Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Published: 22 February 2024

Attention-deficit/hyperactivity disorder
- Stephen V. Faraone ORCID: orcid.org/0000-0002-9217-3982 1 ,
- Mark A. Bellgrove ORCID: orcid.org/0000-0003-0186-8349 2 ,
- Isabell Brikell 3 , 4 , 5 ,
- Samuele Cortese 6 , 7 , 8 , 9 , 10 ,
- Catharina A. Hartman 11 ,
- Chris Hollis ORCID: orcid.org/0000-0003-1083-6744 12 ,
- Jeffrey H. Newcorn 13 ,
- Alexandra Philipsen ORCID: orcid.org/0000-0001-6876-518X 14 ,
- Guilherme V. Polanczyk ORCID: orcid.org/0000-0003-2311-3289 15 ,
- Katya Rubia 16 , 17 ,
- Margaret H. Sibley ORCID: orcid.org/0000-0001-7167-2240 18 &
- Jan K. Buitelaar ORCID: orcid.org/0000-0001-8288-7757 19 , 20
Nature Reviews Disease Primers volume 10 , Article number: 11 ( 2024 ) Cite this article
5928 Accesses
6 Citations
186 Altmetric
Metrics details
- Cognitive neuroscience
- Medical genetics
An Author Correction to this article was published on 15 April 2024
This article has been updated
Attention-deficit/hyperactivity disorder (ADHD; also known as hyperkinetic disorder) is a common neurodevelopmental condition that affects children and adults worldwide. ADHD has a predominantly genetic aetiology that involves common and rare genetic variants. Some environmental correlates of the disorder have been discovered but causation has been difficult to establish. The heterogeneity of the condition is evident in the diverse presentation of symptoms and levels of impairment, the numerous co-occurring mental and physical conditions, the various domains of neurocognitive impairment, and extensive minor structural and functional brain differences. The diagnosis of ADHD is reliable and valid when evaluated with standard diagnostic criteria. Curative treatments for ADHD do not exist but evidence-based treatments substantially reduce symptoms and/or functional impairment. Medications are effective for core symptoms and are usually well tolerated. Some non-pharmacological treatments are valuable, especially for improving adaptive functioning. Clinical and neurobiological research is ongoing and could lead to the creation of personalized diagnostic and therapeutic approaches for this disorder.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
24,99 € / 30 days
cancel any time
Subscribe to this journal
Receive 1 digital issues and online access to articles
92,52 € per year
only 92,52 € per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others

Polygenic profiles define aspects of clinical heterogeneity in attention deficit hyperactivity disorder

Machine learning in attention-deficit/hyperactivity disorder: new approaches toward understanding the neural mechanisms

Differences in the genetic architecture of common and rare variants in childhood, persistent and late-diagnosed attention-deficit hyperactivity disorder
Change history, 15 april 2024.
A Correction to this paper has been published: https://doi.org/10.1038/s41572-024-00518-w
Faraone, S. V. et al. Attention-deficit/hyperactivity disorder. Nat. Rev. Dis. Primers 1 , 15020 (2015).
Article PubMed Google Scholar
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders 5th edn (American Psychiatric Publishing, 2013).
World Health Organization. International classification of diseases 11th revision (WHO, 2022).
Faraone, S. V. et al. The World Federation of ADHD international consensus statement: 208 evidence-based conclusions about the disorder. Neurosci. Biobehav. Rev. 128 , 789–818 (2021).
Article PubMed PubMed Central Google Scholar
Polanczyk, G., de Lima, M. S., Horta, B. L., Biederman, J. & Rohde, L. A. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am. J. Psychiatry 164 , 942–948 (2007).
Polanczyk, G. V., Willcutt, E. G., Salum, G. A., Kieling, C. & Rohde, L. A. ADHD prevalence estimates across three decades: an updated systematic review and meta-regression analysis. Int. J. Epidemiol. 43 , 434–442 (2014).
Wootton, R. E. et al. Decline in attention-deficit hyperactivity disorder traits over the life course in the general population: trajectories across five population birth cohorts spanning ages 3 to 45 years. Int. J. Epidemiol. 51 , 919–930 (2022).
Faraone, S. V., Biederman, J. & Mick, E. The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol. Med. 36 , 159–165 (2006).
Simon, V., Czobor, P., Balint, S., Meszaros, A. & Bitter, I. Prevalence and correlates of adult attention-deficit hyperactivity disorder: meta-analysis. Br. J. Psychiatry 194 , 204–211 (2009).
Song, P. et al. The prevalence of adult attention-deficit hyperactivity disorder: a global systematic review and meta-analysis. J. Glob. Health 11 , 04009 (2021).
Vos, M. & Hartman, C. A. The decreasing prevalence of ADHD across the adult lifespan confirmed. J. Glob. Health 12 , 03024 (2022).
Solmi, M. et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol. Psychiatry 27 , 281–295 (2021).
Grevet, E. H. et al. The course of attention-deficit/hyperactivity disorder through midlife. Eur. Arch. Psychiatry Clin. Neurosci. 274 , 59–70 (2022).
Sibley, M. H. et al. Variable patterns of remission from ADHD in the multimodal treatment study of ADHD. Am. J. Psychiatry 179 , 142–151 (2022).
Vos, M. et al. Characterizing the heterogeneous course of inattention and hyperactivity-impulsivity from childhood to young adulthood. Eur. Child. Adolesc. Psychiatry 31 , 1–11 (2022).
Pedersen, S. L. et al. Real-world changes in adolescents’ ADHD symptoms within the day and across school and non-school days. J. Abnorm. Child. Psychol. 48 , 1543–1553 (2020).
Van Meter, A. R. et al. The stability and persistence of symptoms in childhood-onset ADHD. Eur. Child Adolesc. Psychiatry https://doi.org/10.1007/s00787-023-02235-3 (2023).
Halperin, J. M. & Marks, D. J. Practitioner review: assessment and treatment of preschool children with attention-deficit/hyperactivity disorder. J. Child. Psychol. Psychiatry 60 , 930–943 (2019).
MTA Cooperative Group. A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. The MTA Cooperative Group. Multimodal Treatment Study of Children with ADHD. Arch. Gen. Psychiatry 56 , 1073–1086 (1999).
Article Google Scholar
Staller, J. & Faraone, S. V. Attention-deficit hyperactivity disorder in girls: epidemiology and management. CNS Drugs 20 , 107–123 (2006).
Article CAS PubMed Google Scholar
Bruchmuller, K., Margraf, J. & Schneider, S. Is ADHD diagnosed in accord with diagnostic criteria? Overdiagnosis and influence of client gender on diagnosis. J. Consult. Clin. Psychol. 80 , 128–138 (2012).
Dalsgaard, S. et al. Incidence rates and cumulative incidences of the full spectrum of diagnosed mental disorders in childhood and adolescence. JAMA Psychiatry 77 , 155–164 (2020).
Solberg, B. S. et al. Gender differences in psychiatric comorbidity: a population-based study of 40 000 adults with attention deficit hyperactivity disorder. Acta Psychiatr. Scand. 137 , 176–186 (2018).
Libutzki, B. et al. Direct medical costs of ADHD and its comorbid conditions on basis of a claims data analysis. Eur. Psychiatry 58 , 38–44 (2019).
Chen, Q. et al. Common psychiatric and metabolic comorbidity of adult attention-deficit/hyperactivity disorder: a population-based cross-sectional study. PLoS ONE 13 , e0204516 (2018).
Sundquist, J., Ohlsson, H., Sundquist, K. & Kendler, K. S. Common adult psychiatric disorders in Swedish primary care where most mental health patients are treated. BMC Psychiatry 17 , 235 (2017).
Cortese, S., Faraone, S. V., Bernardi, S., Wang, S. & Blanco, C. Gender differences in adult attention-deficit/hyperactivity disorder: results from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). J. Clin. Psychiatry 77 , e421–e428 (2016).
Gaub, M. & Carlson, C. L. Gender differences in ADHD: a meta-analysis and critical review. J. Am. Acad. Child. Adolesc. Psychiatry 36 , 1036–1045 (1997).
Hinshaw, S. P., Nguyen, P. T., O’Grady, S. M. & Rosenthal, E. A. Annual research review: attention-deficit/hyperactivity disorder in girls and women: underrepresentation, longitudinal processes, and key directions. J. Child. Psychol. Psychiatry 63 , 484–496 (2022).
Young, S. et al. Females with ADHD: an expert consensus statement taking a lifespan approach providing guidance for the identification and treatment of attention-deficit/hyperactivity disorder in girls and women. BMC Psychiatry 20 , 404 (2020).
Harris, M. G. et al. Gender-related patterns and determinants of recent help-seeking for past-year affective, anxiety and substance use disorders: findings from a national epidemiological survey. Epidemiol. Psychiatr. Sci. 25 , 548–561 (2016).
Khoury, N. M., Radonjić, N. V., Albert, A. B. & Faraone, S. V. From structural disparities to neuropharmacology: a review of adult attention-deficit/hyperactivity disorder medication treatment. Child. Adolesc. Psychiatr. Clin. N. Am. 31 , 343–361 (2022).
Slobodin, O. & Masalha, R. Challenges in ADHD care for ethnic minority children: a review of the current literature. Transcult. Psychiatry 57 , 468–483 (2020).
Coker, T. R. et al. Racial and ethnic disparities in ADHD diagnosis and treatment. Pediatrics 138 , e20160407 (2016).
Miller, T. W., Nigg, J. T. & Miller, R. L. Attention deficit hyperactivity disorder in African American children: what can be concluded from the past ten years? Clin. Psychol. Rev. 29 , 77–86 (2009).
Morgan, P. L., Staff, J., Hillemeier, M. M., Farkas, G. & Maczuga, S. Racial and ethnic disparities in ADHD diagnosis from kindergarten to eighth grade. Pediatrics 132 , 85–93 (2013).
Morgan, P. L., Hillemeier, M. M., Farkas, G. & Maczuga, S. Racial/ethnic disparities in ADHD diagnosis by kindergarten entry. J. Child. Psychol. Psychiatry 55 , 905–913 (2014).
Stevens, J., Harman, J. S. & Kelleher, K. J. Race/ethnicity and insurance status as factors associated with ADHD treatment patterns. J. Child. Adolesc. Psychopharmacol. 15 , 88–96 (2005).
Shi, Y. et al. Racial disparities in diagnosis of attention-deficit/hyperactivity disorder in a US national birth cohort. JAMA Netw. Open. 4 , e210321 (2021).
Glasofer, A., Dingley, C. & Reyes, A. T. Medication decision making among African American caregivers of children with ADHD: a review of the literature. J. Atten. Disord. 25 , 1687–1698 (2021).
Fairman, K. A., Peckham, A. M. & Sclar, D. A. Diagnosis and treatment of ADHD in the United States: update by gender and race. J. Atten. Disord. 24 , 10–19 (2020).
Biederman, J., Newcorn, J. & Sprich, S. Comorbidity of attention deficit hyperactivity disorder with conduct, depressive, anxiety, and other disorders. Am. J. Psychiatry 148 , 564–577 (1991).
Hartman, C. A. et al. Anxiety, mood, and substance use disorders in adult men and women with and without attention-deficit/hyperactivity disorder: a substantive and methodological overview. Neurosci. Biobehav. Rev. 151 , 105209 (2023).
Dalsgaard, S., Ostergaard, S. D., Leckman, J. F., Mortensen, P. B. & Pedersen, M. G. Mortality in children, adolescents, and adults with attention deficit hyperactivity disorder: a nationwide cohort study. Lancet 385 , 2190–2196 (2015).
Elwin, M., Elvin, T. & Larsson, J. O. Symptoms and level of functioning related to comorbidity in children and adolescents with ADHD: a cross-sectional registry study. Child. Adolesc. Psychiatry Ment. Health 14 , 30 (2020).
Kessler, R. C., Chiu, W. T., Demler, O., Merikangas, K. R. & Walters, E. E. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 62 , 617–627 (2005).
Sun, S. et al. Association of psychiatric comorbidity with the risk of premature death among children and adults with attention-deficit/hyperactivity disorder. JAMA Psychiatry 76 , 1141–1149 (2019).
Kessler, R. C. et al. The effects of temporally secondary co-morbid mental disorders on the associations of DSM-IV ADHD with adverse outcomes in the US National Comorbidity Survey Replication Adolescent Supplement (NCS-A). Psychol. Med. 44 , 1779–1792 (2014).
Angold, A., Costello, J. & Erkanli, A. Comorbidity. J. Child. Psychol. Psychiat 40 , 57–87 (1999).
Biederman, J. et al. The longitudinal course of comorbid oppositional defiant disorder in girls with attention-deficit/hyperactivity disorder: findings from a controlled 5-year prospective longitudinal follow-up study. J. Dev. Behav. Pediatr. 29 , 501–507 (2008).
Biederman, J. et al. The long-term longitudinal course of oppositional defiant disorder and conduct disorder in ADHD boys: findings from a controlled 10-year prospective longitudinal follow-up study. Psychol. Med. 38 , 1027–1036 (2008).
Instanes, J. T., Klungsoyr, K., Halmoy, A., Fasmer, O. B. & Haavik, J. Adult ADHD and comorbid somatic disease: a systematic literature review. J. Atten. Disord. 22 , 203–228 (2016).
Kittel-Schneider, S. et al. Non-mental diseases associated with ADHD across the lifespan: Fidgety Philipp and Pippi Longstocking at risk of multimorbidity? Neurosci. Biobehav. Rev. 132 , 1157–1180 (2021).
Arrondo, G. et al. Associations between mental and physical conditions in children and adolescents: an umbrella review. Neurosci. Biobehav. Rev. 137 , 104662 (2022).
Garcia-Argibay, M. et al. The association between type 2 diabetes and attention- deficit/hyperactivity disorder: a systematic review, meta-analysis, and population-based sibling study. Neurosci. Biobehav. Rev. 147 , 105076 (2023).
Li, L. et al. Attention-deficit/hyperactivity disorder as a risk factor for cardiovascular diseases: a nationwide population-based cohort study. World Psychiatry 21 , 452–459 (2022).
Bellato, A. et al. Association between ADHD and vision problems. A systematic review and meta-analysis. Mol. Psychiatry 28 , 410–422 (2023).
Cortese, S., Faraone, S. V., Konofal, E. & Lecendreux, M. Sleep in children with attention-deficit/hyperactivity disorder: meta-analysis of subjective and objective studies. J. Am. Acad. Child. Adolesc. Psychiatry 48 , 894–908 (2009).
PubMed Google Scholar
Gidziela, A. et al. A meta-analysis of genetic effects associated with neurodevelopmental disorders and co-occurring conditions. Nat. Hum. Behav. 7 , 642–656 (2023).
Polderman, T. J. et al. Meta-analysis of the heritability of human traits based on fifty years of twin studies. Nat. Genet. 47 , 702–709 (2015).
Faraone, S. V. & Larsson, H. Genetics of attention deficit hyperactivity disorder. Mol. Psychiatry 24 , 562–575 (2018).
Brikell, I., Kuja-Halkola, R. & Larsson, H. Heritability of attention-deficit hyperactivity disorder in adults. Am. J. Med. Genet. B Neuropsychiatr. Genet. 168 , 406–413 (2015).
Nikolas, M. A. & Burt, S. A. Genetic and environmental influences on ADHD symptom dimensions of inattention and hyperactivity: a meta-analysis. J. Abnorm. Psychol. 119 , 1–17 (2010).
Taylor, M. J. et al. Association of genetic risk factors for psychiatric disorders and traits of these disorders in a Swedish population twin sample. JAMA Psychiatry 76 , 280–289 (2019).
Brikell, I., Burton, C., Mota, N. R. & Martin, J. Insights into attention-deficit/hyperactivity disorder from recent genetic studies. Psychol. Med. 51 , 2274–2286 (2021).
Tistarelli, N., Fagnani, C., Troianiello, M., Stazi, M. A. & Adriani, W. The nature and nurture of ADHD and its comorbidities: a narrative review on twin studies. Neurosci. Biobehav. Rev. 109 , 63–77 (2020).
Martin, J., Taylor, M. J. & Lichtenstein, P. Assessing the evidence for shared genetic risks across psychiatric disorders and traits. Psychol. Med. 48 , 1759–1774 (2018).
Andersson, A. et al. Research review: the strength of the genetic overlap between ADHD and other psychiatric symptoms – a systematic review and meta-analysis. J. Child. Psychol. Psychiatry 61 , 1173–1183 (2020).
Daucourt, M. C., Erbeli, F., Little, C. W., Haughbrook, R. & Hart, S. A. A meta-analytical review of the genetic and environmental correlations between reading and attention-deficit hyperactivity disorder symptoms and reading and math. Sci. Stud. Read. 24 , 23–56 (2020).
Du Rietz, E. et al. Mapping phenotypic and aetiological associations between ADHD and physical conditions in adulthood in Sweden: a genetically informed register study. Lancet Psychiatry 8 , 774–783 (2021).
Demontis, D. et al. Genome-wide analyses of ADHD identify 27 risk loci, refine the genetic architecture and implicate several cognitive domains. Nat. Genet. 55 , 198–208 (2023).
Article CAS PubMed PubMed Central Google Scholar
Martin, J. et al. A genetic investigation of sex bias in the prevalence of attention-deficit/hyperactivity disorder. Biol. Psychiatry 83 , 1044–1053 (2018).
Rajagopal, V. M. et al. Differences in the genetic architecture of common and rare variants in childhood, persistent and late-diagnosed attention-deficit hyperactivity disorder. Nat. Genet. 54 , 1117–1124 (2022).
Rovira, P. et al. Shared genetic background between children and adults with attention deficit/hyperactivity disorder. Neuropsychopharmacology 45 , 1617–1626 (2020).
Ronald, A., de Bode, N. & Polderman, T. J. C. Systematic review: how the attention-deficit/hyperactivity disorder polygenic risk score adds to our understanding of ADHD and associated traits. J. Am. Acad. Child. Adolesc. Psychiatry 60 , 1234–1277 (2021).
Leppert, B. et al. A cross-disorder PRS-pheWAS of 5 major psychiatric disorders in UK Biobank. PLoS Genet. 16 , e1008185 (2020).
Brikell, I. et al. Interplay of ADHD polygenic liability with birth-related, somatic, and psychosocial factors in ADHD: a nationwide study. Am. J. Psychiatry 180 , 73–88 (2023).
Barnett, E. J. et al. Identifying pediatric mood disorders from transdiagnostic polygenic risk scores: a study of children and adolescents. J. Clin. Psychiatry 83 , 21m14180 (2022).
Hamshere, M. L. et al. High loading of polygenic risk for ADHD in children with comorbid aggression. Am. J. Psychiatry 170 , 909–916 (2013).
Green, A., Baroud, E., DiSalvo, M., Faraone, S. V. & Biederman, J. Examining the impact of ADHD polygenic risk scores on ADHD and associated outcomes: a systematic review and meta-analysis. J. Psychiatr. Res. 155 , 49–67 (2022).
Moses, M. et al. Working memory and reaction time variability mediate the relationship between polygenic risk and ADHD traits in a general population sample. Mol. Psychiatry 27 , 5028–5037 (2022).
Vainieri, I. et al. Polygenic association between attention-deficit/hyperactivity disorder liability and cognitive impairments. Psychol. Med. 52 , 3150–3158 (2022).
Klein, M. et al. Genetic markers of ADHD-related variations in intracranial volume. Am. J. Psychiatry 176 , 228–238 (2019).
Hermosillo, R. J. M. et al. Polygenic risk score-derived subcortical connectivity mediates attention-deficit/hyperactivity disorder diagnosis. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 5 , 330–341 (2019).
PubMed PubMed Central Google Scholar
Satterstrom, F. K. et al. Autism spectrum disorder and attention deficit hyperactivity disorder have a similar burden of rare protein-truncating variants. Nat. Neurosci. 22 , 1961–1965 (2019).
Harich, B. et al. From rare copy number variants to biological processes in ADHD. Am. J. Psychiatry 177 , 855–866 (2020).
Gudmundsson, O. O. et al. Attention-deficit hyperactivity disorder shares copy number variant risk with schizophrenia and autism spectrum disorder. Transl. Psychiatry 9 , 258 (2019).
Calle Sánchez, X. et al. Comparing copy number variations in a Danish case cohort of individuals with psychiatric disorders. JAMA Psychiatry 79 , 59–69 (2022).
Boland, H. et al. A literature review and meta-analysis on the effects of ADHD medications on functional outcomes. J. Psychiatr. Res. 123 , 21–30 (2020).
Bonvicini, C., Faraone, S. V. & Scassellati, C. Attention-deficit hyperactivity disorder in adults: a systematic review and meta-analysis of genetic, pharmacogenetic and biochemical studies. Mol. Psychiatry 21 , 1643 (2016).
Adeyemo, B. O. et al. Mild traumatic brain injury and ADHD: a systematic review of the literature and meta-analysis. J. Atten. Disord. 18 , 576–584 (2014).
Asarnow, R. F., Newman, N., Weiss, R. E. & Su, E. Association of attention-deficit/hyperactivity disorder diagnoses with pediatric traumatic brain injury: a meta-analysis. JAMA Pediatr. 175 , 1009–1016 (2021).
Stevens, S. E. et al. Inattention/overactivity following early severe institutional deprivation: presentation and associations in early adolescence. J. Abnorm. Child. Psychol. 36 , 385–398 (2008).
Kim, J. H. et al. Environmental risk factors, protective factors, and peripheral biomarkers for ADHD: an umbrella review. Lancet Psychiatry 7 , 955–970 (2020).
Taubes, G. Epidemiology faces its limits. Science 269 , 164–169 (1995).
VanderWeele, T. J. & Ding, P. Sensitivity analysis in observational research: introducing the E-value. Ann. Intern. Med. 167 , 268–274 (2017).
Spencer, N. J. et al. Social gradients in ADHD by household income and maternal education exposure during early childhood: findings from birth cohort studies across six countries. PLoS ONE 17 , e0264709 (2022).
Schmengler, H. et al. Educational level, attention problems, and externalizing behaviour in adolescence and early adulthood: the role of social causation and health-related selection-the TRAILS study. Eur. Child Adolesc. Psychiatry 32 , 809–824 (2021).
Burt, S. A. Rethinking environmental contributions to child and adolescent psychopathology: a meta-analysis of shared environmental influences. Psychol. Bull. 135 , 608–637 (2009).
Marees, A. T. et al. Genetic correlates of socio-economic status influence the pattern of shared heritability across mental health traits. Nat. Hum. Behav. 5 , 1065–1073 (2021).
