrical injuries. Ann Plast Surg . 2018;80(3 suppl 2):S113-S118. [Context Link]
11. Devlin JW, Skrobik Y, Gelinas C, et al Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med . 2018;46(9):e825-e873. [Context Link]
12. Retrouvey H, Shahrokhi S. Pain and the thermally injured patient-a review of current therapies. J Burn Care Res . 2015;36(2):315-323. [Context Link]
13. Sood R, Roggy D, Zieger M, et al Cultured epithelial autografts for coverage of large burn wounds in eighty-eight patients: the Indiana University experience. J Burn Care Res . 2010;31(4):559-568. [Context Link]
CE Resources
- Account Login
- Search by Specialty
- Search by Category
- Recommended CE
- Licensure Renewals
Nursing Resources
- Career Articles
- Drug Updates
- Patient Education
About NursingCenter
- Advertise with us
- Evidence-Based Practice Network
- Contact Us / Help
Connect with NursingCenter
Connect with us on Facebook, Twitter, Linkedin, YouTube, Pinterest, and Instagram.
IMAGES
COMMENTS
Nursing Care Plans and Management. The nursing care planning goals for a patient with a burn injury include pain management, infection prevention, wound care, nutritional support, psychological support, and promoting mobility and rehabilitation. The overall goal is to provide comprehensive care that addresses the patient's physical, emotional ...
Burns NCLEX Review and Nursing Care Plans. Burns occur as a result of skin damage secondary to exposure to heat, chemicals, sunlight, electricity, or radiation. Most burns happen accidentally. Burns come in a variety of degrees. The depth of burn and the amount of skin affected are the two determinants of the extent or degree of burn.
Nursing Assessment for Burn Injury (First, Second, Third Degree) Assess the size, location, and depth of the burn to determine the severity of the injury and guide appropriate treatment interventions. Evaluate the patient's pain level using a pain scale to tailor pain management strategies effectively and ensure the patient's comfort.
The nursing care plan for burns begins with a thorough assessment to determine the extent and severity of the burn injury. This assessment serves as the foundation for developing individualized nursing diagnoses and interventions that guide the care provided to the patient. Wound care management is a fundamental aspect of the nursing care plan ...
Main Article: 11 Burn Injury Nursing Care Plans. To implement the plan of care for a burn injury patient effectively, there should be goals that should be set: Maintenance of adequate tissue oxygenation. Maintenance of patent airway and adequate airway clearance. Restoration of optimal fluid and electrolyte balance and perfusion of vital organs.
Description. Burns are caused by a transfer of energy from a heat source to the body. The depth of the injury depends on the temperature of the burning agent and the duration of contact with it. Burns disrupt the skin, which leads to increased fluid loss; infection; hypothermia; scarring; compromised immunity; and changes in function ...
Correct hypoxemia and acidosis from burn or inhalation; use a humidifier for comfort, to thin mucus and to prevent atelectasis. IV fluids, medications, and blood products may need to be infused quickly. If fluid resuscitation is required, utilize appropriate formula and assess for infiltration. Pain is usually present to some varying degree and ...
IV agents: An Anaesthetist and Anaesthetic technician are required; 2-3 nursing staff of which 1 is experienced in burns dressing and 1-2 nursing staff members to assist. All roles must be designated prior to commencement of dressing change and the patient should remain in line of sight to staff at all times.
Introduction. Burns are one type of injury to the skin caused by heat, electricity, chemicals, sunlight, or radiation. The main types of burns include thermal (heat/flame), electrical, chemical, and radiation. Nursing care plan for burns helps to ensure that the patient's wounds are adequately treated and monitored for infection.. Assessment. Severity: It is determined from the depth and ...
The first 48 hours are the most critical period in the care of patients with burns. Nursing priorities in the initial management of patients with burns include airway protection, fluid resuscitation, warming measures, and evaluation of the burned tissue. 1 Airway evaluation and protection are priorities for patients who may have sustained an ...
A burn plan helps to determine the safest and easiest way to complete tasks before, during and after a prescribed burn. The most important reason for having a burn plan is to thoroughly think about each action before striking the match. The burn plan will help determine where the burn should be conducted, what type of management is required ...
Burns Nursing Care Plan. There are a number of nursing diagnoses (both risk and actual problems) for burns that the nurse can identify based on assessment findings such as: Ineffective airway clearance. Impaired gas exchange. Impaired/Alteration in skin integrity. Risk for/Fluid volume deficit. Risk for Infection.
Large total body surface area burns require immediate and aggressive assessment and management from well-trained nurses in a variety of settings. Patients' responses to treatment need to be carefully and frequently monitored to prevent complication and improve survival. In 2016, more than 200,000 people in the United States were hospitalized ...
Pathophysiology of Burn Injury. An important concept to understand with burns is that in larger burns (generally around 30% TBSA), the body's response to the injury is not just localized to that area. There is a systemic response that increases in severity in proportion to the extent of the injury. Bigger burns mean your patient is "bigger ...
Step 1: Assessment. The first step in writing an organized care plan includes gathering subjective and objective nursing data. Subjective data is what the patient tells us their symptoms are, including feelings, perceptions, and concerns. Objective data is observable and measurable. This information can come from,
Writing the best nursing care plan requires a step-by-step approach to complete the parts needed for a care plan correctly. This tutorial will walk you through developing a care plan. This guide has the ultimate database and list of nursing care plans (NCP) and nursing diagnosis samples for our student nurses and professional nurses to use—all for free!
Stages of burn management. Care for a patient with burn injuries is organized into three stages: emergent (resuscitative), acute (wound healing), and rehabilitative (restorative). 9 The assessment and management of specific problems overlap and may span two or three stages.
Nursing the burn-injured patient and supporting his/her family throughout recovery is a complex and demanding but, ultimately rewarding, professional role. The repertoire of required nursing skills is varied and includes comprehensive critical care, complex wound care, pain and anxiety management, psychosocial support and community re-integration.
A variety of factors guide the evaluation and management of burns. First is the type of burn, such as thermal, chemical, electrical, or radiation. Second is the extent of the burn, usually expressed as the percentage of total body surface area (%TBSA) involved. Next is the depth of the burn described as superficial (first degree), partial (second degree) or full thickness (third degree ...
These outcomes and interventions are written as the nursing care plan and serve as a written guide for all health care professionals. An example of a written nursing care plan for the patient in the resuscitative and acute care phases of a major burn injury is provided in by Molter et.al and Ahrns-Klas.[8,9]
Nursing priorities in the initial management of patients with burns include airway protection, fluid resuscitation, warming measures, and evaluation of the burned tissue. 1 Airway evaluation and protection are priorities for patients who may have sustained an inhalation injury or burns to the airways. Patients involved in structure fires ...
PRESCRIBED FIRE BASICS. RESCRIBED FIRE BASICS:PLANNING A PRESCRIBED BURNburn plan is a written document that helps the burn. anager ensure a safe and efective prescribed burn. The burn plan's essential function is to identify burn objective. and provide procedures to accomplish them safely.pla.