Kong, A. et al. The nature of nurture: effects of parental genotypes. Science 359 , 424–428 (2018).
Howe, L. J. et al. Within-sibship genome-wide association analyses decrease bias in estimates of direct genetic effects. Nat. Genet. 54 , 581–592 (2022).
Zwicker, A. et al. Neurodevelopmental and genetic determinants of exposure to adversity among youth at risk for mental illness. J. Child Psychol. Psychiatry 61 , 536–544 (2019).
de la Paz, L. et al. Youth polygenic scores, youth ADHD symptoms, and parenting dimensions: an evocative gene-environment correlation study. Res. Child Adolesc. Psychopathol. 51 , 665–677 (2023).
Havdahl, A. et al. Associations between pregnancy-related predisposing factors for offspring neurodevelopmental conditions and parental genetic liability to attention-deficit/hyperactivity disorder, autism, and schizophrenia: the Norwegian Mother, Father and Child Cohort Study (MoBa). JAMA Psychiatry 79 , 799–810 (2022).
Leppert, B. et al. Association of maternal neurodevelopmental risk alleles with early-life exposures. JAMA Psychiatry 76 , 834–842 (2019).
Thapar, A. & Rutter, M. Do prenatal risk factors cause psychiatric disorder? Be wary of causal claims. Br. J. Psychiatry 195 , 100–101 (2009).
Carlsson, T., Molander, F., Taylor, M. J., Jonsson, U. & Bölte, S. Early environmental risk factors for neurodevelopmental disorders – a systematic review of twin and sibling studies. Dev. Psychopathol. 195 , 1448–1495 (2020).
Google Scholar
He, Y., Chen, J., Zhu, L. H., Hua, L. L. & Ke, F. F. Maternal smoking during pregnancy and ADHD: results from a systematic review and meta-analysis of prospective cohort studies. J. Atten. Disord. 24 , 1637–1647 (2017).
Huang, L. et al. Maternal smoking and attention-deficit/hyperactivity disorder in offspring: a meta-analysis. Pediatrics 141 , e20172465 (2017).
Dong, T. et al. Prenatal exposure to maternal smoking during pregnancy and attention-deficit/hyperactivity disorder in offspring: a meta-analysis. Reprod. Toxicol. 76 , 63–70 (2018).
Ratanatharathorn, A., Chibnik, L. B., Koenen, K. C., Weisskopf, M. G. & Roberts, A. L. Association of maternal polygenic risk scores for mental illness with perinatal risk factors for offspring mental illness. Sci. Adv. 8 , eabn3740 (2022).
Thapar, A. et al. Prenatal smoking might not cause attention-deficit/hyperactivity disorder: evidence from a novel design. Biol. Psychiatry 66 , 722–727 (2009).
Faraone, S. V. & Biederman, J. Can attention-deficit/hyperactivity disorder onset occur in adulthood? JAMA Psychiatry 73 , 655–656 (2016).
Dvorsky, M. R. & Langberg, J. M. A review of factors that promote resilience in youth with ADHD and ADHD symptoms. Clin. Child. Fam. Psychol. Rev. 19 , 368–391 (2016).
Barry, R. J., Johnstone, S. J. & Clarke, A. R. A review of electrophysiology in attention-deficit/hyperactivity disorder: II. Event-related potentials. Clin. Neurophysiol. 114 , 184–198 (2003).
Barry, R. J., Clarke, A. R. & Johnstone, S. J. A review of electrophysiology in attention-deficit/hyperactivity disorder: I. Qualitative and quantitative electroencephalography. Clin. Neurophysiol. 114 , 171–183 (2003).
Kaiser, A. et al. Earlier versus later cognitive event-related potentials (ERPs) in attention-deficit/hyperactivity disorder (ADHD): a meta-analysis. Neurosci. Biobehav. Rev. 112 , 117–134 (2020).
Hoogman, M. et al. Brain imaging of the cortex in ADHD: a coordinated analysis of large-scale clinical and population-based samples. Am. J. Psychiatry 176 , 531–542 (2019).
Hoogman, M. et al. Subcortical brain volume differences in participants with attention deficit hyperactivity disorder in children and adults: a cross-sectional mega-analysis. Lancet Psychiatry 4 , 310–319 (2017).
Albaugh, M. D. et al. White matter microstructure is associated with hyperactive/inattentive symptomatology and polygenic risk for attention-deficit/hyperactivity disorder in a population-based sample of adolescents. Neuropsychopharmacology 44 , 1597–1603 (2019).
Clarke, A. R., Barry, R. J. & Johnstone, S. Resting state EEG power research in attention-deficit/hyperactivity disorder: a review update. Clin. Neurophysiol. 131 , 1463–1479 (2020).
Bussalb, A. et al. Is there a cluster of high theta-beta ratio patients in attention deficit hyperactivity disorder? Clin. Neurophysiol. 130 , 1387–1396 (2019).
Slater, J. et al. Can electroencephalography (EEG) identify ADHD subtypes? A systematic review. Neurosci. Biobehav. Rev. 139 , 104752 (2022).
Parlatini, V. et al. Network abnormalities in attention-deficit/hyperactivity disorder (ADHD): a systematic review of 127 diffusion imaging studies with meta-analysis. Mol. Psychiatry 28 , 4098–4123 (2023).
Sudre, G. et al. Mapping the cortico-striatal transcriptome in attention deficit hyperactivity disorder. Mol. Psychiatry 28 , 792–800 (2023).
Hart, H., Radua, J., Nakao, T., Mataix-Cols, D. & Rubia, K. Meta-analysis of functional magnetic resonance imaging studies of inhibition and attention in attention-deficit/hyperactivity disorder: exploring task-specific, stimulant medication, and age effects. JAMA Psychiatry 70 , 185–198 (2013).
Norman, L. J. et al. Structural and functional brain abnormalities in attention-deficit/hyperactivity disorder and obsessive-compulsive disorder: a comparative meta-analysis. JAMA Psychiatry 73 , 815–825 (2016).
Lukito, S. et al. Comparative meta-analyses of brain structural and functional abnormalities during cognitive control in attention-deficit/hyperactivity disorder and autism spectrum disorder. Psychol. Med. 50 , 894–919 (2020).
Samea, F. et al. Brain alterations in children/adolescents with ADHD revisited: a neuroimaging meta-analysis of 96 structural and functional studies. Neurosci. Biobehav. Rev. 100 , 1–8 (2019).
McCarthy, H., Skokauskas, N. & Frodl, T. Identifying a consistent pattern of neural function in attention deficit hyperactivity disorder: a meta-analysis. Psychol. Med. 44 , 869–880 (2014).
Sonuga-Barke, E. J. & Castellanos, F. X. Spontaneous attentional fluctuations in impaired states and pathological conditions: a neurobiological hypothesis. Neurosci. Biobehav. Rev. 31 , 977–986 (2007).
Gao, Y. et al. Impairments of large-scale functional networks in attention-deficit/hyperactivity disorder: a meta-analysis of resting-state functional connectivity. Psychol. Med. 49 , 2475–2485 (2019).
Sutcubasi, B. et al. Resting-state network dysconnectivity in ADHD: a system-neuroscience-based meta-analysis. World J. Biol. Psychiatry 21 , 662–672 (2020).
Norman, L. J., Sudre, G., Price, J., Shastri, G. G. & Shaw, P. Evidence from “big data” for the default-mode hypothesis of ADHD: a mega-analysis of multiple large samples. Neuropsychopharmacology 48 , 281–289 (2023).
Cortese, S., Aoki, Y. Y., Itahashi, T., Castellanos, F. X. & Eickhoff, S. B. Systematic review and meta-analysis: resting state functional magnetic resonance imaging studies of attention-deficit/hyperactivity disorder. J. Am. Acad. Child. Adolesc. Psychiatry 60 , 61–75 (2021).
Shaw, P. et al. Attention-deficit/hyperactivity disorder is characterized by a delay in cortical maturation. Proc. Natl Acad. Sci. USA 104 , 19649–19654 (2007).
Shaw, P. et al. Development of cortical surface area and gyrification in attention-deficit/hyperactivity disorder. Biol. Psychiatry 72 , 191–197 (2012).
Shaw, P. et al. A multicohort, longitudinal study of cerebellar development in attention deficit hyperactivity disorder. J. Child. Psychol. Psychiatry 59 , 1114–1123 (2018).
Sripada, C. S., Kessler, D. & Angstadt, M. Lag in maturation of the brain’s intrinsic functional architecture in attention-deficit/hyperactivity disorder. Proc. Natl Acad. Sci. USA 111 , 14259–14264 (2014).
Norman, L. J., Sudre, G., Bouyssi-Kobar, M., Sharp, W. & Shaw, P. An examination of the relationships between attention/deficit hyperactivity disorder symptoms and functional connectivity over time. Neuropsychopharmacology 47 , 704–710 (2022).
Faraone, S. V. The pharmacology of amphetamine and methylphenidate: relevance to the neurobiology of attention-deficit/hyperactivity disorder and other psychiatric comorbidities. Neurosci. Biobehav. Rev. 87 , 255–270 (2018).
Radonjić, N. V., Bellato, A., Khoury, N. M., Cortese, S. & Faraone, S. V. Nonstimulant medications for attention-deficit/hyperactivity disorder (ADHD) in adults: systematic review and meta-analysis. CNS Drugs 37 , 381–397 (2023).
Pretus, C. et al. Time and psychostimulants: opposing long-term structural effects in the adult ADHD brain. A longitudinal MR study. Eur. Neuropsychopharmacol. 27 , 1238–1247 (2017).
Walhovd, K. B. et al. Methylphenidate effects on cortical thickness in children and adults with attention-deficit/hyperactivity disorder: a randomized clinical trial. AJNR Am. J. Neuroradiol. 41 , 758–765 (2020).
Bouziane, C. et al. White matter by diffusion MRI following methylphenidate treatment: a randomized control trial in males with attention-deficit/hyperactivity disorder. Radiology 293 , 186–192 (2019).
Greven, C. U. et al. Developmentally stable whole-brain volume reductions and developmentally sensitive caudate and putamen volume alterations in those with attention-deficit/hyperactivity disorder and their unaffected siblings. JAMA Psychiatry 72 , 490–499 (2015).
Schweren, L. J. et al. Thinner medial temporal cortex in adolescents with attention-deficit/hyperactivity disorder and the effects of stimulants. J. Am. Acad. Child. Adolesc. Psychiatry 54 , 660–667 (2015).
Fotopoulos, N. H. et al. Cumulative exposure to ADHD medication is inversely related to hippocampus subregional volume in children. Neuroimage Clin. 31 , 102695 (2021).
Rubia, K. et al. Effects of stimulants on brain function in attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. Biol. Psychiatry 76 , 616–628 (2014).
Faraone, S. V. et al. Practitioner review: emotional dysregulation in attention-deficit/hyperactivity disorder – implications for clinical recognition and intervention. J. Child. Psychol. Psychiatry 60 , 133–150 (2019).
Scassellati, C., Bonvicini, C., Faraone, S. V. & Gennarelli, M. Biomarkers and attention-deficit/hyperactivity disorder: a systematic review and meta-analyses. J. Am. Acad. Child. Adolesc. Psychiatry 51 , 1003–1019.e20 (2012).
Bellato, A. et al. Practitioner review: clinical utility of the QbTest for the assessment and diagnosis of attention-deficit/hyperactivity disorder – a systematic review and meta-analysis. J. Child Psychol. Psychiatry https://doi.org/10.1111/jcpp.13901 (2023).
Stein, M. A., Snyder, S. M., Rugino, T. A. & Hornig, M. Commentary: objective aids for the assessment of ADHD – further clarification of what FDA approval for marketing means and why NEBA might help clinicians. A response to Arns et al. (2016). J. Child. Psychol. Psychiatry 57 , 770–771 (2016).
Lee, S. et al. Can neurocognitive outcomes assist measurement-based care for children with attention-deficit/hyperactivity disorder? A systematic review and meta-analyses of the relationships among the changes in neurocognitive functions and clinical outcomes of attention-deficit/hyperactivity disorder in pharmacological and cognitive training interventions. J. Child. Adolesc. Psychopharmacol. 32 , 250–277 (2022).
Gordon, M. et al. Symptoms versus impairment: the case for respecting DSM-IV’s Criterion D. J. Atten. Disord. 9 , 465–475 (2006).
Sibley, M. H. et al. Late-onset ADHD reconsidered with comprehensive repeated assessments between ages 10 and 25. Am. J. Psychiatry 175 , 140–149 (2018).
Mulraney, M. et al. Systematic review and meta-analysis: screening tools for attention-deficit/hyperactivity disorder in children and adolescents. J. Am. Acad. Child. Adolesc. Psychiatry 61 , 982–996 (2022).
Coghill, D. et al. The management of ADHD in children and adolescents: bringing evidence to the clinic: perspective from the European ADHD Guidelines Group (EAGG). Eur. Child Adolesc. Psychiatry 32 , 1337–1361 (2021).
Fischer, M., Barkley, R., Fletcher, K. & Smallish, L. The stability of dimensions of behavior in ADHD and normal children over an 8-year followup. J. Abnorm. Child. Psychol. 21 , 315–337 (1993).
Evans, S. W., Allen, J., Moore, S. & Strauss, V. Measuring symptoms and functioning of youth with ADHD in middle schools. J. Abnorm. Child. Psychol. 33 , 695–706 (2005).
Chan, E., Fogler, J. M. & Hammerness, P. G. Treatment of attention-deficit/hyperactivity disorder in adolescents: a systematic review. JAMA 315 , 1997–2008 (2016).
Brinkman, W. B., Simon, J. O. & Epstein, J. N. Reasons why children and adolescents with attention-deficit/hyperactivity disorder stop and restart taking medicine. Acad. Pediatr. 18 , 273–280 (2018).
Sibley, M. H. et al. Defining ADHD symptom persistence in adulthood: optimizing sensitivity and specificity. J. Child. Psychol. Psychiatry 58 , 655–662 (2017).
Biederman, J. & Spencer, T. J. Psychopharmacological interventions. Child. Adolesc. Psychiatr. Clin. N. Am. 17 , 439–458 (2008).
Biederman, J., Spencer, T. & Wilens, T. in Essentials of Child and Adolescent Psychiatry (eds Wiener, J. M. & Dulcan, M.) 635–699 (American Psychiatric Publishing, 2006).
Cooper, M. et al. Investigating late-onset ADHD: a population cohort investigation. J. Child Psychol. Psychiatry 59 , 1105–1113 (2018).
Mitchell, J. T. et al. A qualitative analysis of contextual factors relevant to suspected late-onset ADHD. J. Atten. Disord. 25 , 724–735 (2021).
Waltereit, R., Ehrlich, S. & Roessner, V. First-time diagnosis of ADHD in adults: challenge to retrospectively assess childhood symptoms of ADHD from long-term memory. Eur. Child. Adolesc. Psychiatry 32 , 1333–1335 (2023).
Faraone, S. V. et al. Systematic review: nonmedical use of prescription stimulants: risk factors, outcomes, and risk reduction strategies. J. Am. Acad. Child. Adolesc. Psychiatry 59 , 100–112 (2020).
Yeung, A., Ng, E. & Abi-Jaoude, E. TikTok and attention-deficit/hyperactivity disorder: a cross-sectional study of social media content quality. Can. J. Psychiatry 67 , 899–906 (2022).
Rommelse, N. et al. An evidenced-based perspective on the validity of attention-deficit/hyperactivity disorder in the context of high intelligence. Neurosci. Biobehav. Rev. 71 , 21–47 (2016).
National Institute for Health and Care Excellence. Attention deficit hyperactivity disorder: diagnosis and management. NICE guideline NG87. NICE https://www.nice.org.uk/guidance/ng87/resources/attention-deficit-hyperactivity-disorder-diagnosis-and-management-pdf-1837699732933 (2019).
Wolraich, M. L. et al. Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics 144 , e20192528 (2019).
Sugaya, L. S., Farhat, L. C., Califano, P. & Polanczyk, G. V. Efficacy of stimulants for preschool attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. JCPP Adv. 3 , e12146 (2023).
Cortese, S. Pharmacologic treatment of attention deficit-hyperactivity disorder. N. Engl. J. Med. 383 , 1050–1056 (2020).
Poitras, V. & McCormack, S. Guanfacine hydrochloride extended-release for the treatment of attention deficit hyperactivity disorder in adults: a review of clinical effectiveness, cost-effectiveness, and guidelines (Canadian Agency for Drugs and Technologies in Health, 2018).
Iwanami, A., Saito, K., Fujiwara, M., Okutsu, D. & Ichikawa, H. Efficacy and safety of guanfacine extended-release in the treatment of attention-deficit/hyperactivity disorder in adults: results of a randomized, double-blind, placebo-controlled study. J. Clin. Psychiatry 81 , 19m12979 (2020).
Cortese, S. et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis. Lancet Psychiatry 5 , 727–738 (2018).
O’Connor, L., Carbone, S., Gobbo, A., Gamble, H. & Faraone, S. V. Pediatric attention deficit hyperactivity disorder (ADHD): 2022 updates on pharmacological management. Expert. Rev. Clin. Pharmacol. 16 , 799–812 (2023).
Faraone, S. V., McBurnett, K., Sallee, F. R., Steeber, J. & Lopez, F. A. Guanfacine extended release: a novel treatment for attention-deficit/hyperactivity disorder in children and adolescents. Clin. Ther. 35 , 1778–1793 (2013).
Childress, A. C. & Sallee, F. R. Revisiting clonidine: an innovative add-on option for attention-deficit/hyperactivity disorder. Drugs Today 48 , 207–217 (2012).
Article CAS Google Scholar
Buitelaar, J. et al. Toward precision medicine in ADHD. Front. Behav. Neurosci. 16 , 900981 (2022).
Faraone, S. V. et al. Early response to SPN-812 (viloxazine extended-release) can predict efficacy outcome in pediatric subjects with ADHD: a machine learning post-hoc analysis of four randomized clinical trials. Psychiatry Res. 296 , 113664 (2021).
Faraone, S. V. et al. Predicting efficacy of viloxazine extended-release treatment in adults with ADHD using an early change in ADHD symptoms: machine learning post hoc analysis of a phase 3 clinical trial. Psychiatry Res. 318 , 114922 (2022).
Newcorn, J. H., Sutton, V. K., Weiss, M. D. & Sumner, C. R. Clinical responses to atomoxetine in attention-deficit/hyperactivity disorder: the Integrated Data Exploratory Analysis (IDEA) study. J. Am. Acad. Child. Adolesc. Psychiatry 48 , 511–518 (2009).
Zhang, L. et al. Attention-deficit/hyperactivity disorder medications and long-term risk of cardiovascular diseases. JAMA Psychiatry https://doi.org/10.1001/jamapsychiatry.2023.4294 (2023).
Cortese, S. et al. Practitioner review: current best practice in the management of adverse events during treatment with ADHD medications in children and adolescents. J. Child. Psychol. Psychiatry 54 , 227–246 (2013).
Bloch, M. H., Panza, K. E., Landeros-Weisenberger, A. & Leckman, J. F. Meta-analysis: treatment of attention-deficit/hyperactivity disorder in children with comorbid tic disorders. J. Am. Acad. Child. Adolesc. Psychiatry 48 , 884–893 (2009).
van de Loo-Neus, G. H., Rommelse, N. & Buitelaar, J. K. To stop or not to stop? How long should medication treatment of attention-deficit hyperactivity disorder be extended? Eur. Neuropsychopharmacol. 21 , 584–599 (2011).
Faraone, S. V., Biederman, J., Morley, C. P. & Spencer, T. J. Effect of stimulants on height and weight: a review of the literature. J. Am. Acad. Child. Adolesc. Psychiatry 47 , 994–1009 (2008).
Biederman, J. et al. Growth trajectories in stimulant-treated children ages 6 to 12: an electronic medical record analysis. J. Dev. Behav. Pediatr. 44 , e80–e87 (2023).
Li, L. et al. Associations of prescribed ADHD medication in pregnancy with pregnancy-related and offspring outcomes: a systematic review. CNS Drugs 34 , 731–747 (2020).
Bang Madsen, K. et al. In utero exposure to ADHD medication and long-term offspring outcomes. Mol. Psychiatry 28 , 1739–1746 (2023).
Sonuga-Barke, E. J. et al. Nonpharmacological interventions for ADHD: systematic review and meta-analyses of randomized controlled trials of dietary and psychological treatments. Am. J. Psychiatry 170 , 275–289 (2013).
Faraone, S. V. & Antshel, K. M. Towards an evidence-based taxonomy of nonpharmacologic treatments for ADHD. Child. Adolesc. Psychiatr. Clin. N. Am. 23 , 965–972 (2014).
Sibley, M. H. et al. Non-pharmacological interventions for attention-deficit hyperactivity disorder in children and adolescents. Lancet Child Adolesc. Health 7 , 415–428 (2023).
Langberg, J. M., Epstein, J. N., Becker, S. P., Girio-Herrera, E. & Vaughn, A. J. Evaluation of the homework, organization, and planning skills (HOPS) intervention for middle school students with ADHD as implemented by school mental health providers. Sch. Psych. Rev. 41 , 342–364 (2012).
Sibley, M. H. et al. Parent-teen behavior therapy + motivational interviewing for adolescents with ADHD. J. Consult. Clin. Psychol. 84 , 699–712 (2016).
Groenman, A. P. et al. An individual participant data meta-analysis: behavioral treatments for children and adolescents with attention-deficit/hyperactivity disorder. J. Am. Acad. Child. Adolesc. Psychiatry 61 , 144–158 (2022).
Dekkers, T. J. et al. Meta-analysis: which components of parent training work for children with attention-deficit/hyperactivity disorder? J. Am. Acad. Child. Adolesc. Psychiatry 61 , 478–494 (2022).
Nimmo-Smith, V. et al. Non-pharmacological interventions for adult ADHD: a systematic review. Psychol. Med. 50 , 529–541 (2020).
Safren, S. A. et al. Cognitive-behavioral therapy for ADHD in medication-treated adults with continued symptoms. Behav. Res. Ther. 43 , 831–842 (2005).
Young, S. et al. A randomized controlled trial reporting functional outcomes of cognitive-behavioural therapy in medication-treated adults with ADHD and comorbid psychopathology. Eur. Arch. Psychiatry Clin. Neurosci. 267 , 267–276 (2017).
Tourjman, V. et al. Psychosocial interventions for attention deficit/hyperactivity disorder: a systematic review and meta-analysis by the CADDRA guidelines work group. Brain Sci. 12 , 1023 (2022).
Pan, M. R. et al. Efficacy of cognitive behavioural therapy in medicated adults with attention-deficit/hyperactivity disorder in multiple dimensions: a randomised controlled trial. Eur. Arch. Psychiatry Clin. Neurosci. 272 , 235–255 (2022).
Lopez-Pinar, C., Martinez-Sanchis, S., Carbonell-Vaya, E., Sanchez-Meca, J. & Fenollar-Cortes, J. Efficacy of nonpharmacological treatments on comorbid internalizing symptoms of adults with attention-deficit/hyperactivity disorder: a meta-analytic review. J. Atten. Disord. 24 , 456–478 (2020).
Liu, C. I., Hua, M. H., Lu, M. L. & Goh, K. K. Effectiveness of cognitive behavioural-based interventions for adults with attention-deficit/hyperactivity disorder extends beyond core symptoms: a meta-analysis of randomized controlled trials. Psychol. Psychother. 96 , 543–559 (2023).
Lopez-Pinar, C., Martinez-Sanchis, S., Carbonell-Vaya, E., Fenollar-Cortes, J. & Sanchez-Meca, J. Long-term efficacy of psychosocial treatments for adults with attention-deficit/hyperactivity disorder: a meta-analytic review. Front. Psychol. 9 , 638 (2018).
Hirvikoski, T. et al. Psychoeducational groups for adults with ADHD and their significant others (PEGASUS): a pragmatic multicenter and randomized controlled trial. Eur. Psychiatry 44 , 141–152 (2017).
Groß, V. et al. Effectiveness of psychotherapy in adult ADHD: what do patients think? Results of the COMPAS study. J. Atten. Disord. 23 , 1047–1058 (2019).
Philipsen, A. et al. Effects of group psychotherapy, individual counseling, methylphenidate, and placebo in the treatment of adult attention-deficit/hyperactivity disorder: a randomized clinical trial. JAMA Psychiatry 72 , 1199–1210 (2015).
Young, Z., Moghaddam, N. & Tickle, A. The efficacy of cognitive behavioral therapy for adults with ADHD: a systematic review and meta-analysis of randomized controlled trials. J. Atten. Disord. 24 , 875–888 (2020).
Oliva, F. et al. The efficacy of mindfulness-based interventions in attention-deficit/hyperactivity disorder beyond core symptoms: a systematic review, meta-analysis, and meta-regression. J. Affect. Disord. 292 , 475–486 (2021).
Schippers, L. M. et al. A qualitative and quantitative study of self-reported positive characteristics of individuals with ADHD. Front. Psychiatry 13 , 922788 (2022).
Salvat, H. et al. Nutrient intake, dietary patterns, and anthropometric variables of children with ADHD in comparison to healthy controls: a case-control study. BMC Pediatr. 22 , 70 (2022).
Ryu, S. A. et al. Associations between dietary intake and attention deficit hyperactivity disorder (ADHD) scores by repeated measurements in school-age children. Nutrients 14 , 2919 (2022).
Chang, J. P., Su, K. P., Mondelli, V. & Pariante, C. M. Omega-3 polyunsaturated fatty acids in youths with attention deficit hyperactivity disorder: a systematic review and meta-analysis of clinical trials and biological studies. Neuropsychopharmacology 43 , 534–545 (2018).
Hunjan, A. K., Hübel, C., Lin, Y., Eley, T. C. & Breen, G. Association between polygenic propensity for psychiatric disorders and nutrient intake. Commun. Biol. 4 , 965 (2021).
Bloch, M. H. & Qawasmi, A. Omega-3 fatty acid supplementation for the treatment of children with attention-deficit/hyperactivity disorder symptomatology: systematic review and meta-analysis. J. Am. Acad. Child. Adolesc. Psychiatry 50 , 991–1000 (2011).
Johnstone, J. M., Hughes, A., Goldenberg, J. Z., Romijn, A. R. & Rucklidge, J. J. Multinutrients for the treatment of psychiatric symptoms in clinical samples: a systematic review and meta-analysis of randomized controlled trials. Nutrients 12 , 3394 (2020).
Nigg, J. T., Lewis, K., Edinger, T. & Falk, M. Meta-analysis of attention-deficit/hyperactivity disorder or attention-deficit/hyperactivity disorder symptoms, restriction diet, and synthetic food color additives. J. Am. Acad. Child. Adolesc. Psychiatry 51 , 86–97.e8 (2012).
San Mauro Martin, I. et al. Impulsiveness in children with attention-deficit/hyperactivity disorder after an 8-week intervention with the Mediterranean diet and/or omega-3 fatty acids: a randomised clinical trial. Neurologia 37 , 513–523 (2022).
Khoshbakht, Y., Moghtaderi, F., Bidaki, R., Hosseinzadeh, M. & Salehi-Abargouei, A. The effect of dietary approaches to stop hypertension (DASH) diet on attention-deficit hyperactivity disorder (ADHD) symptoms: a randomized controlled clinical trial. Eur. J. Nutr. 60 , 3647–3658 (2021).
Huberts-Bosch, A. et al. Short-term effects of an elimination diet and healthy diet in children with attention-deficit/hyperactivity disorder: a randomized controlled trial. Eur. Child Adolesc. Psychiatry https://doi.org/10.1007/s00787-023-02256-y (2023).
Rubia, K., Westwood, S., Aggensteiner, P. M. & Brandeis, D. Neurotherapeutics for attention deficit/hyperactivity disorder (ADHD): a review. Cells 10 , 2156 (2021).
Purper-Ouakil, D. et al. Personalized at-home neurofeedback compared to long-acting methylphenidate in children with ADHD: NEWROFEED, a European randomized noninferiority trial. J. Child. Psychol. Psychiatry 63 , 187–198 (2022).
Riesco-Matias, P., Yela-Bernabe, J. R., Crego, A. & Sanchez-Zaballos, E. What do meta-analyses have to say about the efficacy of neurofeedback applied to children with ADHD? Review of previous meta-analyses and a new meta-analysis. J. Atten. Disord. 25 , 473–485 (2021).
Cortese, S. et al. Neurofeedback for attention-deficit/hyperactivity disorder: meta-analysis of clinical and neuropsychological outcomes from randomized controlled trials. J. Am. Acad. Child. Adolesc. Psychiatry 55 , 444–455 (2016).
Bussalb, A. et al. Clinical and experimental factors influencing the efficacy of neurofeedback in ADHD: a meta-analysis. Front. Psychiatry 10 , 35 (2019).
Neurofeedback Collaborative Group Double-blind placebo-controlled randomized clinical trial of neurofeedback for attention-deficit/hyperactivity disorder with 13-month follow-up. J. Am. Acad. Child. Adolesc. Psychiatry 60 , 841–855 (2021).
Alegria, A. A. et al. Real-time fMRI neurofeedback in adolescents with attention deficit hyperactivity disorder. Hum. Brain Mapp. 38 , 3190–3209 (2017).
Lam, S. L. et al. Double-blind, sham-controlled randomized trial testing the efficacy of fMRI neurofeedback on clinical and cognitive measures in children with ADHD. Am. J. Psychiatry 179 , 947–958 (2022).
Criaud, M. et al. Increased left inferior fronto-striatal activation during error monitoring after fMRI neurofeedback of right inferior frontal cortex in adolescents with attention deficit hyperactivity disorder. Neuroimage Clin. 27 , 102311 (2020).
Rubia, K. et al. Functional connectivity changes associated with fMRI neurofeedback of right inferior frontal cortex in adolescents with ADHD. Neuroimage 188 , 43–58 (2019).
Westwood, S. J., Radua, J. & Rubia, K. Noninvasive brain stimulation in children and adults with attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. J. Psychiatry Neurosci. 46 , E14–E33 (2021).
Hyde, J. et al. Efficacy of neurostimulation across mental disorders: systematic review and meta-analysis of 208 randomized controlled trials. Mol. Psychiatry 27 , 2709–2719 (2022).
Alyagon, U. et al. Alleviation of ADHD symptoms by non-invasive right prefrontal stimulation is correlated with EEG activity. Neuroimage Clin. 26 , 102206 (2020).
Westwood, S. J. et al. Transcranial direct current stimulation (tDCS) combined with cognitive training in adolescent boys with ADHD: a double-blind, randomised, sham-controlled trial. Psychol. Med. 53 , 497–512 (2023).
Leffa, D. T. et al. Transcranial direct current stimulation vs sham for the treatment of inattention in adults with attention-deficit/hyperactivity disorder: the TUNED randomized clinical trial. JAMA Psychiatry 79 , 847–856 (2022).
McGough, J. J. et al. Double-blind, sham-controlled, pilot study of trigeminal nerve stimulation for attention-deficit/hyperactivity disorder. J. Am. Acad. Child. Adolesc. Psychiatry 58 , 403–411.e3 (2019).
Denyer, H. et al. ADHD Remote Technology study of cardiometabolic risk factors and medication adherence (ART-CARMA): a multi-centre prospective cohort study protocol. BMC Psychiatry 22 , 813 (2022).
Hollis, C. et al. Annual research review: digital health interventions for children and young people with mental health problems – a systematic and meta-review. J. Child. Psychol. Psychiatry 58 , 474–503 (2017).
Kollins, S. H. et al. A novel digital intervention for actively reducing severity of paediatric ADHD (STARS-ADHD): a randomised controlled trial. Lancet Digital Health 2 , e168–e178 (2020).
Singh, L. J., Gaye, F., Cole, A. M., Chan, E. S. M. & Kofler, M. J. Central executive training for ADHD: effects on academic achievement, productivity, and success in the classroom. Neuropsychology 36 , 330–345 (2022).
Kofler, M. J. et al. A randomized controlled trial of central executive training (CET) versus inhibitory control training (ICT) for ADHD. J. Consult. Clin. Psychol. 88 , 738–756 (2020).
Westwood, S. J., Cortese, S., Rubia, K. & Sonuga-Barke, E. Computerised cognitive training for attention-deficit/hyperactivity disorder (ADHD): a European ADHD Guidelines Group (EAGG) systematic review and meta-analysis of randomised controlled trials with blinded and objective outcomes. Mol. Psychiatry 28 , 1402–1414 (2023).
Wehmeier, P. M., Schacht, A. & Barkley, R. A. Social and emotional impairment in children and adolescents with ADHD and the impact on quality of life. J. Adolesc. Health 46 , 209–217 (2010).
Dona, S. W. A. et al. The impact of childhood attention-deficit/hyperactivity disorder (ADHD) on children’s health-related quality of life: a systematic review and meta-analysis. J. Atten. Disord. 27 , 598–611 (2023).
Jans, T. et al. Does intensive multimodal treatment for maternal ADHD improve the efficacy of parent training for children with ADHD? A randomized controlled multicenter trial. J. Child. Psychol. Psychiatry 56 , 1298–1313 (2015).
Kosheleff, A. R., Mason, O., Jain, R., Koch, J. & Rubin, J. Functional impairments associated with ADHD in adulthood and the impact of pharmacological treatment. J. Atten. Disord. 27 , 669–697 (2023).
Chien, W. C. et al. The risk of injury in adults with attention-deficit hyperactivity disorder: a nationwide, matched-cohort, population-based study in Taiwan. Res. Dev. Disabil. 65 , 57–73 (2017).
Klein, R. G., Pine, D. S. & Klein, D. F. Resolved: mania is mistaken for ADHD in prepubertal children. J. Am. Acad. Child. Adolesc. Psychiatry 37 , 1093–1096 (1998).
Pawaskar, M., Fridman, M., Grebla, R. & Madhoo, M. Comparison of quality of life, productivity, functioning and self-esteem in adults diagnosed with ADHD and with symptomatic ADHD. J. Atten. Disord. 24 , 136–144 (2019).
Philipsen, A. et al. Early maladaptive schemas in adult patients with attention deficit hyperactivity disorder. Atten. Defic. Hyperact. Disord. 9 , 101–111 (2017).
Ware, J. E. & Sherbourne, C. D. The MOS 36-item short form health survey (SF-36): I. Conceptual framework and item selection. Med. Care 30 , 473–483 (1992).
Endicott, J., Nee, J., Harrison, W. & Blumenthal, R. Quality of life enjoyment and satisfaction questionnaire: a new measure. Psychopharmacol. Bull. 29 , 321–326 (1993).
CAS PubMed Google Scholar
Brod, M., Johnston, J., Able, S. & Swindle, R. Validation of the adult attention-deficit/hyperactivity disorder quality-of-life scale (AAQoL): a disease-specific quality-of-life measure. Qual. Life Res. 15 , 117–129 (2006).
Weiss, M. D. et al. Moderators and mediators of symptoms and quality of life outcomes in an open-label study of adults treated for attention-deficit/hyperactivity disorder. J. Clin. Psychiatry 71 , 381–390 (2010).
Coghill, D. R., Banaschewski, T., Soutullo, C., Cottingham, M. G. & Zuddas, A. Systematic review of quality of life and functional outcomes in randomized placebo-controlled studies of medications for attention-deficit/hyperactivity disorder. Eur. Child. Adolesc. Psychiatry 26 , 1283–1307 (2017).
Chang, Z. et al. Risks and benefits of attention-deficit/hyperactivity disorder medication on behavioral and neuropsychiatric outcomes: a qualitative review of pharmacoepidemiology studies using linked prescription databases. Biol. Psychiatry 86 , 335–343 (2019).
Chang, Z. et al. Association between medication use for attention-deficit/hyperactivity disorder and risk of motor vehicle crashes. JAMA Psychiatry 74 , 597–603 (2017).
Quinn, P. D. et al. ADHD medication and substance-related problems. Am. J. Psychiatry 174 , 877–885 (2017).
Lu, Y. et al. Association between medication use and performance on higher education entrance tests in individuals with attention-deficit/hyperactivity disorder. JAMA Psychiatry 74 , 815–822 (2017).
Chen, V. C. H. et al. Methylphenidate and mortality in children with attention-deficit hyperactivity disorder: population-based cohort study. Br. J. Psychiatry 220 , 64–72 (2022).
Agarwal, R., Goldenberg, M., Perry, R. & William Ishak, W. The quality of life of adults with attention deficit hyperactivity disorder: a systematic review. Innov. Clin. Neurosci. 9 , 10–21 (2012).
Adler, L. A. et al. Atomoxetine treatment in adults with attention-deficit/hyperactivity disorder and comorbid social anxiety disorder. Depress Anxiety 26 , 212–221 (2009).
Adler, L. A. et al. Once-daily atomoxetine for adult attention-deficit/hyperactivity disorder: a 6-month, double-blind trial. J. Clin. Psychopharmacol. 29 , 44–50 (2009).
Adler, L. A. et al. Self-reported quality of life in adults with attention-deficit/hyperactivity disorder and executive function impairment treated with lisdexamfetamine dimesylate: a randomized, double-blind, multicenter, placebo-controlled, parallel-group study. BMC Psychiatry 13 , 253 (2013).
Spencer, T. J. et al. Attention-deficit/hyperactivity disorder-specific quality of life with triple-bead mixed amphetamine salts (SPD465) in adults: results of a randomized, double-blind, placebo-controlled study. J. Clin. Psychiatry 69 , 1766–1775 (2008).
Durell, T. M. et al. Atomoxetine treatment of attention-deficit/hyperactivity disorder in young adults with assessment of functional outcomes: a randomized, double-blind, placebo-controlled clinical trial. J. Clin. Psychopharmacol. 33 , 45–54 (2013).
Goodman, D. W., Ginsberg, L., Weisler, R. H., Cutler, A. J. & Hodgkins, P. An interim analysis of the quality of life, effectiveness, safety, and tolerability (QU.E.S.T.) evaluation of mixed amphetamine salts extended release in adults with ADHD. CNS Spectr. 10 , 26–34 (2005).
Lücke, C. et al. Long-term improvement of quality of life in adult ADHD – results of the randomized multimodal COMPAS trial. Int. J. Ment. Health 50 , 250–270 (2021).
Tsujii, N. et al. Effect of continuing and discontinuing medications on quality of life after symptomatic remission in attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. J. Clin. Psychiatry 81 , 19r13015 (2020).
Ramsay, J. R. Assessment and monitoring of treatment response in adult ADHD patients: current perspectives. Neuropsychiatr. Dis. Treat. 13 , 221–232 (2017).
Hegvik, T. A. et al. Druggable genome in attention deficit/hyperactivity disorder and its co-morbid conditions. New avenues for treatment. Mol. Psychiatry 26 , 4004–4015 (2021).
Malik, M. A., Faraone, S. V., Michoel, T. & Haavik, J. Use of big data and machine learning algorithms to extract possible treatment targets in neurodevelopmental disorders. Pharmacol. Ther. 250 , 108530 (2023).
Hoogman, M., Stolte, M., Baas, M. & Kroesbergen, E. Creativity and ADHD: a review of behavioral studies, the effect of psychostimulants and neural underpinnings. Neurosci. Biobehav. Rev. 119 , 66–85 (2020).
Hess, J. L. et al. A polygenic resilience score moderates the genetic risk for schizophrenia: replication in 18,090 cases and 28,114 controls from the Psychiatric Genomics Consortium. Am. J. Med. Genet. B Neuropsychiatr. Genet . 195 , e32957 (2023).
Hou, J. et al. Polygenic resilience scores capture protective genetic effects for Alzheimer’s disease. Transl. Psychiatry 12 , 296 (2022).
Nigg, J. T. Considerations toward an epigenetic and common pathways theory of mental disorder. J. Psychopathol. Clin. Sci. 132 , 297–313 (2023).
Garcia-Argibay, M. et al. Predicting childhood and adolescent attention-deficit/hyperactivity disorder onset: a nationwide deep learning approach. Mol. Psychiatry 28 , 1232–1239 (2022).
Biederman, J. et al. Evidence of low adherence to stimulant medication among children and youths with ADHD: an electronic health records study. Psychiatr. Serv. 70 , 874–880 (2019).
Biederman, J. et al. Further evidence of low adherence to stimulant treatment in adult ADHD: an electronic medical record study examining timely renewal of a stimulant prescription. Psychopharmacology 237 , 2835–2843 (2020).
Brikell, I. et al. ADHD medication discontinuation and persistence across the lifespan: a retrospective observational study using population-based databases. Lancet Psychiatry 11 , 16–26 (2024).
Manalili, M. A. R. et al. From puzzle to progress: how engaging with neurodiversity can improve cognitive science. Cogn. Sci. 47 , e13255 (2023).
Rostain, A., Jensen, P. S., Connor, D. F., Miesle, L. M. & Faraone, S. V. Toward quality care in ADHD: defining the goals of treatment. J. Atten. Disord. 19 , 99–117 (2015).
Higdon, C., Blader, J., Kalari, V. K. & Fornari, V. M. Measurement-based care in the treatment of attention-deficit/hyperactivity disorder and disruptive behavior disorders. Child. Adolesc. Psychiatr. Clin. N. Am. 29 , 663–674 (2020).
Faraone, S. V. et al. The adult ADHD quality measures initiative. J. Atten. Disord. 23 , 1063–1078 (2019).
Callen, E. F. et al. Progress and pitfalls in the provision of quality care for adults with attention deficit hyperactivity disorder in primary care. J. Atten. Disord. 27 , 575–582 (2023).
Demontis, D. et al. Discovery of the first genome-wide significant risk loci for attention deficit/hyperactivity disorder. Nat. Genet. 51 , 63–75 (2019).
Thapar, A. et al. Psychiatric gene discoveries shape evidence on ADHD’s biology. Mol. Psychiatry 21 , 1202–1207 (2015).
Dark, C., Homman-Ludiye, J. & Bryson-Richardson, R. J. The role of ADHD associated genes in neurodevelopment. Dev. Biol. 438 , 69–83 (2018).
Sollis, E. et al. Equivalent missense variant in the FOXP2 and FOXP1 transcription factors causes distinct neurodevelopmental disorders. Hum. Mutat. 38 , 1542–1554 (2017).
Harrington, A. J. et al. MEF2C regulates cortical inhibitory and excitatory synapses and behaviors relevant to neurodevelopmental disorders. Elife 5 , e20059 (2016).
Lionel, A. C. et al. Rare copy number variation discovery and cross-disorder comparisons identify risk genes for ADHD. Sci. Transl. Med. 3 , 95ra75 (2011).
Lee, P. H. et al. Genomic relationships, novel loci, and pleiotropic mechanisms across eight psychiatric disorders. Cell 179 , 1469–1482.e11 (2019).
Cortese, S., Newcorn, J. H. & Coghill, D. A practical, evidence-informed approach to managing stimulant-refractory attention deficit hyperactivity disorder (ADHD). CNS Drugs 35 , 1035–1051 (2021).
Download references
Acknowledgements
S.V.F. is supported by the European Union’s Horizon 2020 research and innovation programme (grant agreement 965381), NIMH (grants U01AR076092-01A1, 1R21MH1264940, R01MH116037 and 1R01NS128535-01), Oregon Health and Science University, Otsuka Pharmaceuticals, Noven Pharmaceuticals Incorporated, and Supernus Pharmaceutical Company. M.A.B. is supported by a Senior Research Fellowship (level B) from the Australian National Health and Medical Research Council (NHMRC; 1154378). His research programme is supported by the NHMRC (2010899) and Medical Research Future Fund of Australia (MRF2006438, EPCD000002). I.B. is supported by the European Union’s Horizon 2020 research and innovation programme (grant agreement 965381). S.C., NIHR Research Professor (NIHR303122), is funded by the NIHR for this research project. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR, NHS or the UK Department of Health and Social Care. S.C. is also supported by NIHR grants NIHR203684, NIHR203035, NIHR130077, NIHR128472 and RP-PG-0618-20003 and by grant 101095568-HORIZONHLTH-2022-DISEASE-07-03 from the European Research Executive Agency. C.A.H. is supported by the European Union’s Horizon 2020 research and innovation programme (grant agreement 965381), and ZonMW (grants 636340003 and 636340002). C.H. is supported by the NIHR (grants MIC-2016-003 and NIHR203310), and by the UKRI Medical Research Council (grant MR/T046864/1). J.H.N. is supported by grants from the National Institute of Child Health and Human Development (R01; HD093612) and the National Institute on Drug Abuse (R21; DA054281). A.P. is currently supported by funding from the National Institute for Health and Care Research (grant NIHR203035), the European Union’s Horizon 2020 research and innovation programme (grant agreement 945151), German Research Foundation (grant PH 177/7-1), Ministry of Culture and Science of the State of North Rhine-Westphalia (grant IBehave), Ministry of Research and Education (grants 01NVF20004 and 01IS22085D (Eureka Cluster on software innovation)). G.V.P. is supported by São Paulo Research Foundation (FAPESP) (grant 2016/22455-8), and National Council for Scientific and Technological Development (CNPq; grant 310582/2017-2). K.R. is supported by the National Institute of Health Research (grants NIHR130077 and NIHR203684) and the UK Department of Health and Social Care via the NIHR Biomedical Research Centre (BRC) for Mental Health at South London and the Maudsley National Health Service (NHS) Foundation Trust and the IoPPN, King’s College London. M.H.S. is supported by the Institute of Education Sciences (grant R305A210462) and the National Institute of Mental Health (grants R34 MH125037 and R34 MH122225). J.K.B. is supported by the European Union’s Horizon 2020 research and innovation programme (grant agreements 115300 and 777394 (EU-AIMS and AIMS-2-TRIALS), 847818 (CANDY), and 847879 (PRIME)).
Author information
Authors and affiliations.
Departments of Psychiatry and of Neuroscience and Physiology, Norton College of Medicine at SUNY Upstate Medical University, Syracuse, NY, USA
Stephen V. Faraone
School of Psychological Sciences, Turner Institute for Brain and Mental Health, Monash University, Melbourne, Victoria, Australia
Mark A. Bellgrove
Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden
Isabell Brikell
Department of Global Public Health and Primary Care, University of Bergen, Bergen, Norway
Department of Biomedicine, Aarhus University, Aarhus, Denmark
Centre for Innovation in Mental Health, School of Psychology, Faculty of Environmental and Life Sciences, University of Southampton, Southampton, UK
Samuele Cortese
Clinical and Experimental Sciences (CNS and Psychiatry), Faculty of Medicine, University of Southampton, Southampton, UK
Solent NHS Trust, Southampton, UK
Hassenfeld Children’s Hospital at NYU Langone, New York University Child Study Center, New York City, NY, USA
DiMePRe-J-Department of Precision and Rigenerative Medicine-Jonic Area, University of Bari “Aldo Moro”, Bari, Italy
Interdisciplinary Center Psychopathology and Emotion regulation (ICPE), Department of Psychiatry, University Medical Center Groningen, University of Groningen, Groningen, Netherlands
Catharina A. Hartman
National Institute for Health and Care Research (NIHR) MindTech MedTech Co-operative and NIHR Nottingham Biomedical Research Centre, Institute of Mental Health, Mental Health and Clinical Neurosciences, School of Medicine, University of Nottingham, Nottingham, UK
Chris Hollis
Department of Psychiatry, Icahn School of Medicine at Mount Sinai, New York, NY, USA
Jeffrey H. Newcorn
Department of Psychiatry and Psychotherapy, University Hospital Bonn, Bonn, Germany
Alexandra Philipsen
Department of Psychiatry, Faculdade de Medicina FMUSP, Universidade de São Paulo, São Paulo, Brazil
Guilherme V. Polanczyk
Department of Child & Adolescent Psychiatry, Institute of Psychiatry, Psychology & Neurosciences, King’s College London, London, UK
Katya Rubia
Department of Child & Adolescent Psychiatry, Transcampus Professor KCL-Dresden, Technical University, Dresden, Germany
University of Washington School of Medicine, Seattle, WA, USA
Margaret H. Sibley
Department of Cognitive Neuroscience, Donders Institute for Brain, Cognition and Behaviour, Radboudumc, Nijmegen, Netherlands
Jan K. Buitelaar
Karakter Child and Adolescent Psychiatry University Center, Nijmegen, Netherlands
You can also search for this author in PubMed Google Scholar
Contributions
Introduction (S.V.F. and J.K.B.); Epidemiology (C.A.H. and G.V.P.); Mechanisms/pathophysiology (I.B., K.R., M.A.B. and S.V.F.); Diagnosis and screening (M.H.S. and S.C.); Management (J.H.N., S.C., A.P., M.H.S., J.K.B., M.A.B., K.R. and C.H.); Quality of life (G.V.P. and A.P.); Outlook (J.K.B. and S.V.F.). Aside from the first and last authors, authorship is alphabetical. All authors extensively commented on each other’s sections.
Corresponding author
Correspondence to Stephen V. Faraone .
Ethics declarations
Competing interests.
S.V.F. in the past year received income, potential income, travel expenses, continuing education support and/or research support from Aardvark, Aardwolf, AIMH, Tris, Otsuka, Ironshore, Kanjo, Johnson & Johnson/Kenvue, KemPharm/Corium, Akili, Supernus, Atentiv, Noven, Sky Therapeutics, Axsome and Genomind; with his institution, he has US patent US20130217707 A1 for the use of sodium–hydrogen exchange inhibitors in the treatment of ADHD; he also receives royalties from books published by Guilford Press ( Straight Talk about Your Child’s Mental Health ), Oxford University Press ( Schizophrenia: The Facts ) and Elsevier ( ADHD: Non-Pharmacologic Interventions ); and he is Program Director of www.ADHDEvidence.org and www.ADHDinAdults.com . S.C. declares honoraria and reimbursement for travel and accommodation expenses for lectures from the following non-profit associations: Association for Child and Adolescent Central Health (ACAMH), Canadian ADHD Resource Alliance (CADDRA), British Association for Psychopharmacology (BAP), and Healthcare Convention for educational activity on ADHD. C.H. was a member of the UK National Institute for Health and Care Excellence (NICE) ADHD Guideline Committee (CG87); has received honoraria for lectures from BAP; and is a member of the European ADHD Guideline Group (EAGG) (eunethydis.eu/eunethydis-initiatives/european-adhd-guideline-group/). J.H.N. in the past year is/has been an adviser and/or consultant for Corium, Hippo T&C, Ironshore, Lumos, Medice, MindTension, OnDosis, Otsuka, Signant Health and Supernus; he has received research support from the National Institute on Drug Abuse (NIDA), the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) and Otsuka; he also has received honoraria from for disease state presentations from Otsuka, and served as a consultant for the US National Football League. A.P. declares that she served on advisory boards, gave lectures, performed phase III studies and received travel grants within the last 5 years from MEDICE Arzneimittel, Pütter GmbH and Co KG, Takeda, Boehringer and Janssen-Cilag, and receives royalties from books published by Elsevier, Hogrefe, MWV, Kohlhammer, Karger, Oxford University Press, Thieme, Springer and Schattauer; she is a member of the German ADHD Guideline Group, and is an author of the Updated European Consensus Statement. G.V.P. has served as a speaker and/or consultant to Abbott, Ache, Medice, Novo Nordisk, Pfizer and Takeda, and receives authorship royalties from Manole Editors. K.R. has received a grant from Takeda Pharmaceuticals for another project and consulting fees from Supernus and Lundbeck. M.H.S. has consulted with Supernus Pharmaceuticals and Tieffenbacher Pharmaceuticals in the past 12 months, and receives book royalties from Guilford Press. J.K.B. has been in the past 3 years a consultant to/member of advisory board of and/or speaker for Takeda, Roche, Medice, Angelini, Boehringer-Ingelheim and Servier; he is not an employee of any of these companies, and is not a stock shareholder of any of these companies; he has no other financial or material support, including expert testimony, patents and royalties. M.A.B. declares travel expenses and speaking fees attached to conference presentations and professional groups. I.B. and C.A.H. declare no competing interests.
Peer review
Peer review information.
Nature Reviews Disease Primers thanks S. Gau, L. J. Wang, M. Weiss and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary information, rights and permissions.
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Cite this article.
Faraone, S.V., Bellgrove, M.A., Brikell, I. et al. Attention-deficit/hyperactivity disorder. Nat Rev Dis Primers 10 , 11 (2024). https://doi.org/10.1038/s41572-024-00495-0
Download citation
Accepted : 16 January 2024
Published : 22 February 2024
DOI : https://doi.org/10.1038/s41572-024-00495-0
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.

Click through the PLOS taxonomy to find articles in your field.
For more information about PLOS Subject Areas, click here .
Loading metrics
Open Access
Peer-reviewed
Research Article
The impact of psychological theory on the treatment of Attention Deficit Hyperactivity Disorder (ADHD) in adults: A scoping review
Contributed equally to this work with: Rebecca E. Champ
Roles Conceptualization, Data curation, Formal analysis, Writing – original draft
* E-mail: [email protected]
Affiliation Department of Nursing and Midwifery, School of Human and Health Sciences, University of Huddersfield, Huddersfield, United Kingdom
Roles Supervision
¶ ‡ These authors also contributed equally to this work.
Affiliation School of Health and Life Sciences, Teeside University, Middlesbrough, United Kingdom
- Rebecca E. Champ,
- Marios Adamou,
- Barry Tolchard
- Published: December 21, 2021
- https://doi.org/10.1371/journal.pone.0261247
- Peer Review
- Reader Comments
Psychological theory and interpretation of research are key elements influencing clinical treatment development and design in Attention Deficit Hyperactivity Disorder (ADHD). Research-based treatment recommendations primarily support Cognitive Behavioural Therapy (CBT), an extension of the cognitive behavioural theory, which promotes a deficit-focused characterisation of ADHD and prioritises symptom reduction and cognitive control of self-regulation as treatment outcomes. A wide variety of approaches have developed to improve ADHD outcomes in adults, and this review aimed to map the theoretical foundations of treatment design to understand their impact. A scoping review and analysis were performed on 221 documents to compare the theoretical influences in research, treatment approach, and theoretical citations. Results showed that despite variation in the application, current treatments characterise ADHD from a single paradigm of cognitive behavioural theory. A single theoretical perspective is limiting research for effective treatments for ADHD to address ongoing issues such as accommodating context variability and heterogeneity. Research into alternative theoretical characterisations of ADHD is recommended to provide treatment design opportunities to better understand and address symptoms.
Citation: Champ RE, Adamou M, Tolchard B (2021) The impact of psychological theory on the treatment of Attention Deficit Hyperactivity Disorder (ADHD) in adults: A scoping review. PLoS ONE 16(12): e0261247. https://doi.org/10.1371/journal.pone.0261247
Editor: Gerard Hutchinson, University of the West Indies at Saint Augustine, TRINIDAD AND TOBAGO
Received: May 21, 2021; Accepted: November 25, 2021; Published: December 21, 2021
Copyright: © 2021 Champ et al. This is an open access article distributed under the terms of the Creative Commons Attribution License , which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: All relevant data are within the paper and its Supporting Information files.
Funding: The author(s) received no specific funding for this work.
Competing interests: The authors have declared that no competing interests exist.
Introduction
The combination of psychological theory and interpretation of research have been highlighted as critical influencers guiding decision-making for clinical treatment design and development for Attention Deficit Hyperactivity Disorder (ADHD) [ 1 , 2 ]. ADHD is a neurodevelopmental disorder of self-regulation with symptoms negatively affecting daily functioning at work and at home, with long-term impacts in academic, occupational, social and emotional areas of functioning [ 3 – 8 ]. Effective, long-term treatment outcomes benefit both the individual with ADHD and society as a whole as undiagnosed and untreated adults with ADHD may become an economic burden due to increased health care costs and decreased productivity at work [ 9 , 10 ].
Russell Barkley [ 11 ] postulated the first unifying theory of ADHD, which places a core deficit of behavioural inhibition at the source of ADHD behaviours. Several theoretical models attribute additional and alternative cognitive sources for the development of ADHD symptoms [ 12 – 14 ]. While a variety of different interventions are available and the benefit of other forms of support is acknowledged (e.g. psychotherapy or coaching), only Cognitive Behavioural Therapy (CBT), Mindfulness, Dialectical Behavioural Therapy (DBT) and potentially Neurofeedback have the most empirical support [ 15 ]. Results of non-pharmacological intervention studies suggest these interventions have a positive effect on core behavioural symptoms of ADHD (inattention, hyperactivity/impulsivity), particularly when compared to inactive control conditions [ 15 , 16 ]. However, recent systematic reviews of non-pharmacological treatment highlight that different classes of intervention design take similar approaches; that heterogeneity in sample size, study design, quality and symptom outcome measurement makes meta-analysis difficult, and there is a high risk of bias [ 15 – 17 ]. Additionally, the National Institute for Health and Care Excellence (NICE) [ 18 ] only recommends interventions that match a similar protocol to medications: Randomised Controlled Trials (RCTs), primarily based in CBT [ 15 ], despite a growing wider evidence base.
It is hypothesised that much of current research for the characterisation of ADHD is based on a cognitive behavioural theoretical paradigm that does not account comprehensively for the broad spectrum of ADHD presentation [ 1 , 19 – 24 ]. This paradigm is deficit-focused with primary treatment outcomes of symptom reduction and control of maladaptive behaviours. Recent research in psychology suggests that this may not be the best approach to improving mental health, and it may be necessary to develop positive psychological factors and emotions that cultivate health and wellbeing [ 25 , 26 ]. This scoping review aims to map the evidence and understand the influence of current psychological theories on design and treatment recommendations in adult ADHD by answering the following questions:
- Are characterisations of ADHD dominated by a cognitive behavioural paradigm?
- Does that paradigm influence treatment design and outcomes?
- Are there any alternative characterisations of ADHD that present a different perspective to the cognitive behavioural paradigm?
A broad approach was considered most effective to identify gaps in the literature, as data regarding supportive psychological theories would likely be identified in publications beyond specific study designs. To our knowledge, this is the first scoping review providing an overview of the theoretical characterisations of ADHD and their impact on available treatments.
Search strategy
The scoping review was carried out over three months: February, March and April 2020. The scoping review protocol was published on the Open Science Framework ( https://osf.io/ ). Search design and criteria were formulated based on guidance and recommendations by Arksey & O’Malley [ 27 ], Colquhoun et al. [ 28 ], O’Brien et al. [ 29 ] and the Joanna Briggs Institute [ 30 ]. A starting timeframe from the publication of Barkley’s [ 11 ] theory was selected as the foundation for current theoretical characterisations of ADHD. Papers were reviewed from multiple countries, including the United States, the United Kingdom, The Netherlands, Canada, Argentina, Brazil, Colombia, Iceland, Ireland, Portugal, Spain, Belgium, Germany, Switzerland, Finland, Sweden, Israel, Iran, China, Hong Kong, India and Australia, and multiple languages including English, Dutch, German, French, and Spanish.
Research evidence was identified by conducting searches across web-based databases with pre-determined search terms. Table 1 outlines the search terms and syntax used in primary and secondary searches.
- PPT PowerPoint slide
- PNG larger image
- TIFF original image
https://doi.org/10.1371/journal.pone.0261247.t001
Additional searches were in generic search engines Google and Google Scholar, and checks of references from guidance documents and systematic reviews for additional material. Once identified, these references were collected through additional database searches or a direct search in the specific journal or publication.
Inclusion criteria
Titles and abstracts of materials were reviewed for eligibility. Materials were considered appropriate if they met the following criteria:
- Studies involving research on a pilot, efficacy, or applicability of a treatment intervention for adults with ADHD (19–65+, male and female)
- Systematic reviews of treatment literature or specific approaches to treatment for adults with ADHD
- Thesis, conference papers, or reports reviewing, presenting, or recommending treatment approaches for adults with ADHD
- Documents, articles, books, or consensus statements presenting guidance or recommendations for treatment for adults with ADHD
Exclusion criteria
In addition to meeting the inclusion criteria, materials were excluded if they met one of the following exclusion criteria:
- Treatment approaches designed for a specific subset of participants (couples, military, substance abuse)
- Treatment approaches designed to treat specific comorbidities (Autism, Bi-polar, Learning Disabilities, Tourette’s, Oppositional Defiant Disorder, Personality Disorder, Traumatic Brain Injury)
- Treatment approaches designed for the inclusion of younger age groups (children, adolescents) or their parents
- Materials summarising and updating recent developments in the field of treatment for adult ADHD (general practice journals, nursing practice journals, medical student journals)
- Characterisations of adult ADHD that were not empirically researched
A large body of literature has been published over the years which present different characterisations of adult ADHD and subsequent recommendations for treatment. Predominantly based in the US, these biopsychosocial models range from origin theories of genetic strengths [ 31 ], diversity [ 32 ] and developmental impairment of the prefrontal cortex due to issues with attachment and trauma [ 33 ], to identifying multiple presentations of ADHD diagnosed individually with SPECT imaging [ 34 ]. While these models do present alternative characterisations of ADHD, they are not empirically researched and therefore will be excluded from this review.
The following PRISMA flowchart ( Fig 1 ) presents the search process details, including the number of articles located, those eliminated and those included in the final analysis.
https://doi.org/10.1371/journal.pone.0261247.g001
Results and analysis
The 221 articles were subdivided into the following categories according to their primary content: Cognitive Behavioural Therapy (122), Coaching (36), Psychotherapy (16), and Other (47). All articles were assessed for quality against the relevant Critical Appraisals Skills Programme (CASP) checklists. Results summary of the ADHD characterisation cited for each intervention category is displayed in a mosaic plot ( Fig 2 ).
https://doi.org/10.1371/journal.pone.0261247.g002
An overview of interventions published by year is displayed in a column chart ( Fig 3 ).
https://doi.org/10.1371/journal.pone.0261247.g003
Due to the number and variety of materials, a narrative analysis was performed to review the publications’ composition. Systematic reviews were also analysed separately to see if any review of the characterisation of ADHD had been completed previously.
Systematic reviews
Over the years, several systematic reviews of treatments for adult ADHD have been published. Searches were undertaken through Joanna Briggs Institute Evidence Synthesis, The Cochrane Database of Systematic Reviews, and the Campbell Library show some of these reviews are specific to the efficacy of a particular intervention approach, such as psychodynamic therapy [ 35 ], homoeopathy [ 36 ], Cognitive Behavioural Therapy (CBT) [ 37 – 41 ], Mindfulness [ 42 , 43 ], and Meditation [ 44 , 45 ]. Others have been focused on efficacy [ 2 , 15 , 16 , 46 – 48 ], long term outcomes [ 10 , 49 ], or guidance [ 50 ]. Only one systematic review investigated the characterisation of adult ADHD but failed to find evidence of neurocognitive disfunction as a predictor of persistence [ 51 ]. Interestingly, one systematic review investigated how adults with ADHD experience and manage their symptoms [ 52 ]. Therefore, it seems that no recent attempt has reviewed the psychological theories for the characterisation of adult ADHD.
Data extraction
Articles were reviewed, and data extracted into categorised excel spreadsheets for comparison. Each document was examined for the following criteria:
- Research Purpose/Outcome
- Treatment Approach
- ADHD Characterisation
- ADHD Theory
Intervention analysis
Research studies and guidance documents present treatment approaches in various environments, contexts and skill levels of delivery. The following interventions present a wide range of delivery in clinical and non-clinical environments; therapeutic, academic, and social contexts; and professionals including psychiatrists, clinical psychologists, nurses, occupational therapists, psychotherapists, as well as counsellors, coaches, and mentors.
Cognitive Behavioural Therapy (CBT).
Due to the involvement of cognitive behavioural theory in establishing the characterisation of ADHD, the bulk of research in the field has used this intervention model. While recommended as the primary treatment modality, treatment goals and methodologies have changed over time. Due to this shift in focus, some early research references non-empirical anecdotal work. This analysis will use the delineation of “waves” as seen in the current theoretical literature to demonstrate these changes [ 53 ] ( S1 Appendix ).
First wave : Behaviourism . Before 1990, ADHD was still considered a disorder of childhood. Although considerable research exists regarding “first wave” treatments in children, the few approaches developed for adults apply pure behavioural theory and techniques. A case study of three subjects focused on improving attentional behaviour in psychiatric patients [ 54 ], and the design utilises operant theory and models used for brain injury [ 55 ]. Guidance documents for teachers, parents and counsellors [ 56 ] and psychotherapists [ 57 ] highlight the importance of behavioural skill development. The conceptualisation of ADHD in these treatment models is a disorder of attention [ 54 ] and a neurobiological disorder of self-regulation, executive function deficits and disinhibition [ 56 , 57 ]. Burgess et al. [ 54 ] exemplify the transition of the conceptualisation of attentional deficits in ADHD from mental illness to mental disorder.
The therapist’s role in these models is to assist the client in learning and practising practical behavioural strategies for task attention, organisation, listening and scheduling, and planning and organising daily activities. Treatment designs are varied, with only one specifying weekly sessions from 6–10 weeks [ 54 ]. Characterisation of ADHD aetiology highlight issues with inability to maintain vigilance (attention deficit) and distractibility [ 54 ], self-regulation, impaired inhibition, developmental delay, and deficits in executive function, referencing Barkley [ 56 , 57 ].
Rational Emotive Behaviour Therapy (REBT) . A single case study for ADHD specifically used REBT [ 58 ]. REBT approaches ADHD as a combination of neurobiological deficits [ 59 ] and developed secondary psychological personality disorders. Failure to develop cognitive structures leads to a lack of connection between thoughts, emotions and feelings, leading to deeply held distorted convictions and beliefs. The therapist’s role in this model is to assist the individual to dispute evaluative cognitions (“musts”) to develop a more rational philosophical orientation to the world. The approach incorporates independent “experiments” by clients outside of therapy, problem-solving methodology, and gentle introduction of rational self-statements for clients who lack the cognitive sophistication to engage in disputing of irrational beliefs [58, p. 95]. Treatment design has a developmental and longitudinal focus, in this case eight years. Characterisation of ADHD is described as DSM-IV core symptoms of attentional difficulties, impulsivity and hyperactivity [ 60 ] and references both Douglas’s [ 61 ] cognitive processing deficit model and Barkley’s [ 59 ] model of response inhibition and executive function deficits contributing to deficient self-regulation, impaired cross-temporal organisation of behaviour, and diminished social effectiveness and adaptation.
Second wave : Cognitive and cognitive behavioural therapy model . Cognitive and Cognitive Behavioural approaches are the primary and recommended treatment for working with ADHD and therefore make up the bulk of studies reviewed for this analysis. Considered “second wave” cognitive behavioural therapies, they consist of systematic reviews [ 2 , 37 , 38 , 41 ], randomised controlled trials (RCT) [ 62 – 80 ], group interventions [ 81 – 87 ], individual interventions [ 88 – 90 ], quantitative analysis [ 91 ], qualitative analysis [ 92 ], a cohort study [ 93 ], case-control studies [ 69 , 94 – 98 ], single case studies [ 99 – 102 ], multiple case studies [ 103 – 106 ], and psychotherapeutic treatment guidance [ 8 , 106 – 138 ]. Many of these studies deliver CBT as a standalone intervention, however multimodal treatment is recommended, and several treatment models include individual coaching or mentoring support alongside or in between CBT sessions [ 57 , 72 , 77 , 86 , 103 , 112 , 127 , 131 , 137 , 139 ]. One intervention also includes hypnosis and CBT [ 140 ].
Second wave interventions for ADHD recognise the neurobiological deficits as specific to the disorder and not brain injury. While they stress there is no “cure” for ADHD and the literature is clear that ADHD does not arise from distorted cognitions, cognitive treatment models focus primarily on improving, strengthening, or retraining cognitive abilities to increase awareness of behaviour and behavioural control. Early research identified cognitive distortions and maladaptive strategies and beliefs as interfering with skills acquisition and therefore needed support [ 104 , 136 ]. Further research shifted this view slightly to perceive the development of a negative self-concept as the core issue for maladaptive schema or “secondary symptoms” of stress, anxiety, depression, and chronic perceived failure attributed to a history of unachieved potential and negative feedback resulting from a lack of recognition of the disorder. [ 122 , 141 , 142 ]. Aims of treatment reduce deficit-based symptoms, develop environmental restructuring and accommodations, improve self-esteem and negative self-concept through disorder psychoeducation, and increase confidence in capabilities through supported skills practice and repetition. Approaches vary widely, including cognitive rehabilitation, cognitive and metacognitive remediation, and cognitive restructuring. However, most treatment approaches in this area are defined as Cognitive Behavioural Therapy (CBT) ( S1 Appendix ).
The therapists’ role in these models is more a “partner”, “expert teacher-motivator” [ 122 ] and collaborator than the traditional medical expert role [ 117 , 121 , 129 ]. Originally defined by Hallowell & Ratey [ 143 ] as “coaching”, therapists are encouraged to be active and directive in providing structure and redirection to goals or session topics [ 83 , 87 , 101 , 108 , 129 , 135 , 137 , 144 ]. Failure to initiate behavioural changes or maintain new habits and strategies, or “procrastivity”, is attributed to motivational problems due to the nature of the disorder [ 8 , 108 , 121 , 145 ]. CBT for ADHD identifies the ADHD client’s difficulty with delayed gratification and generation of positive emotions as the reason for lack of engagement or “Coping Drift”, where individuals stop implementing the skills taught in treatment [ 121 , 145 ]. Professionals are cautioned that repetition is key, and strategies must be reinforced, or relapse is likely. Therefore relapse prevention is included in practice as well as model design [ 8 , 70 , 71 , 74 , 83 , 86 , 93 , 94 , 108 , 121 , 126 , 136 , 145 , 146 ]. Recommendations for resistance or avoidance of aversive emotional states is to provide therapist support to develop tolerance [ 107 , 122 , 135 ], reframe past experiences [ 112 , 128 , 147 ], and build resilience when encountering setbacks [ 8 , 111 , 118 , 137 , 138 , 146 ]. Treatment designs are limited in length, either by the number of sessions (3 to 16) or by relevance (academic year) except for single case studies [ 99 – 102 , 104 ]. Intervention delivery methods vary from individual or group therapy and didactic teaching with therapeutic support to a computerised program and self-help manuals ( S1 Appendix ).
Characterisation of ADHD and aetiology highlight issues with attentional and behavioural control (hyperactivity, impulsivity, disorganisation) initially, but broadens to give a higher priority to executive dysfunction deficits, motivation and sustained attention, issues with emotional control and self-regulation. Guidance documents definitions of ADHD are often cited: of the 84 papers in this Second Wave analysis, 29 reference DSM-IV [ 60 ], seven reference DSM-IV-TR [ 148 ], and eight reference DSM-V [ 149 ]. Several studies reference alternative characterisations of ADHD, such as similarity to brain injury [ 117 ] and Brown’s Executive Function model [ 83 , 94 ]. However, Barkley is cited in 70 documents.
Third Wave : Mindfulness and acceptance . Third Wave cognitive behavioural interventions take a different treatment approach to traditional CBT. While they are similar in the practical application of behavioural techniques, they differ in their theoretical approach and the focus on cognitive change. Third-wave approaches explore context: the relationship between a person’s thoughts and emotions rather than content alone. This relationship includes a more holistic perspective of health beyond the reduction of disorders [ 53 ]. Therefore, this analysis will review them separately. These approaches include Metacognitive Therapy (MCT), Dialectical Behavioural Therapy (DBT), and Mindfulness Cognitive Behavioural Therapy (MCBT).
Metacognitive Therapy (MC) . Four documents used a metacognitive approach (MC), divided into group metacognitive therapy [ 5 , 76 , 150 ] and metacognitive remedial psychotherapeutic guidance [ 151 ]. Metacognitive interventions conceptualise ADHD as neurobiological dysfunction in the corticostriatal pathways, displayed as deficits in executive functions [ 151 ]. MC highlights the importance of awareness of cognitions or thinking about thinking to strengthen executive functions to enhance functioning and improve self-control. Borrowing from the psychoanalytic frame [ 152 ], treatment of this hybrid model aims to develop an “observing ego” or self-awareness, increasing the ability to be conscious of maladaptive thoughts and behaviours and confront them via self-analysis. The therapist’s role is to focus on cognitive and behavioural aspects of treatment and only address motivational or unconscious elements if they remain unexplained by neurobehavioural origins. Individual treatment plans are designed on a case-by-case basis to capture the individual’s unique problems and strengths. Analysis of authentic and emotionally charged experiences facilitates self-awareness using metaphoric problem identification, followed by strategy design and modification [ 151 ]. In group therapy, the therapist acts as an educator and facilitator, assisting with goal identification, the leading theme focused or problem assessment discussion, and offering support and encouragement [ 76 ]. Characterisation of ADHD focuses primarily on executive function deficits, followed by inattention and memory. This focus is reflected practically in treatment design as hyperactivity/impulsivity is considered less prevalent in adults [ 76 ]. Barkley is a primary citation in all four documents.
Dialectical Behavioural Therapy (DBT) . Ten studies identified an adapted model of Dialectical Behavioural Therapy (DBT) for ADHD. These consist of randomised controlled trials [ 21 , 153 – 155 ], a pragmatic open study [ 156 ], and group interventions [ 157 – 161 ]. This treatment model recognises ADHD neurobiological deficits but is grounded in a phenomenological conceptualisation, perceiving the nature of ADHD as a personality disorder. This conceptualisation is supported by similarities in symptoms and the positive response to the treatment of ADHD with comorbid Borderline Personality Disorder (BPD) [ 158 ]. Linehan [ 162 ] characterises BPD as a disorder of self-regulation from biological irregularities combined with dysfunctional environments, including their interaction and transaction. Experiences of invalidating environments impair childhood ability to learn to label experiences and emotions, modulate emotional arousal, tolerate distress, or form realistic goals and expectations, resulting in a child who invalidates their own experiences, generating a lack of self-trust. The adapted model is presented in group format of 13 weeks of 2-hour sessions. The design prioritises ADHD symptom-oriented modules, highlights non-empirically researched resources of ADHD [ 163 ], and includes DBT “mindfulness” training explicitly. The therapist’s role in the DBT adapted model for ADHD supports treatment aims of learning to “control ADHD—instead of being controlled by ADHD” through psychoeducation and provision of session structure and flexibility for individuals. A key therapist practice adopted from DBT is the dialectical balance between validating symptoms, aiming for a stabilising effect and encouragement of motivation, and skills training for behavioural change [ 158 ]. These models characterise ADHD as a deficit of attention and emotional control with hyperactive and impulsive behaviour, but later papers highlight issues with executive function and self-regulation [ 157 ]. Four studies cite Wender [ 164 ] as diagnostic criteria [ 153 , 158 – 160 ], two studies cite DSM-IV [ 154 , 155 ], and four studies cite Barkley specifically [ 21 , 156 , 157 , 161 ].
Mindfulness . Twenty-two documents included mindfulness in treatment options for ADHD. These included systematic reviews [ 42 , 165 – 167 ], randomised controlled trials [ 168 – 174 ], a pragmatic open study [ 156 ], group interventions [ 98 , 175 , 176 ], a case-control study [ 177 ], a multiple case study [ 178 ], and psychotherapeutic guidance [ 8 , 179 – 182 ]. Only two studies presented mindfulness treatment alone [ 98 , 156 ]. In Edel et al. [ 156 ], mindfulness was used as a comparator to DBT.
Mindfulness-based approaches conceptualise ADHD as a neurobiological disorder of self-regulation with deficits in executive function. Issues with sustained and selective attention are addressed by mindfulness meditation, which is presented as a self-regulatory practice recognised as mental training to strengthen and improve regulation of attention, emotions and brain function [ 167 , 175 , 177 , 181 ]. The therapist’s role is primarily to introduce and support developing the new skill set of “mindful awareness” or cognitive defusion to facilitate the ability to decrease emotional responses while continuing to act [ 8 ]. Interestingly, Zylowska’s [ 175 , 176 ] Mindfulness-Based Cognitive Therapy treatment model includes within its psychoeducation a characterisation of ADHD as a “neurobiological difference” with both evolutionary non-adaptive and potentially adaptive aspects [ 183 – 185 ]. However, within the treatment approach, the ADHD characterisation remains based on cognitive behavioural theory.
Treatment is in a group format, and length varies from 8 to 12 weeks of 2 to 3-hour sessions. The characterisation is reasonably consistent across this group, focusing primarily on poor sustained attention, inhibition and emotional dysregulation attributed to executive dysfunction, with one study highlighting impairments in performance monitoring [ 173 ]. Two papers cite DSM IV [ 42 , 168 ], two cite DSM V [ 167 , 170 ], and sixteen cite Barkley specifically [ 8 , 98 , 156 , 165 , 166 , 169 , 171 – 173 , 175 , 176 – 180 , 182 ].
Thirty-six documents presented coaching as a beneficial intervention for ADHD. These include a systematic review [ 186 ], a randomised controlled trial [ 187 ], individual interventions [ 188 – 199 ], qualitative studies [ 200 – 204 ], quantitative studies [ 205 – 207 ], and psychotherapeutic guidance [ 118 , 143 , 208 – 218 ]. It is important to note that nineteen studies were conducted at university for students, and therefore have academic goal achievement as a focus [ 187 – 195 , 197 – 199 , 201 , 204 , 206 , 208 , 212 ].
The term “coaching therapy” was coined by Hallowell and Ratey [ 143 ] to highlight the need for a therapist to take a more “active, encouraging role” with ADHD patients. The role of the “therapist-coach” was to provide a structuring force, maintaining focus and reminding patients of goals and objectives through directive interaction, as opposed to open-ended psychoanalysis. ADHD Coaching has since developed into an independent modality, which can be delivered alone or as part of a multi-modal approach. The ADHD Coaches Organisation (ACO) defines ADHD Coaching as a blending of three elements: Life Coaching, Skills Coaching, and Education [ 218 ]. Life coaching separates ADHD Coaching from therapy by highlighting the therapist-client relationship’s collaborative nature, where the coach supports client self-awareness and achievement of self-identified goals, providing structure and accountability as needed. The client is viewed as a creative and resourceful expert with individual strengths which are leveraged in skills coaching to design systems and strategies to strengthen clients’ ability to manage daily life. Education is provided through relevant ADHD research and tools, as requested by the client or as needed.
Conceptualisations of ADHD within coaching models focus almost exclusively on working with neurobiological deficits in executive function, with the primary treatment aim to set and achieve goals and develop skill sets to support practical day to day management. Some models even define themselves specifically as “Executive Function Coaching” [ 191 , 195 , 198 , 204 , 206 , 208 ]. However, some models highlight ADHD Coaching as based on or similar to CBT [ 186 , 196 , 199 , 208 ]. The role of the coach is to support clients to improve self-regulation, defined as the ability to persist in goal-directed behaviour through time [ 204 , 209 ], by modelling cognitive strategies, practising non-judgement, offering pragmatic support and guidance, and holding clients accountable by reflection in session or monitoring progress via between session check-ins. Negative emotions are addressed as barriers to goal achievement and confidence, but models are specific that ADHD coaching is practical [ 186 ], dealing with “what, when and how–never why” [ 213 ].
Six documents mention self-determination models as part of a wider ADHD Coaching treatment model [ 190 , 191 , 194 , 195 , 204 , 206 ]. These are functional theory models designed to assist students, particularly those with learning disabilities, to develop internal or dispositional characteristics of self-determined behaviour and goal acquisition [ 219 – 221 ]. Field & Hoffman’s model [ 221 ] defines self-determination as the ability to define and achieve goals grounded in knowing and valuing oneself, which can be supported or thwarted by internal variables and environmental factors. The model specifically focuses on internal controllable variables to assist individuals to adapt to environments with unpredictable support. The core theory is that to be self-determined, one must develop internal awareness and the skills and strength to act on this internal foundation. The model has five major components:
- “Know Yourself”: Increase awareness of one’s preferences, strengths, weaknesses and needs by “dreaming” or overcoming barriers in socialised expectations for individuals with disabilities that limit options and perceptions of self-efficacy, building on a foundation for self-determined decision making.
- “Value Yourself”: Develop affective variables of self-esteem, including identifying strengths in areas commonly perceived as weakness, supporting the self-acceptance of disability and motivation for self-advocacy, increasing the ability to be self-determined.
- Plan: Learn planning skills and visual rehearsal of creative and effective actions for short-range steps leading to long term goals.
- Act: Awareness of how to assertively communicate goals, desires and intentions to others and access relevant resources. Understanding persistence, negotiation, and conflict resolution around risk-taking and barriers that may result from taking action.
- Experience Outcomes and Learn: Learn skills in evaluation of progress based on experience of change and comparison to expected outcomes. Recognition and celebration of successes crystallises the self-determination process.
Wehmeyer et al.’s model [ 219 , 222 ] is a teaching model to help students become causal agents. Based on cognitive behavioural theory [ 223 , 224 ], social cognitive theory [ 225 ] and research in self-management and self-control [ 226 ], this model defines self-determination as the abilities necessary to act as one’s primary causal agent and make choices and decisions about the quality of life free from external influence and interference [ 227 ]. Developed from a model designed to teach students decision making, independent performance, self-evaluation, and adjustment skills, the updated model includes defining those who are self-determined to persistently regulate problem-solving to meet self-directed personal goals using student-directed learning strategies [ 219 ]. This ability is developed through a learned problem-solving sequence of thoughts and actions to reduce the discrepancy between what students want or need and what they have or know. The sequence requires the students to 1) identify the problem; 2) identify potential solutions; 3) identify barriers to solving the problem; and 4) identify consequences to each solution, thereby enabling the student to regulate problem-solving by setting goals to meet needs, constructing plans to meet goals, and adjusting actions to complete plans [ 219 ]. A comprehensive combined curriculum of these frameworks was later developed [ 220 ]. While they provide support for client autonomy and causal agency within the design of these ADHD Coaching models, these models prioritise goal setting and identification as regulators for human behaviour and recommend student-directed learning strategies based on operant psychology, applied behavioural analysis and positive reinforcement techniques. Thus, treatment approaches for ADHD remain based on cognitive behavioural theory.
Treatment approaches in ADHD Coaching models are primarily cognitive behavioural, including reframing negative self-talk [ 228 ], continuous reinforcement [ 189 , 209 ], implementing rewards and consequences [ 188 , 189 , 192 , 196 , 212 ], and between-session assignments [ 192 , 196 , 209 , 217 ]. These models focus on the characterisation of ADHD as deficits in executive function relating to goal-directed behaviour, disorganisation and planning, motivation, and ultimately self-regulation. Citations for characterisation in ADHD Coaching models include one referencing DSM IV [ 211 ], three reference DSM-IV-TR [ 191 , 202 , 214 ], one reference to Brown’s Executive Function Model [ 195 ], and twenty-eight reference Barkley specifically [ 118 , 128 , 143 , 186 , 188 , 189 , 191 – 194 , 196 – 201 , 203 – 207 , 209 , 212 , 214 – 218 ].
Other interventions.
Fourty-seven documents describe non-pharmacological interventions not based on psychotherapy. These include Neurofeedback, Transcranial Stimulation, Hypnotherapy, Light Therapy, Computer-Based, Mentoring, Self-Monitoring, Binaural Beat Auditory Stimulation, and Movement-related interventions.
Neurofeedback . Twelve documents explored Neurofeedback as an intervention for ADHD. These include randomised controlled trials [ 229 – 231 ], individual interventions [ 232 , 233 ], case-control studies [ 234 , 235 ], a single case study [ 236 ], and treatment guidance [ 118 , 237 – 239 ]. Neurofeedback (NF) treatment models focus heavily on neurocognitive deficits as being the origin of ADHD behaviours. The research uses Electroencephalography (EEG) measures to study the correspondences between intracranial electrical currents and responding voltages on the scalp. These measures indicate aspects of brain electrical function and processing, such as the electrical activity of various brain regions and their response to stimuli during cognitive tasks. EEG activity is quantified by computation of amplitude and power values for specific frequency bands of activity, source localization, and brain electrical activity mapping. Frequency refers to the number of oscillations, or waveforms, within a given time period. Analysis of waveforms, or a mixture of frequency bands, is a relational and complex process of examining frequency bands associated with both regions of the brain and cognitive or behavioural characteristics.
Characterisations of ADHD are presented as disturbances in cortical arousal, executive function, and self-regulation. Theta/beta and theta/alpha waveform ratios (TBR) are considered a measure of differences in excess, slow-wave activity and epileptiform spike and wave activity [ 240 ], interpreted as abnormal brain processes indicating cortical under arousal, insufficient inhibitory control, and maturational delay in ADHD [ 241 ]; however recent studies have challenged TBR as a marker for ADHD diagnosis [ 235 ]. Sensory-motor rhythm (SMR) or low beta waveform ratios are thought to indicate cortical hypo-arousal, interpreted as deficiencies in the early stages of information processing [ 230 ]. Decreased contingent negative variation (CNV), a steady, slow, negative-going waveform associated with cognitive energy in anticipation of task performance, is considered indicative of dysfunctional regulation of energetical resources in ADHD [ 234 ].
Based on research in children, two treatment approaches reflect changes in the conceptualisation of ADHD and, therefore, treatment aims. Traditionally, the focus of treatment has been based on a “conditioning and repair model” [ 242 ]. Treatment aims to address dysfunctions and see behavioural improvement and remediation of symptoms following NF application [ 243 ]. Skill acquisition and learning are implicit, automatic, and unconscious. Changes in activity indicate positive results: the ability to decrease slow-wave activity (theta) and/or increase fast wave EEG activity (beta) should correlate with symptom improvement; or modulation of slow cortical potentials (SCP), changes of cortical electrical activity, indicate improved cortical regulatory processes [ 244 ]. The role of the therapist is to act as a model for affect regulation [ 236 ] as well as use behavioural principles such as operant conditioning (i.e., positive reinforcement) in the training process resulting in normalisation and stable change in resting EEG, or “EEG trait” [ 245 ], and behaviour [ 231 , 233 , 234 ].
More recently, the NF treatment focus has developed into a “skills acquisition model” [ 242 ]. Rather than simply improving neuropsychological deficits, it is thought that NF may be used as a tool for enhancing or optimising specific cognitive or attentional states [ 246 , 247 ]. This model recognises the bio-psycho-social model of neurodevelopmental disorders, characterising ADHD as impairments in attention, executive functions and self-regulation [ 229 , 230 ]. In this model, self-regulation, or neuro-regulation, is defined as explicit learning of controlled cognitive processes of cortical regulation evidenced by normalised shifts in EEG amplitudes [ 242 , 248 , 249 ]. Performance optimisation is evidenced by improved skill in changing the “EEG state” via self-initiated effort during task performance [ 243 , 250 ]. The therapist’s role is to use cognitive behavioural therapy elements such as positive feedback and coaching and operant procedures as active support within treatment sessions to enhance self-efficacy and self-confidence to support neuro-regulation [ 244 , 251 ]. Citations for characterisation of ADHD in NF models include two citations for DSM-IV-TR [ 231 , 238 ], two for DSM -V [ 232 , 233 ], one for Sonuga-Barke’s Delay Aversion Model [ 237 ], three for Sergeant’s Cognitive-Energic Model [ 230 , 234 , 237 ], and four citations for Barkley [ 118 , 229 , 237 , 239 ].
Transcranial stimulation . Four documents present Transcranial Stimulation as a treatment approach for ADHD. These include a systematic review [ 252 ], two randomised controlled trials of Transcranial Direct Stimulation (tDCS) [ 253 , 254 ], and a randomised controlled trial of Transcranial Magnetic Stimulation (rTMS) [ 255 ]. Both forms of transcranial stimulation conceptualise ADHD as a neurobiological disorder with deficits in executive functions, including attention, working memory, impulsivity, and inhibitory control. The treatment aims to increase cortical excitability in the area of stimulation, leading to improved neuropsychological and cognitive functions.
Treatment approaches are non-invasive but differ in their application. Transcranial Magnetic Stimulation uses a coil placed on the subjects head to deliver brief, intense pulses of current (up to 50 Hz) to generate a sizeable electromagnetic induction field initiating neurotransmitter release in the cortex and subcortical white matter of the brain [ 255 , 256 ]. Transcranial Direct Current Stimulation uses conductive sponge electrodes applied to the scalp in specific locations to deliver a weak electrical current (1–2 mA or milliamps) for up to 20 minutes. It is hypothesised that the electrical current changes the polarisation of the neurons, affecting their average level of discharge [ 253 , 254 , 256 ]. Multiple treatments are administered daily for 3–4 weeks. Protocols suggest two applications of stimulation: “online”, or while a patient is completing a task, or “offline” where the treatment is applied before or without specific targeted tasks. Citations for characterisation of ADHD in these models include DSM-IV [ 252 ], DSM-IV-TR [ 254 ], DSM V [ 255 ] and Barkley [ 253 ].
Hypnotherapy . Two RCTs examined hypnotherapy as a treatment approach for ADHD [ 74 , 257 ]. These studies conceptualise ADHD as a developmental neurobiological disability with deficits in attention, issues with hyperactivity/impulsivity and problems in executive function, including processing speed, regulating alertness, modulating emotions, and utilizing memory. Treatment aims to improve symptoms, mood, quality of life and cognitive performance. Treatment design is based on symptoms outlined in the DSM-IV and Brown’s Executive Dysfunction Model [ 258 ]. The therapist’s role was to follow a semi-structured manual to review the previous session, present the theme for the current session, perform induction and guided hypnotherapy with a post-hypnotic suggestion, and lead discussion. Treatment length was ten weekly sessions of 40 to 60 minutes. Citations for characterisation of ADHD were the DSM-IV [ 257 ] and Brown’s Executive Dysfunction Model [ 74 ].
Light therapy . Five documents present light therapy as a treatment approach for ADHD: a systematic review [ 259 ], an individual intervention [ 260 ], a quantitative study [ 261 ], a literature review [ 262 ], and treatment guidance [ 263 ]. These documents conceptualise ADHD as a neuropsychiatric disorder with primary symptoms of impulsivity, inattention, and hyperactivity impacted by mood regulation difficulties, maintaining arousal and sleep disturbances that contribute to pathophysiology. This conceptualisation is supported by links between ADHD, seasonal affective disorder (SAD) and circadian rhythms and highlighted by similarities in symptoms between sleep deprivation and ADHD [ 261 , 263 ]. Research indicates abnormalities in circadian related physiological measures such as heart rate increase relevant to autonomic function, dysregulation in melatonin rhythm leading to delays in melatonin onset, which may affect the modulation of the sleep/wake cycle [ 263 , 264 ], as well as some evidence of low cortisol impacting wakening times [ 259 ]. Also, a later diurnal preference, or evening chronotype, is highly prevalent in the ADHD population. Its association with shorter night sleep periods is believed to generate sleep debt, delay the sleep phase, and exacerbate symptoms or potentially play a causal role in ADHD symptoms [ 262 , 263 ].
Light Therapy (LT) treatment aims to assist with phase-shifting abnormal circadian rhythms through light exposure to achieve sleep onset to improve alignment with work, academic, or social norms. Treatment outcomes are improved sleep and improved ability to maintain effort, arousal and attention [ 260 , 262 ]. The treatment has been trialled as a three-week self-administered daily dose of 10,000 lux at a distance of 24 inches using a full-spectrum fluorescent lightbox [ 260 ]. Citations for the characterisation of ADHD in these documents include DSM-IV [ 260 ], DSM-V [ 259 ], Douglas [ 262 ], Brown’s Executive Dysfunction Theory [ 261 ], and Barkley [ 261 ].
Computer-based interventions . Eight documents presented computer-based interventions as a treatment approach for ADHD. These include randomised controlled trials [ 265 – 268 ], individual interventions [ 269 , 270 ], and case-control studies [ 271 , 272 ]. These approaches characterise ADHD as a neurobiological disorder with executive function deficits, including difficulties in sustained attention, response inhibition, goal persistence, and working memory. Computer-based interventions take two approaches: supportive or training. Supportive interventions aim to target specific symptoms and facilitate functioning via supportive software. Individuals are given access to tools used independently following training for a set timeframe. In Hecker et al. [ 271 ], a software tool designed to reduce internal and external distractions aimed to reduce effort and improve engagement, resulting in increased time reading and comprehension. In Irvine [ 269 ], a smartphone app for time management aimed to reduce the discrepancy between the perception of time and actual time spent by providing immediate real-time feedback on the current status and time use, leading to adjustments of future tasks according to behavioural therapeutic principles.
Training interventions aim to strengthen cognitive skills and/or remediate deficiencies via cognitive behavioural learning strategies of repetition and positive reinforcement. Working Memory Training [ 265 , 266 , 268 ] aimed to enhance auditory-verbal and visual-space working memory through intensive training with increasing task difficulty leading to improved cognitive and academic performance and attentional self-regulation. Cognitive ability training [ 272 ] aimed to improve cognitive skills of decision making, attention, organisation and time management through simulated activities in a gaming environment, providing immediate real-time rewards. Cognitive training for executive function [ 267 , 270 ] aimed to remediate cognitive processes deficiencies by repeated and graded exposure to neutral and universal stimuli and feedback. Training is self-administered, hierarchical and adjusted to individual performance with outcomes for improvements in daily executive functioning, occupational performance, and quality of life. Treatment length varied in frequency and intensity, from 20-minute sessions 3–5 times a week for 12 weeks to 45-minute sessions five days a week for five weeks and included weekly check-ins or supportive coaching. Citations for characterisation of ADHD in these approaches include DSM-IV [ 265 , 266 , 268 , 270 ], DSM V [ 271 ], Brown’s Executive Dysfunction Model [ 267 , 270 ], Nigg’s Integrative Theory [ 267 ], and Barkley [ 266 , 267 , 269 , 270 ].
Mentoring . One study presented mentoring as an individual intervention for ADHD [ 273 ]. Based in a university environment, ADHD is characterised as deficits in basic cognitive skills, such as attention, concentration, and memory and higher-level cognitive skills or “executive functioning”, such as planning, organization, judgment, problem-solving, and cognitive flexibility. These can negatively affect the university experience, as more independent self-management and a complex skill set are required for success, particularly time management and organization, academic skills, and social skills.
The mentoring program pairs second-year master’s level occupational therapy (MSOT) students (mentors) with undergraduate college students (mentees) for one-to-one support twice weekly for 2-hour sessions in the fall and spring semesters. This mentoring is a credit-bearing course that addresses skill development in time management and organization, academic skills, and social skills for college success. Mentees are graded on attendance, professional behaviours, compliance on a weekly to-do list, a presentation on academic resources, and a 4-part written paper on an academic skill. Mentors are participating as part of a professional Occupational Therapy training programme with an overall goal to facilitate student success in college, and if factors overwhelmingly interfere with this goal, to identify an alternate, suitable plan. As part of the training, mentors meet in discussion groups to brainstorm ways to overcome the mentoring process’s challenges. The citation for the characterisation of ADHD in this intervention is primarily the DSM V [ 273 ].
Self-monitoring . One study presented individual self-monitoring as an intervention for ADHD [ 274 ]. Based in a university environment, ADHD is characterised as a neurobehavioral disorder with symptoms of inattention, hyperactivity, and impulsivity, which increases the risk of academic failure or underachievement.
A checklist tool is co-designed and supported with integrity checks and email reminders every 2–4 days, with face-to-face check-in sessions every two weeks. The self-monitoring intervention aims to teach participants to observe and record behaviours to change the behaviour in the future. Outcomes are to obtain higher grades, endorse fewer ADHD symptoms, engage in more positive study skills, further attain goals, and improve medication adherence. Citations for characterisation of ADHD is DSM IV [ 274 ].
Binaural beat auditory stimulation . Two documents present binaural beat auditory stimulation as a treatment for ADHD. These include an individual intervention [ 275 ] and a literature review [ 276 ]. These approaches characterise ADHD as a disorder with core deficits in behavioural inhibition and sustained attention, highlighting a decrease in beta wave states interfering with maintenance of attention as a contributing factor.
Binaural beat auditory stimulation generates tones of two frequencies presented separately in each ear which are synthesised by the medulla into a single low-frequency tone. The pulse frequency from this binaural beat is the difference between the two tones and generates electrical activity that EEG can record. Treatment aims to match the difference between the tones to a particular brain-wave state, such as the beta range, which will correspondingly be maintained by overall brain activity and affect cognition levels [ 277 ]. Treatment involves exposure to auditory stimulus via headphones during an active task. Citations for characterisation of ADHD only directly reference Barkley [ 275 ].
Movement-related interventions . Twelve documents present movement-related interventions as a treatment for ADHD, including a systematic review [ 278 ], a pilot study [ 279 ], case-control studies [ 280 – 285 ], and treatment guidance [ 286 – 289 ]. In these approaches, ADHD is a disorder with core issues in special working memory, attention control, response inhibition, motor control, delay aversion, emotional self-regulation, and executive dysfunction. Movement-related interventions approach treatment in two ways: passive and active.
One document presented a passive intervention. Whole Body Vibration (WBV) devices deliver sinusoidal or oscillating wave vibrations at low frequencies to enhance mechanical muscular performance [ 290 ], improve balance and proprioception [ 291 ], and increase vigilance [ 292 ], potentially by inducing muscle contractions and increasing tension through the stretch reflex. Treatment is passive, delivered while sitting still, and aims to improve attention, inhibitory control, and cognitive performance in ADHD [ 280 ].
Active movement-related interventions aim to improve neurobiological factors such as increased cerebral blood flow, enhance neuroplasticity [ 288 , 289 ], assist the development of cortical and subcortical brain regions through activity [ 287 ], reduce the impact of comorbid anxiety, depression, stress and negative affect [ 279 , 288 ], and improve cognitive function and performance [ 282 – 286 ]. There is a specific focus on hypodopominergic functioning in ADHD and the upregulation of a brain-derived neurotrophic factor (BDNF) protein in several studies. [ 281 , 283 , 286 , 288 , 289 ]. Research shows that BDNF is linked to differentiation and survival of dopaminergic neurons, and decreased levels of BDNF have been suggested as being involved in ADHD pathology [ 293 ]. As well as improved cognition, one of the benefits of acute exercise is elevated levels of BDNF, which these models argue makes exercise an important intervention for ADHD. Treatment varies both in approach and length, from vigorous physical activity for 30 minutes, such as cycling, to fine motor movement stimulation using an anti-stress ball during a task. Citations for the characterisation of ADHD in these approaches include DSM IV [ 287 ], DSM V [ 285 ], Nigg [ 281 , 286 ], Sergeant [ 282 ], Sonuga-Barke [ 282 , 286 ], and Barkley [ 278 – 280 , 283 , 284 , 286 , 288 , 289 ].
Alternative models.
Psychoanalysis and Psychodynamic . There are very few studies in Psychoanalysis and Psychodynamic approaches for adult ADHD. A group intervention [ 294 ], single [ 295 , 296 ] or double case studies [ 297 – 299 ] were reviewed, as well as an evaluation study [ 300 ]. Much of the literature consists of literature reviews [ 35 , 301 – 304 ] and guidance pieces [ 152 , 305 , 306 ], which demonstrate considerable debate in the characterisation and aetiology of ADHD. Early papers reflect issues in clinical approaches by highlighting the importance of considering ADHD diagnosis as defined by DSM-IV in light of epidemiological evidence [ 301 , 307 ]. Both Psychoanalysis and Psychodynamic approaches present alternative models to Barkley, with distinct variation in characterisation.
Historically, Psychoanalysis does not recognise neurobiological deficits. Behaviours associated with ADHD are conceptualized as disturbances in the ego, identified as the organising force responsible for synthesis and integration of internal and external stimuli, internalisation of object relations and structure and development of the superego, and integral to facilitating the capacity for self-observation and self-reflection. Early presentations of these disturbances in childhood lead to attachment issues and interfere with sibling relationship development [ 301 ]. Behaviours are perceived as defence mechanisms, identified as an internal struggle for control [ 296 , 300 ]. Psychodynamic perspectives differ in that behaviours are conceptualized as a reaction to neurobiological deficits [ 152 , 302 , 306 ], facilitating engagement with Barkley’s model. Executive functioning deficits are presented as synonymous with self-regulation deficits, interfering with the development of personality structure and an internal representation of self about others. Self-regulation deficits disrupt the ability to empathise, which distorts the capacity to mentalise and develop a coherent sense of self [ 304 ].
The therapist’s role in these models is to act as the organising force for the client, assisting them to develop ego capacities via therapeutic relationship and transference. This enables the client to experience empathy, recognise mental states, and identify self in relation to others [ 35 , 301 , 304 ]. With the exception of the group intervention [ 294 ], treatment designs are intensive, up to four times a week [ 301 , 304 ] and long term, between 2 and 12 years [ 295 , 296 , 298 , 301 , 304 ]. Despite the alternative model to characterise ADHD, four studies reference international guidance [ 297 , 301 , 302 , 307 ], seven studies mention executive function or cognitive control [ 35 , 152 , 295 , 297 , 299 , 304 , 306 ], and seven reference Barkley specifically [ 35 , 294 , 295 , 297 – 299 , 304 ].
A review of 221 documents confirmed that treatment approaches for ADHD are based on a dominant cognitive behavioural paradigm for conceptualising ADHD, which attributes symptoms solely to neurobiological and developmental deficits leading to challenges with cognitive function, behavioural control, and management of self-regulation. This is reflected in descriptions of treatment aims, approaches and outcomes ( S1 Appendix ).
While this scoping review aimed for as broad a scope as possible, it is important to acknowledge the limitations of this study. First, while translation services were used as much as possible, the material identified in the results were primarily published in English. Further, the majority of the documents presented were published in the US, Canada and European countries. This may be due to documents being presented or published by journals not listed by the major search engines, and therefore not identified in the search strategies. Alternatively, there may not be a large existent body of published research in other countries, as the official diagnosis criteria for adults with ADHD was only recognised in 2013 [ 149 ]. Secondly, this scoping review was an enormous undertaking, and results are only up to date as of April 2020. However, searches did not reveal any other recent reviews of the theoretical charactarisation of ADHD, therefore it is believed this is the most current comprehensive scoping review on the topic.
This review reflects current research understanding that ADHD is complex and multidimensional in its presentation and impact. Clearly, it shows a broad, cross-disciplinary interest in developing treatment approaches to support individuals with ADHD to reduce symptoms, improve functioning and achieve a better quality of life. Critically, it highlights that a single theoretical perspective limits research into effective treatments for ADHD. Existing aetiological theories of ADHD have been challenged for their refutability [ 308 ], and other issues such as accounting for context variability, or inability to fully link or account for the full aspects of the symptomology [ 19 – 21 ], and heterogeneity [ 1 , 22 – 24 ] including specific links between domains and outcome [ 22 ] and cognition and motivation to select actions for a given context [ 309 ]. Recent recommendations for resolving challenges with heterogeneity in ADHD emphasise the importance of theoretical guidance in decision-making and recognise the critical role of beliefs, assumptions, and goals in preventing misapplication of conclusions to clinical circumstances or populations [ 1 ]. It is proposed that treatments based on approaches from a singular perspective on processes of self-regulation and a deficit-based origin of impairments in ADHD may be limited in scope and capacity to identify and support positive psychological factors for well-being and growth. Hence, the findings in this scoping review identify a gap in research and practice for alternative theoretical perspectives of ADHD.
This review concludes that further research into additional theoretical models of self-regulation would provide opportunities to develop alternative treatment approaches and benefit research and understanding of the symptomology of ADHD.
Supporting information
S1 appendix. analysis of treatment approaches..
https://doi.org/10.1371/journal.pone.0261247.s001
S1 File. PRISMA scoping review checklist.
https://doi.org/10.1371/journal.pone.0261247.s002
- View Article
- Google Scholar
- PubMed/NCBI
- 6. Barkley RA. Executive functions: What they are, how they work, and why they evolved. New York, NY: Guildford Press; 2012.
- 7. Brown TE. A new understanding of ADHD in children and adults: Executive function and impairments. New York, NY: Routledge; 2013.
- 8. Ramsay JR. Rethinking adult ADHD. Washington D.C.: American Psychological Association; 2020.
- 11. Barkley RA. ADHD and the nature of self control. London: Guildford Press; 1997.
- 18. NICE, editor. Attention deficit hyperactivity disorder: diagnosis and management. In National Institute for Health Care and Excellence; 2019. Available from: https://www.nice.org.uk/guidance/cg72
- 19. Brown TE. Differential diagnosis of ADD versus ADHD in adults. In: Nadeau KG, editor. A comprehensive guide to attention deficit disorder in adults. New York: Brunner/Mazel Inc.; 1995. p. 93–108.
- 20. Brown TE. Smart but stuck: Emotions in teens and adults with ADHD. San Francisco: Jossey-Bass; 2014.
- 26. Liberman RP. Recovery from disability: Manual of psychiatric rehabilitation. Arlington, VA: American Psychiatric Publishing, Inc.; 2008.
- 30. Aromataris E, Munn Z. Johanna Briggs Institute reviewer’s manual. The Joanna Briggs Institute. 2017.
- 31. Hartmann T, Popkin M. ADHD: a hunter in a farmer’s world. Rochester, Vermont: Healing Arts Press; 2019.
- 32. Weiss L. Embracing ADHD: A healing perspecive. Lanham, MD: Taylor Trade Publishing; 2015.
- 33. Maté G. Scattered minds: The origin and healing of Attention Deficit Disorder. London, UK: Vermilion; 1999.
- 34. Amen D. Healing ADD: The breakthrough program that allows you to see and heal the 7 types of Attention Deficit Disorder. New York, NY: Berkley Publishing Group; 2013.
- 55. Wood RL. Head trauma rehabilitation: A neurobehavioural approach. London: Croom Helm; 1987.
- 56. Jordan DR. Attention Deficit Disorder: ADHD and ADD syndromes. Third. Austin, TX: Pro-Ed; 1998.
- 58. Yankura J, Dryden W. Using REBT with common psychological problems: A therapist’s casebook. New York: Springer Publishing Co.; 1997.
- 59. Barkley RA. Attention deficit hyperactivity disorder: a handbook for diagnosis and treatment. New York: Guildford Press; 1990.
- 60. American Psychiatric Association. The diagnostic and statistical manual of mental disorders. 4th ed. Washington D.C.: American Psychiatric Association; 1994.
- 61. Douglas VI. Higher mental processess in hyperactive children: implications for training. In: Knights RM, Bakker DJ, editors. Treatment of hyperactive and learning disordered children. Baltimore: University Park Press; 1980. p. 65–92.
- 108. Safren SA, Perlman C, Sprich S, Otto M. Mastering your adult ADHD. New York: Oxford University Press; 2005.
- 111. Young S, Bramham J. ADHD in adults: a psychological guide to practice. Chichester, West Sussex: John Wiley & Sons, Inc; 2007.
- 112. Young SJ, Ross RR. R&R2 for ADHD youths and adults: a prosocial competence training program. Ottawa, Canada: Cognitive Centre of Canada; 2007.
- 118. Ramsay JR. Nonmedication treatments for adult ADHD. Washington D.C.: American Psychological Association; 2010.
- 121. Young S, Bramham J. Cognitive-behavioural therapy for ADHD in adolescents and adults: A psychological guide to practice. 2nd ed. Chichester, West Sussex: Wiley-Blackwell; 2012.
- 122. Knouse LE. Cognitive behavioural therapies for ADHD. In: Barkley RA, editor. Attention deficit hyperactivity disorder: A handbook for diagnosis and treatment. 4th ed. New York: Guilford Press; 2014. p. 757–94.
- 125. Jeavons A, Bishop T, French B, Bastable S, Harpham-Salter A. The adult ADHD treatment handbook. Abington, Oxon: Routledge; 2018.
- 128. Nadeau K. The clinician’s role in the treatment of ADHD. In: Goldstein S, Ellison AT, editors. Clinician’s guide to adult ADHD: assessment and intervention. San Diego, CA: Academic Press; 2002. p. 107–26.
- 129. Nadeau KG. Life management skills for the adult with ADHD. In: Nadeau KG, editor. A comprehensive guide to attention deficit disorder in adults. New York, NY: Brunner/Mazel Inc.; 1995. p. 191–217.
- 130. Murphy K. Empowering the adult with ADHD. In: Nadeau KG, editor. A comprehensive guide to attention deficit disorder in adults. New York, NY: Brunner/Mazel Inc.; 1995. p. 135–45.
- 135. Young S. A model of psychotherapy for adults with ADHD. In: Goldstein S, Ellison T, editors. Clinician’s guide to adult ADHD: assessment and intervention. San Diego, CA: Academic Press; 2002. p. 147–63.
- 136. McDermott S. Cognitive Therapy for adults with attention-deficit/hyperactivity disorder. In: Brown TE, editor. Attention-deficit disorders and comorbidities in children, adolescents, and adults. Arlington, VA: American Psychiatric Publishing, Inc.; 2000. p. 569–606.
- 137. Murphy K. Psychological counselling of adults with ADHD. In: Barkley RA, editor. Attention deficit hyperactivity disorder: a handbook for diagnosis and treatment. 3rd ed. New York, NY: Guildford Press; 2006.
- 138. Brooks RB. Changing the mindset of adults with ADHD: strategies for fostering hope, optimism, and resilience. In: Goldstein S, Ellison AT, editors. Clinician’s guide to adult ADHD: assessment and intervention. San Diego, CA: Academic Press; 2002. p. 127–46.
- 143. Hallowell E, Ratey J. Driven to distraction. New York: Touchstone; 1994. https://doi.org/10.1080/14640749408401099 pmid:7809399
- 145. Ramsay JR, Rostain AL. The adult ADHD toolkit. New York: Routledge; 2015.
- 148. American Psychiatric Association [APA]. The diagnostic and statistical manual of mental disorders. IV-TR. Washington D.C.: American Psychiatric Publishing, Inc.; 2000.
- 149. American Psychiatric Association [APA]. The diagnostic and statistical manual of mental disorders. 5th ed. Washington D.C.: American Psychiatric Association; 2013.
- 150. Solanto M V. Cognitive-behavioural therapy for adult ADHD. New York: Guildford Press; 2010.
- 157. Fleming AP, Fleming AP. Randomized controlled trial of group cognitive-behavioral therapy for ADHD among college students. University of Washington; 2013.
- 162. Linehan MM. Cognitive-behavioural treatment of borderline personality disorder. 14th ed. New York: Guildford Press; 1993.
- 163. Hartmann T. ADD: a different perception. Grass Valley, California: Underwood Books; 1997.
- 164. Wender PH. Attention deficit hyperactivity disorder in adults. New York: Oxford University Press; 1995.
- 182. Zylowska L. The mindfulness prescription for adult ADHD. Boulder, CO: Trumpeter; 2012.
- 189. Reaser AL. ADHD coaching and college students. Florida State University; 2008. https://doi.org/10.1111/j.1863-2378.2008.01123.x pmid:18399943
- 191. Farmer JL. The development of the Personal Strengths Intervention (PSI) to improve self- determination and social-emotional levels in postsecondary students with learning disabilities and/or ADHD: A multiple baseline study. [Internet]. Available in ProQuest Dissertations and Theses database. (UMI No. 3466210). 2011. Available from: http://search.ebscohost.com.proxy-ub.rug.nl/login.aspx?direct=true&db=psyh&AN=2012-99070-067&site=ehost-live&scope=site
- 195. Bomar R. The role of online academic coaching on levels of self-determination of college students with learning disabilities. Texas Woman’s University; 2017.
- 210. Nadeau KG. Non-medication treatments for women with ADHD: working with coaches and organizers. In: Nadeau KG, Quinn P, editors. Understanding women with ADHD. Washington D.C.: Advantage Books; 2002. p. 124–32.
- 211. Jaksa P, Ratey N. Therapy and ADD coaching: similarities, differences, and collaboration [Internet]. 1999 [cited 2016 Feb 7]. p. http://www.nancyratey.com/adhdcoaching/therapy-add . Available from: http://www.nancyratey.com/adhdcoaching/therapy-addcoaching
- 212. Quinn P, Ratey N, Maitland TL. Coaching college students with ADHD. Silver Spring, MD: Advantage Books; 2000.
- 213. Ratey N. Life coaching for adult ADHD. In: Goldstein S, Ellison AT, editors. Clinician’s guide to adult ADHD: assessment and intervention. San Diego, CA: Academic Press; 2002. p. 261–77.
- 217. Bowles VM. A survey of the methods and processes involved in interventions with ADHD clients from a psychologist and ADHD coach perspective. Florida State University; 2012.
- 218. Wright SD. ADHD coaching matters: the definitive guide. College Station, TX: ACO Books; 2014.
- 220. Wehmeyer ML, Field S. Self-Determination: instructional and assessment strategies. Thousand Oaks, CA: Corwin Press; 2007.
- 222. Mithaug DE, Wehmeyer ML, Agran M, Martin JE, Palmer S. The self-determined learning model of instruction: Engaging students to solve their learning problems. In: Wehmeyer ML, Sands DJ, editors. Making it happen: student involvement in educational planning, decision-making and instruction. Baltimore: Paul H. Brookes; 1998. p. 299–328.
- 223. Agran M, Martin JE. Applying a technology of self-control in community environments for individuals who are mentally retarded. In: Hersen M, Eisler RM, Miller PM, editors. Progress in behavior modification. Newbury Park, CA: SAGE; 1987. p. 108–51. pmid:3588360
- 224. Kanfer R, Goldstein AP. Helping people change: A textbook of methods. New York: Pergamon Press; 1986.
- 225. Bandura A. Social foundations of thought and action: a social cognitive theory. Englewood Cliffs: Prentice-Hall; 1986.
- 226. Martin JE, Burger D, Elias-Burger S, Mithaug DE. Applications of self-control strategies to facilitate independence in vocational and instructional settings. In: Bray NW, editor. International review of research in mental retardation. San Diego: Academic Press; 1988. p. 155–93.
- 258. Brown TE. Attention deficit disorder: The unfocused mind in children and adults. New Haven, CT: Yale University Press; 2005.
- 269. Irvine MJD. Outcome evaluation of a time management smartphone application: a pilot study [Internet]. George Fox University; 2013. Available from: http://digitalcommons.georgefox.edu/psyd/118
- 276. Peterson O. Rhythm as an intervention for health and mental health difficulties: a comprehensive literature review. Doctoral Thesis. Alliant International University; 2012.
Log in using your username and password
- Search More Search for this keyword Advanced search
- Latest content
- Topic collections
- BMJ Journals
You are here
- Volume 21, Issue 4
- Twenty years of research on attention-deficit/hyperactivity disorder (ADHD): looking back, looking forward
- Article Text
- Article info
- Citation Tools
- Rapid Responses
- Article metrics
- Samuele Cortese 1 , 2 , 3 , 4 , 5 ,
- David Coghill 6 , 7 , 8
- 1 Academic Unit of Psychology, Center for Innovation in Mental Health , University of Southampton , Southampton , UK
- 2 Clinical and Experimental Sciences (CNS and Psychiatry), Faculty of Medicine , University of Southampton , Southampton , UK
- 3 Solent NHS Trust , Southampton , UK
- 4 New York University Child Study Center , New York City , New York , USA
- 5 Division of Psychiatry and Applied Psychology, School of Medicine , University of Nottingham , Nottingham , UK
- 6 Departments of Paediatrics and Psychiatry, Faculty of Medicine, Dentistry and Health Sciences , University of Melbourne , Melbourne , Victoria , Australia
- 7 Murdoch Children’s Research Institute , Melbourne , Victoria , Australia
- 8 Royal Children’s Hospital , Melbourne , Victoria , Australia
- Correspondence to Dr Samuele Cortese, Academic Unit of Psychology and Clinical and Experimental Sciences (CNS and Psychiatry), University of Southampton, Southampton SO17 1BJ, UK; samuele.cortese{at}gmail.com
In this clinical review we summarise what in our view have been some the most important advances in the past two decades, in terms of diagnostic definition, epidemiology, genetics and environmental causes, neuroimaging/cognition and treatment of attention-deficit/hyperactivity disorder (ADHD), including: (1) the most recent changes to the diagnostic criteria in the Diagnostic and Statistical Manual of Mental Disorders and International Classification of Diseases; (2) meta-analytic evidence showing that, after accounting for diagnostic methods, the rates of ADHD are fairly consistent across Western countries; (3) the recent finding of the first genome-wide significant risk loci for ADHD; (4) the paradigm shift in the pathophysiological conceptualisation of ADHD from alterations in individual brain regions to a complex dysfunction in brain networks; (5) evidence supporting the short-term efficacy of ADHD pharmacological treatments, with a different profile of efficacy and tolerability in children/adolescents versus adults; (6) a series of meta-analyses showing that, while non-pharmacological treatment may not be effective to target ADHD core symptoms, some of them effectively address ADHD-related impairments (such as oppositional behaviours for parent training and working memory deficits for cognitive training). We also discuss key priorities for future research in each of these areas of investigation. Overall, while many research questions have been answered, many others need to be addressed. Strengthening multidisciplinary collaborations, relying on large data sets in the spirit of Open Science and supporting research in less advantaged countries will be key to face the challenges ahead.
https://doi.org/10.1136/ebmental-2018-300050
Statistics from Altmetric.com
Request permissions.
If you wish to reuse any or all of this article please use the link below which will take you to the Copyright Clearance Center’s RightsLink service. You will be able to get a quick price and instant permission to reuse the content in many different ways.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is the most common neurodevelopmental disorder in children, with an estimated worldwide prevalence around 5%. 1 Although it has for a long time been considered a childhood disorder, it is now established that impairing ADHD symptoms persist in adulthood in a sizeable portion of cases (around 65%), 2 although there is variability in the estimate due to methodological heterogeneity across studies. 3
As for other mental health conditions there has, over the past two decades, been an increasing body of research on ADHD. Reasons for this increase include: increased recognition of the impact of ADHD on functioning; advances in research methodology and technology; and interest from pharmaceutical companies.
Here, we provide an overview of what we deem have been some the most important advances, in the past two decades, in ADHD research. We also discuss key areas for future research.
Given the large body of literature and space constraints, this review is selective rather than systematic and comprehensive. We relied mostly on meta-analyses, retrieved with a search in PubMed using the following syntax/terms (update: 8 August 2018): (ADHD OR Attention Deficit OR Hyperkinetic Disorder) AND (meta-analy* OR metaanaly).
Presentation
Diagnostic definition.
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), 4 published in 2013, introduced several significant changes in relation to the DSM Fourth Edition Text Revision (DSM-IV-TR) 5 criteria. First, the threshold in the number of symptoms (criterion A) necessary for the diagnosis in older adolescents and adults was reduced from 6 to 5. This change is in keeping with the notion that, despite a reduction in the number of symptoms over development, adults with ADHD in childhood can still present with impairment. 2 The required age of onset was increased from ‘prior to 7’ to ‘prior to 12’. The purpose of these changes was well intended and designed to facilitate the diagnostic process in adults, who often have trouble pinpointing the exact age of onset, especially if early in the development. Unfortunately, neither change was based on empirical evidence, and methods used for diagnostic ascertainment in adults are still under debate. 3 Another pivotal change in DSM-5 is the removal of the veto around the dual diagnosis of ADHD and autism spectrum disorders (ASD) that was present in previous editions of the DSM. Unlike the age of onset and symptom number changes this change is supported by a significant body of research (see ref 6 ). Finally, the (sub)types of ADHD defined in the DSM-IV-(TR) were replaced by the notion of different presentations. This acknowledges the instability in the phenotypic manifestation of inattention or hyperactive/impulsive symptoms over time, 7 in contrast to the more static notion of a subtype.
With regard to the International Classification of Diseases (ICD), it appears that the veto to diagnose ASD in the presence of ADHD will be retained in the upcoming ICD 11th Revision ( https://icd.who.int/browse11/l-m/en#/http%3a%2f%2fid.who.int%2ficd%2fentity%2f821852937 ).
Overall, while these changes to a degree reflect recent empirical evidence and/or practical needs in the diagnostic process, there are still issues that need to be addressed. First, current criteria still focus on the number of symptoms rather than on a more precise definition of functional impairment. This should be a priority for the field and efforts, such as the development of the International Classification of Functioning, Disability and Health: Child and Youth version, are already ongoing. 8 Second, while currently each of the symptoms listed in the DSM criterion A carries the same weight, it has been argued that inattention should be more heavily weighted than hyperactivity/impulsivity. 9 Supporting evidence, which comes from clinical samples, needs to be replicated in population-based studies. Third, from a practical standpoint, it is unclear on how to best integrate different information sources (eg, parents, teachers, etc). Addressing this challenge is pivotal. Fourth, although proposed as a separate type of ADHD or even a separate diagnostic entity, the extent to which the construct of sluggish cognitive tempo (impairment of attention in hypoactive-appearing individuals) overlaps with ADHD inattentive presentation remains still unclear. 10 11 Finally, one of the most controversial topics in the entire field of ADHD research is currently around the possibility that ADHD can emerge de novo in adulthood, in contrast to its conceptualisation as a neurodevelopmental disorder. Despite an increasing number of important studies, the controversy is far from being solved 12 and we expect it will be a major focus of research in the field in coming years.
We also expect that proposed radical, although controversial, changes in the nosographic approach to mental health conditions, such as the Research Domain Criteria will significantly influence future research on ADHD. 13
Epidemiology
One of the most controversial questions in relation to the epidemiology of ADHD has been around possible differences in the prevalence of the disorder in different countries. In particular, the differential rates of clinical diagnosis in North America and Europe are cited by detractors of ADHD, as supporting the notion that ADHD is not a ‘real’ disorder but rather a social construct. 14 However, a meta-analysis published in 2007 1 found that diagnostic criteria, source of information, requirement of impairment for diagnosis and geographic origin of the studies significantly impacted on the estimated pooled rate of ADHD (5.29%). A significant difference in prevalence emerged only between North America and both Africa and the Middle East, although evidence from non-Western countries was limited. However, as there were only a limited number of studies available for Africa and Middle East, these findings should be considered with caution. By contrast, no significant differences emerged between Europe and North America, suggesting that when using the same diagnostic approach the rates of the disorder are fairly consistent in Western countries, with variability in the prevalence accounted for primarily by methods used to diagnose ADHD. Another more recent meta-analysis 15 found no evidence to support an increase in the epidemiological prevalence of ADHD over the past three decades when standardised diagnostic procedures are followed. This implies that the trend for increased rates of diagnosis 16 are not accounted for by actual increases in prevalence. Rather, the mismatch between administrative and epidemiological rates of the disorder, which varies between the USA and Europe, is likely accounted for by cultural and social factors. 16
As the bulk of the available epidemiological studies focus on school-age children from North America and Europe, further population-based studies from other continents as well as in preschoolers and adults should be encouraged. Additionally, longitudinal epidemiological studies aimed at better understanding the developmental trajectories and predictors of remission/persistence of ADHD in adulthood will be instrumental, alongside other clinical, neuropsychological, genetic and neuroimaging studies, to inform prevention programmes. Development of a standardised definition of caseness and remission will be pivotal for this body of research to be fruitful.
Genetics and environmental causes of ADHD
Studies of twins and adopted children indicate a high heritability for ADHD (60%–90%). 17 Efforts to find the genes underpinning this heritability have been more challenging than initially anticipated. As for other mental health conditions, it became clear that ADHD aetiology is accounted for by a complex interaction of many genes each with a relatively small effect and by gene × environment interactions. 18
The first approach to finding the genes involved in ADHD was the ‘candidate gene’ approach. This approach focuses on identifying the variants in genes coding for proteins hypothesised, a priori, to be involved in the pathophysiology of ADHD. These studies identified only about 10 genes as having significant support, 19 which together accounted for only a small fraction of the total ADHD heritability. The next major approach, ‘genome-wide association studies’ (GWAS), which allows the analysis of a large number of common (ie, present at greater than 5% frequency in the population) single-nucleotide polymorphisms across the entire genome, was initially unsuccessful in ADHD, as the available sample was too small to show a meaningful effect. However, in a major breakthrough, the first 12 independent loci have been recently identified through GWAS. 20 Associations were enriched in loss-of-function intolerant genes and brain-expressed regulatory marks, paving the way for a number of novel lines of investigation on the neurobiology of ADHD.
A further recently developed approach focuses on rare (ie, a frequency in the general population below 1%) ‘copy number variants’ (CNV). These are defined as replications or deletions of the DNA with a length of at least 1 kb. CNVs over-represented in ADHD have been detected, but their contribution can so far only explain 0.2% of ADHD heritability. 21
As for environmental aetiological factors, there have been, over the past years, considerable data suggesting that prenatal and postnatal factors, such as maternal smoking and alcohol use, low birth weight, premature birth and exposure to environmental toxins, such as organophosphate pesticides, polychlorinated biphenyls and zinc, are associated with increased risk for ADHD. 17 22 However, except for preterm birth, genetics studies have implicated unmeasured familial confounding factors, which are not in line with a causal role of environmental factors. 23
Severe maternal deprivation has also been related to the development of ADHD-like symptoms. 24
The study of the causes of ADHD still has many unanswered questions. We need a better understanding of how genes interact with each other, and of the interplay between environmental factors and genes. Genetics has the potential to offer many other exciting future avenues of research in ADHD. We will only mention briefly here: (1) the use of induced pluripotent stem cell derived from peripheral tissue of patients with ADHD and used to generate brain cells with the aim to model brain circuits and responses to medications or other stressors; (2) the use of zebrafish and fruit fly models to augment currently available animal models of ADHD.
Neuroimaging and neurocognition
Initial pathophysiological models of ADHD published 20 years ago 25 were based on dysfunctions in a limited number of brain areas, namely the frontal cortex and the basal ganglia. Over the past two decades, and similar to other mental health conditions, a major paradigm shift from alterations in individual brain regions to dysfunction in brain networks has begun to reshape our understanding of the pathophysiology of ADHD. Structurally, meta-analyses and mega-analyses of the structural MRI studies conducted over the past two decades pointed to consistently replicated alterations in the basal ganglia, 26 and in a number of other subcortical areas. 27 Functionally, a comprehensive meta-analysis 28 found that the majority of the ADHD-related hypoactivated areas were related to the ventral attention and the frontoparietal networks. By contrast, the majority of ADHD-related hyperactivated areas fell within the default mode network and other hyperactivated areas were within the visual network. This is in line with the hypothesis that the attentional lapses that characterise ADHD result from an inappropriate intrusion of the default network in the activity of task-positive networks frontoparietal, ventral or dorsal attention networks, 28 according to the default network hypothesis of ADHD , 29 which has been arguably one of the most inspiring proposals in the neuroscience of ADHD over the past two decades.
While we have gained insight into the brain networks that are dysfunctional in ADHD and in the delay in cortical maturation, 30 we look forward to the next generation of neuroimaging studies which we hope will start to translate these findings into the clinical practice. The introduction of machine learning approaches, such as support vector machine, has been welcomed in the field of clinical neuroscience as a way to translate neuroscientific findings at the individual patient level, thus overcoming the main limitation of current studies that can only provide results valid at the group, rather than individual, level. 31 An increasing number of studies have used machine learning based on MRI data to validate the diagnosis of ADHD with varying degrees of success. 32 33
Neurocognitive studies have made a considerable contribution to our understanding of ADHD. In recent years, the field has moved away from linear single-cause models of ADHD towards multipathway models that emphasise the heterogeneity inherent to ADHD and provide a link between individual differences at the brain level and clinical presentation. 34 35
We believe that an interesting line of research for the future will be to combine genetics, clinical, neurocognitive and neuroimaging data to define, via machine learning approaches, response to treatment, tolerability profiles and functional trajectory of the disorder over time. This will be a crucial step towards personalised and precision approaches to treatment.
Over the past two decades, there has been a marked increase in the number of randomised controlled trials (RCT) aimed at testing the short-term efficacy and tolerability of pharmacological treatments for ADHD (both stimulant and non-stimulant medications). Most have been sponsored by Big Pharma and were designed to support the licence of the medication. In parallel, due to concerns around possible side effects of medications and lack of clarity around their long-term effects, several lines of research on non-pharmacological interventions have been developed. Recent important methodologically sound meta-analyses allow us to summarise and critically discuss this large body of evidence.
For the pharmacological interventions, a comprehensive network meta-analysis 36 of 133 double-blind RCTs demonstrated high to moderate effect sizes (in terms of efficacy) for the different medications versus placebo. Standardised mean differences (SMD) ranged from −1.02 (95% CI −1.19 to −0.85) for amphetamines to −0.56 (95% CI −0.66 to −0.45) for atomoxetine (methylphenidate: −0.78, 95% CI −0.93 to −0.62). In children/adolescents, methylphenidate was the only drug with better acceptability than placebo; in adults this was the case only for amphetamines (with no difference between placebo and other active drugs). Taking into account both efficacy and safety, evidence from this meta-analysis supported methylphenidate as preferred first-choice medication for the short-term treatment of ADHD in children/adolescents and amphetamines for adults.
As for non-pharmacological options, a comprehensive synthesis on non-pharmacological treatments for children and adolescents with ADHD has been provided in a series of meta-analyses by the European ADHD Guidelines Group (EAGG). In 2013, they published a first systematic review/meta-analysis 37 addressing the efficacy of behavioural interventions, diet interventions (restricted elimination diets, artificial food colour exclusions and free fatty acid supplementation), cognitive training and neurofeedback on ADHD core symptoms (ie, inattention, hyperactivity and impulsivity). The systematic review included only RCTs and considered two contrasting outcomes: those rated by individuals not blinded to the treatment condition (active vs control) and those rated by individuals who were probably blinded to treatment (eg, teachers in trials assessing a behavioural intervention implemented with parents). The results were strikingly different depending on the type rater. When considering not blinded ratings, all interventions resulted significantly more efficacious than the control condition in terms of reduction of ADHD core symptoms. However, when considering the more rigorous probably blinded ratings, only free fatty acid supplementation and artificial food colour exclusion remained significantly more efficacious than the control conditions, with small effect sizes (SMD=0.16 and 0.42, respectively), indicating that the clinical impact of these treatments on ADHD core symptoms is, at the group level, modest.
Subsequent EAGG meta-analyses focused on ADHD core symptoms and on ADHD-related problems. A meta-analysis 38 specifically focusing on behavioural interventions showed that, even when considering probably blinded ratings, the behavioural interventions were efficacious at improving important aspects related to ADHD, namely parenting (SMD for positive parenting 0.63; SMD for negative parenting 0.43) and conduct problems (SMD 0.31). Another updated meta-analysis 39 on cognitive training, which was found efficacious in improving verbal and visual working memory, which are impaired in a sizeable portion of children with ADHD and have been demonstrated to dissociate from ADHD symptoms. 40 These meta-analyses also suggest that training which targets several neuropsychological aspects may be more efficacious at improving ADHD symptoms, than training targeting only one aspect of cognitive functioning. The most recent meta-analysis 41 by the EAGG on neurofeedback did not provide support for the efficacy of neurofeedback on any of the neuropsychological and academic outcomes. Overall, this body of research does not provide solid evidence to routinely recommend non-pharmacological interventions as highly effective treatments for ADHD core symptoms, although some of them (eg, behavioural interventions or cognitive training) may be effective for important associated impairments (oppositional behaviours and working memory deficits, respectively). The role of fatty acid supplementation and artificial food colours exclusion as possible treatment strategies should be considered cautiously given the small effect size, with CIs close to non-significance.
Probably, the most crucial area of future treatment research in ADHD will be to gain insight into the long-term positive and negative effects of treatments, using randomised trials with withdrawn designs, as well as additional population-based studies with self-controlled methodologies and longitudinal follow-up studies. These should clarify the conclusions from the various follow-up waves of the Multimodal Treatment of ADHD (MTA) study, showing that neither the type and intensity of treatment received during the initial 15-month randomised phase of the study (treatment as usual medication (MED), behavioural therapy (BEH), medication plus behavioural therapy (COMB)) nor exposure to medication over the subsequent observational periods predicted the functional outcome at follow-up which has now extended to 16 years. Of note, in the MTA, the treatments received in the three experimental arms (MED, BEH, COMB) during initial 15-month randomised phase were carefully crafted in an attempt to achieve optimal outcomes. After this initial phase all participants were free to choose the type of treatment they received from their regular provider. As it is likely that these treatments were not as carefully optimised and monitored as the three experimental groups during the randomised phase, these longer term findings of the MTA are not easily interpretable and might be, to some extent, misleading.
Conclusions
Many questions have been successfully answered in the field of ADHD. Many others remain to be addressed. Additional multidisciplinary collaborations, use of large data sets in the spirit of Open Science and support of research activities in less advantaged countries are key to address the challenge.
- Polanczyk G ,
- de Lima MS ,
- Horta BL , et al
- Faraone SV ,
- Biederman J ,
- Sibley MH ,
- Mitchell JT ,
- 4. ↵ American Psychiatric Association . Diagnostic and statistical manual of mental disorders, DSM-5 . Fifth edn . American Psychiatric Publishing , 2013 .
- 5. ↵ American Psychiatric Association . Diagnostic and statistical manual of mental disorders . Fourth edn : American Psychiatric Publishing , 2000 .
- Visser JC ,
- Rommelse NN ,
- Greven CU , et al
- Willcutt EG ,
- Pennington BF , et al
- Coghill D , et al
- Sokolova E ,
- Claassen T , et al
- Becker SP ,
- Leopold DR ,
- Burns GL , et al
- Agnew-Blais J ,
- Arseneault L
- Peterson BS
- Sergeant J ,
- Gillberg C , et al
- Polanczyk GV ,
- Salum GA , et al
- Daley D , et al
- Asherson P ,
- Banaschewski T , et al
- Cummins TD ,
- Tong J , et al
- 20. ↵ Discovery Of The First Genome-Wide Significant Risk Loci For ADHD . https://www.biorxiv.org/content/early/2017/06/03/145581
- Hohmann S ,
- Lahey BB , et al
- Sciberras E ,
- Mulraney M ,
- Silva D , et al
- Stevens SE ,
- Sonuga-Barke EJ ,
- Kreppner JM , et al
- Castellanos FX
- Rubia K , et al
- Hoogman M ,
- Bralten J ,
- Hibar DP , et al
- Cortese S ,
- Chabernaud C , et al
- Eckstrand K ,
- Sharp W , et al
- Pettersson-Yeo W ,
- Marquand AF , et al
- Johnston BA ,
- Matthews K , et al
- Coghill DR ,
- Del Giovane C , et al
- Brandeis D ,
- Cortese S , et al
- van der Oord S ,
- Ferrin M , et al
- Brandeis D , et al
- Rhodes SM ,
Contributors SC drafted the paper. DC revised the first draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests SC declares reimbursement for travel and accommodation expenses from the Association for Child and Adolescent Central Health (ACAMH) in relation to lectures delivered for ACAMH, and from Healthcare Convention for educational activity on ADHD. DC declares grants and personal fees from Shire and Servier; personal fees from Eli Lilly, Novartis and Oxford University Press; and grants from Vifor.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Read the full text or download the PDF:

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
- My Bibliography
- Collections
- Citation manager
Save citation to file
Email citation, add to collections.
- Create a new collection
- Add to an existing collection
Add to My Bibliography
Your saved search, create a file for external citation management software, your rss feed.
- Search in PubMed
- Search in NLM Catalog
- Add to Search
Twenty years of research on attention-deficit/hyperactivity disorder (ADHD): looking back, looking forward
Affiliations.
- 1 Academic Unit of Psychology, Center for Innovation in Mental Health, University of Southampton, Southampton, UK.
- 2 Clinical and Experimental Sciences (CNS and Psychiatry), Faculty of Medicine, University of Southampton, Southampton, UK.
- 3 Solent NHS Trust, Southampton, UK.
- 4 New York University Child Study Center, New York City, New York, USA.
- 5 Division of Psychiatry and Applied Psychology, School of Medicine, University of Nottingham, Nottingham, UK.
- 6 Departments of Paediatrics and Psychiatry, Faculty of Medicine, Dentistry and Health Sciences, University of Melbourne, Melbourne, Victoria, Australia.
- 7 Murdoch Children's Research Institute, Melbourne, Victoria, Australia.
- 8 Royal Children's Hospital, Melbourne, Victoria, Australia.
- PMID: 30301823
- PMCID: PMC10270437
- DOI: 10.1136/ebmental-2018-300050
In this clinical review we summarise what in our view have been some the most important advances in the past two decades, in terms of diagnostic definition, epidemiology, genetics and environmental causes, neuroimaging/cognition and treatment of attention-deficit/hyperactivity disorder (ADHD), including: (1) the most recent changes to the diagnostic criteria in the Diagnostic and Statistical Manual of Mental Disorders and International Classification of Diseases; (2) meta-analytic evidence showing that, after accounting for diagnostic methods, the rates of ADHD are fairly consistent across Western countries; (3) the recent finding of the first genome-wide significant risk loci for ADHD; (4) the paradigm shift in the pathophysiological conceptualisation of ADHD from alterations in individual brain regions to a complex dysfunction in brain networks; (5) evidence supporting the short-term efficacy of ADHD pharmacological treatments, with a different profile of efficacy and tolerability in children/adolescents versus adults; (6) a series of meta-analyses showing that, while non-pharmacological treatment may not be effective to target ADHD core symptoms, some of them effectively address ADHD-related impairments (such as oppositional behaviours for parent training and working memory deficits for cognitive training). We also discuss key priorities for future research in each of these areas of investigation. Overall, while many research questions have been answered, many others need to be addressed. Strengthening multidisciplinary collaborations, relying on large data sets in the spirit of Open Science and supporting research in less advantaged countries will be key to face the challenges ahead.
© Author(s) (or their employer(s)) 2018. No commercial re-use. See rights and permissions. Published by BMJ.
PubMed Disclaimer
Conflict of interest statement
Competing interests: SC declares reimbursement for travel and accommodation expenses from the Association for Child and Adolescent Central Health (ACAMH) in relation to lectures delivered for ACAMH, and from Healthcare Convention for educational activity on ADHD. DC declares grants and personal fees from Shire and Servier; personal fees from Eli Lilly, Novartis and Oxford University Press; and grants from Vifor.
- Attention-deficit/hyperactive disorder: missing the bull's eye. Leon C, Sharma R, Kaur S. Leon C, et al. Evid Based Ment Health. 2019 Feb;22(1):e1. doi: 10.1136/ebmental-2018-300079. Epub 2019 Jan 21. Evid Based Ment Health. 2019. PMID: 30665988 Free PMC article. No abstract available.
Similar articles
- Guidance for identification and treatment of individuals with attention deficit/hyperactivity disorder and autism spectrum disorder based upon expert consensus. Young S, Hollingdale J, Absoud M, Bolton P, Branney P, Colley W, Craze E, Dave M, Deeley Q, Farrag E, Gudjonsson G, Hill P, Liang HL, Murphy C, Mackintosh P, Murin M, O'Regan F, Ougrin D, Rios P, Stover N, Taylor E, Woodhouse E. Young S, et al. BMC Med. 2020 May 25;18(1):146. doi: 10.1186/s12916-020-01585-y. BMC Med. 2020. PMID: 32448170 Free PMC article.
- Attention-deficit hyperactivity disorder. Posner J, Polanczyk GV, Sonuga-Barke E. Posner J, et al. Lancet. 2020 Feb 8;395(10222):450-462. doi: 10.1016/S0140-6736(19)33004-1. Epub 2020 Jan 23. Lancet. 2020. PMID: 31982036 Free PMC article. Review.
- Attention-deficit hyperactivity disorder (ADHD): an updated review of the essential facts. Tarver J, Daley D, Sayal K. Tarver J, et al. Child Care Health Dev. 2014 Nov;40(6):762-74. doi: 10.1111/cch.12139. Epub 2014 Apr 14. Child Care Health Dev. 2014. PMID: 24725022 Review.
- [Is emotional dysregulation a component of attention-deficit/hyperactivity disorder (ADHD)?]. Villemonteix T, Purper-Ouakil D, Romo L. Villemonteix T, et al. Encephale. 2015 Apr;41(2):108-14. doi: 10.1016/j.encep.2013.12.004. Epub 2014 Apr 1. Encephale. 2015. PMID: 24703785 French.
- Attention deficit/hyperactivity disorder: a focused overview for children's environmental health researchers. Aguiar A, Eubig PA, Schantz SL. Aguiar A, et al. Environ Health Perspect. 2010 Dec;118(12):1646-53. doi: 10.1289/ehp.1002326. Epub 2010 Sep 8. Environ Health Perspect. 2010. PMID: 20829148 Free PMC article. Review.
- The meaning of boredom : Properly managing childhood boredom could lead to more fulfilling lives. Uehara I, Ikegaya Y. Uehara I, et al. EMBO Rep. 2024 Jun;25(6):2515-2519. doi: 10.1038/s44319-024-00155-0. Epub 2024 May 13. EMBO Rep. 2024. PMID: 38741007 Free PMC article.
- Stimulant medications in children with ADHD normalize the structure of brain regions associated with attention and reward. Wu F, Zhang W, Ji W, Zhang Y, Jiang F, Li G, Hu Y, Wei X, Wang H, Wang SA, Manza P, Tomasi D, Volkow ND, Gao X, Wang GJ, Zhang Y. Wu F, et al. Neuropsychopharmacology. 2024 Feb 26. doi: 10.1038/s41386-024-01831-4. Online ahead of print. Neuropsychopharmacology. 2024. PMID: 38409281
- Management Strategies for Borderline Personality Disorder and Bipolar Disorder Comorbidities in Adults with ADHD: A Narrative Review. MacDonald L, Sadek J. MacDonald L, et al. Brain Sci. 2023 Oct 26;13(11):1517. doi: 10.3390/brainsci13111517. Brain Sci. 2023. PMID: 38002478 Free PMC article. Review.
- Inflammation, Dopaminergic Brain and Bilirubin. Jayanti S, Dalla Verde C, Tiribelli C, Gazzin S. Jayanti S, et al. Int J Mol Sci. 2023 Jul 14;24(14):11478. doi: 10.3390/ijms241411478. Int J Mol Sci. 2023. PMID: 37511235 Free PMC article. Review.
- Attention deficit hyperactivity disorder is associated with (a)symmetric tonic neck primitive reflexes: a systematic review and meta-analysis. Wang M, Yu J, Kim HD, Cruz AB. Wang M, et al. Front Psychiatry. 2023 Jul 7;14:1175974. doi: 10.3389/fpsyt.2023.1175974. eCollection 2023. Front Psychiatry. 2023. PMID: 37484683 Free PMC article. Review.
- Polanczyk G, de Lima MS, Horta BL, et al. . The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry 2007;164:942–8. 10.1176/ajp.2007.164.6.942 - DOI - PubMed
- Faraone SV, Biederman J, Mick E. The age-dependent decline of attention deficit hyperactivity disorder: a meta-analysis of follow-up studies. Psychol Med 2006;36:159–65. 10.1017/S003329170500471X - DOI - PubMed
- Sibley MH, Mitchell JT, Becker SP. Method of adult diagnosis influences estimated persistence of childhood ADHD: a systematic review of longitudinal studies. Lancet Psychiatry 2016;3:1157–65. 10.1016/S2215-0366(16)30190-0 - DOI - PubMed
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders, DSM-5. Fifth edn. American Psychiatric Publishing, 2013.
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Fourth edn: American Psychiatric Publishing, 2000.
Publication types
- Search in MeSH
Related information
- Cited in Books
LinkOut - more resources
Full text sources.
- Europe PubMed Central
- Ovid Technologies, Inc.
- PubMed Central
- Genetic Alliance
- MedlinePlus Health Information
Miscellaneous
- NCI CPTAC Assay Portal
- Citation Manager
NCBI Literature Resources
MeSH PMC Bookshelf Disclaimer
The PubMed wordmark and PubMed logo are registered trademarks of the U.S. Department of Health and Human Services (HHS). Unauthorized use of these marks is strictly prohibited.
Information
- Author Services
Initiatives
You are accessing a machine-readable page. In order to be human-readable, please install an RSS reader.
All articles published by MDPI are made immediately available worldwide under an open access license. No special permission is required to reuse all or part of the article published by MDPI, including figures and tables. For articles published under an open access Creative Common CC BY license, any part of the article may be reused without permission provided that the original article is clearly cited. For more information, please refer to https://www.mdpi.com/openaccess .
Feature papers represent the most advanced research with significant potential for high impact in the field. A Feature Paper should be a substantial original Article that involves several techniques or approaches, provides an outlook for future research directions and describes possible research applications.
Feature papers are submitted upon individual invitation or recommendation by the scientific editors and must receive positive feedback from the reviewers.
Editor’s Choice articles are based on recommendations by the scientific editors of MDPI journals from around the world. Editors select a small number of articles recently published in the journal that they believe will be particularly interesting to readers, or important in the respective research area. The aim is to provide a snapshot of some of the most exciting work published in the various research areas of the journal.
Original Submission Date Received: .
- Active Journals
- Find a Journal
- Proceedings Series
- For Authors
- For Reviewers
- For Editors
- For Librarians
- For Publishers
- For Societies
- For Conference Organizers
- Open Access Policy
- Institutional Open Access Program
- Special Issues Guidelines
- Editorial Process
- Research and Publication Ethics
- Article Processing Charges
- Testimonials
- Preprints.org
- SciProfiles
- Encyclopedia
Journal Menu
- Brain Sciences Home
- Aims & Scope
- Editorial Board
- Reviewer Board
- Topical Advisory Panel
- Instructions for Authors
- Special Issues
- Sections & Collections
- Article Processing Charge
- Indexing & Archiving
- Editor’s Choice Articles
- Most Cited & Viewed
- Journal Statistics
- Journal History
- Journal Awards
- Society Collaborations
- Conferences
- Editorial Office
Journal Browser
- arrow_forward_ios Forthcoming issue arrow_forward_ios Current issue
- Vol. 14 (2024)
- Vol. 13 (2023)
- Vol. 12 (2022)
- Vol. 11 (2021)
- Vol. 10 (2020)
- Vol. 9 (2019)
- Vol. 8 (2018)
- Vol. 7 (2017)
- Vol. 6 (2016)
- Vol. 5 (2015)
- Vol. 4 (2014)
- Vol. 3 (2013)
- Vol. 2 (2012)
- Vol. 1 (2011)
Find support for a specific problem in the support section of our website.
Please let us know what you think of our products and services.
Visit our dedicated information section to learn more about MDPI.
Advances in ADHD
- Print Special Issue Flyer
- Special Issue Editors
Special Issue Information
- Published Papers
A special issue of Brain Sciences (ISSN 2076-3425). This special issue belongs to the section " Developmental Neuroscience ".
Deadline for manuscript submissions: closed (31 August 2023) | Viewed by 79308
Share This Special Issue
Special issue editor.

Dear Colleagues,
Attention-deficit/hyperactivity disorder (ADHD) is the most common neurodevelopmental disorder in children, with an estimated worldwide prevalence around 5% and when applying empirically supported methods of diagnosis, the disorder persists into young adulthood for many people. Male to female ratio is around 3:1 in children and adolescents, but it is believed that females are under-diagnosed.
The etiology of ADHD involves the interplay of multiple genetic and environmental factors. There is no one direct cause for ADHD, either genetic or non-genetic. Rather, it is the complex interactions of multiple genes and multiple environmental risk factors. ADHD is a chronic disorder with identified genetic underpinnings, neurochemical and structural brain abnormalities, and common symptom presentations
ADHD related dysfunction includes occupational, academic, family, social, emotional and interpersonal functional impairments.
There is a need for a clear and concise approach to a complex disorder such as ADHD. Understanding the diagnosis and management of ADHD is incomplete without understanding comorbidities and how to manage them.
This Special Issue will provide insight into the important advances in diagnosis and management of ADHD and its comorbid disorders. The issue will also highlight recent advances in the neurobiology of ADHD.
Dr. Joseph Sadek Guest Editor
Manuscripts should be submitted online at www.mdpi.com by registering and logging in to this website . Once you are registered, click here to go to the submission form . Manuscripts can be submitted until the deadline. All submissions that pass pre-check are peer-reviewed. Accepted papers will be published continuously in the journal (as soon as accepted) and will be listed together on the special issue website. Research articles, review articles as well as short communications are invited. For planned papers, a title and short abstract (about 100 words) can be sent to the Editorial Office for announcement on this website.
Submitted manuscripts should not have been published previously, nor be under consideration for publication elsewhere (except conference proceedings papers). All manuscripts are thoroughly refereed through a single-blind peer-review process. A guide for authors and other relevant information for submission of manuscripts is available on the Instructions for Authors page. Brain Sciences is an international peer-reviewed open access monthly journal published by MDPI.
Please visit the Instructions for Authors page before submitting a manuscript. The Article Processing Charge (APC) for publication in this open access journal is 2200 CHF (Swiss Francs). Submitted papers should be well formatted and use good English. Authors may use MDPI's English editing service prior to publication or during author revisions.
- attention-deficit/hyperactivity disorder (ADHD)
- neurobiology
- neuropsychology
- comorbidities
- treatment response
Published Papers (21 papers)
Jump to: Review , Other
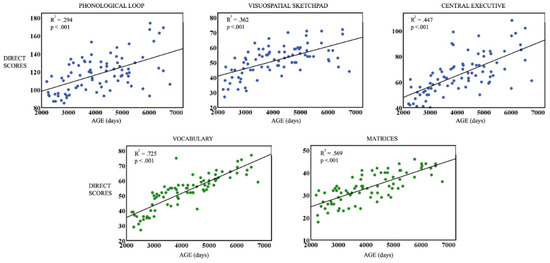
Jump to: Research , Other
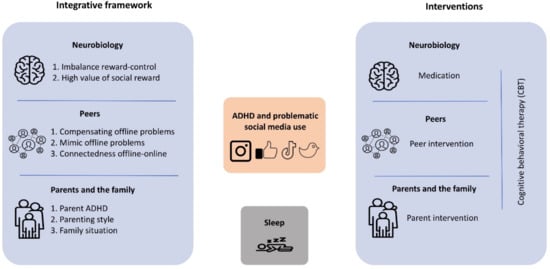
Jump to: Research , Review

Graphical abstract
Further Information
Mdpi initiatives, follow mdpi.
Subscribe to receive issue release notifications and newsletters from MDPI journals
Understanding and Supporting Attention Deficit Hyperactivity Disorder (ADHD) in the Primary School Classroom: Perspectives of Children with ADHD and their Teachers
- Original Paper
- Open access
- Published: 01 July 2022
- Volume 53 , pages 3406–3421, ( 2023 )
Cite this article
You have full access to this open access article

- Emily McDougal ORCID: orcid.org/0000-0001-7684-7417 1 , 3 ,
- Claire Tai 1 ,
- Tracy M. Stewart ORCID: orcid.org/0000-0002-8807-1174 2 ,
- Josephine N. Booth ORCID: orcid.org/0000-0002-2867-9719 2 &
- Sinéad M. Rhodes ORCID: orcid.org/0000-0002-8662-1742 1
41k Accesses
7 Citations
16 Altmetric
Explore all metrics
Children with Attention Deficit Hyperactivity Disorder (ADHD) are more at risk for academic underachievement compared to their typically developing peers. Understanding their greatest strengths and challenges at school, and how these can be supported, is vital in order to develop focused classroom interventions. Ten primary school pupils with ADHD (aged 6–11 years) and their teachers (N = 6) took part in semi-structured interviews that focused on (1) ADHD knowledge, (2) the child’s strengths and challenges at school, and (3) strategies in place to support challenges. Thematic analysis was used to analyse the interview transcripts and three key themes were identified; classroom-general versus individual-specific strategies, heterogeneity of strategies, and the role of peers. Implications relating to educational practice and future research are discussed.
Similar content being viewed by others

Evidence-Based Practices for Children, Youth, and Young Adults with Autism: Third Generation Review

The positive aspects of attention deficit hyperactivity disorder: a qualitative investigation of successful adults with ADHD

Systematic review and meta-analysis: relative age in attention-deficit/ hyperactivity disorder and autism spectrum disorder
Avoid common mistakes on your manuscript.
Characterised by persistent inattention, hyperactivity and impulsivity (APA, 2013), ADHD is a neurodevelopmental disorder thought to affect around 5% of children (Russell et al., 2014 ) although prevalence estimates vary (Sayal et al., 2018 ). Although these core symptoms are central to the ADHD diagnosis, those with ADHD also tend to differ from typically developing children with regards to cognition and social functioning (Coghill et al., 2014 ; Rhodes et al., 2012 ), which can negatively impact a range of life outcomes such as educational attainment and employment (Classi et al., 2012 ; Kuriyan et al., 2013 ). Indeed, academic outcomes for children with ADHD are often poor, particularly when compared with their typically developing peers (Arnold et al., 2020 ) but also compared to children with other neurodevelopmental disorders, such as autism (Mayes et al., 2020 ). Furthermore, children with ADHD can be viewed negatively by their peers. For example, Law et al. ( 2007 ) asked 11–12-year-olds to read vignettes describing the behaviour of a child with ADHD symptoms, and then use an adjective checklist to endorse those adjectives that they felt best described the target child. The four most frequently ascribed adjectives were all negative (i.e. ‘careless’, ‘lonely’, ‘crazy’, and ‘stupid’). These negative perceptions can have a significant impact on the wellbeing of individuals with ADHD, including self-stigmatisation (Mueller et al., 2012 ). There is evidence that teachers with increased knowledge of ADHD report more positive attitudes towards children with ADHD compared to those with poor knowledge (Ohan et al., 2008 ) and thus research that identifies the characteristics of gaps in knowledge is likely to be important in addressing stigma.
Previous research of teachers' ADHD knowledge is mixed, with the findings of some studies indicating that teachers have good knowledge of ADHD (Mohr-Jensen et al., 2019 ; Ohan et al., 2008 ) and others suggesting that their knowledge is limited (Latouche & Gascoigne, 2019 ; Perold et al., 2010 ). Ohan et al. ( 2008 ) surveyed 140 primary school teachers in Australia who reported having experience of teaching at least one child with ADHD. Teachers completed the ADHD Knowledge Scale which consisted of 20 statements requiring a response of either true or false (e.g. “A girl/boy can be appropriately labelled as ADHD and not necessarily be over-active ”). They found that, on average, teachers answered 76.34% of items correctly, although depth of knowledge varied across the sample. Almost a third of the sample (29%) had low knowledge of ADHD (scoring less than 69%), with just under half of teachers (47%) scoring in the average range (scores of 70–80%). Only a quarter (23%) had “high knowledge” (scores above 80%) suggesting that knowledge varied considerably. Furthermore, Perold et al. ( 2010 ) asked 552 teachers in South Africa to complete the Knowledge of Attention Deficit Disorders Scale (KADDS) and found that on average, teachers answered only 42.6% questions about ADHD correctly. Responses of “don’t know” (35.4%) and incorrect responses (22%) were also recorded, indicating gaps in knowledge as well as a high proportion of misconceptions. Similar ADHD knowledge scores were reported in Latouche and Gascoigne’s ( 2019 ) study, who found that teachers enrolled into their ADHD training workshop in Australia had baseline KADDS scores of below 50% accuracy (increased to above 80% accuracy after training).
The differences in ADHD knowledge reported between Ohan et al. ( 2008 ) and the more recent studies could be due to the measures used. Importantly, when completing the KADDS, respondents can select a “don’t know” option (which receives a score of 0), whereas the ADHD Knowledge Scale requires participants to choose either true or false for each statement. The KADDS is longer, with a total of 39 items, compared to the 20-item ADHD Knowledge Scale, offering a more in-depth knowledge assessment. The heterogeneity of measures used within the described body of research is also highlighted within Mohr-Jensen et al. ( 2019 ) systematic review; the most frequently used measure (the KADDS) was only used by 4 out of the 33 reviewed studies, showing little consensus on the best way to measure ADHD knowledge. Despite these differences in measurement, the findings from most studies indicate that teacher ADHD knowledge is lacking.
Qualitative methods can provide rich data, facilitating a deeper understanding of phenomena that quantitative methods alone cannot reveal. Despite this, there are very few examples in the literature of qualitative methods being used to understand teacher knowledge of ADHD. In one example, Lawrence et al. ( 2017 ) interviewed fourteen teachers in the United States about their experiences of working with pupils with ADHD, beginning with their knowledge of ADHD. They found that teachers tended to focus on the external symptoms of ADHD, expressing knowledge of both inattentive and hyperactive symptoms. Although this provided key initial insights into the nature of teachers’ ADHD knowledge, only a small section of the interview schedule (one out of eight questions/topics) directly focused on ADHD knowledge. Furthermore, none of the questions asked directly about strengths, with answers focusing on difficulties. It is therefore difficult to determine from this study whether teachers are aware of strengths and difficulties outside of the triad of symptoms. A deeper investigation is necessary to fully understand what teachers know, and to identify areas for targeted psychoeducation.
Importantly, improved ADHD knowledge may impact positively on the implementation of appropriate support for children with ADHD in school. For example, Ohan et al. ( 2008 ) found that teachers with high or average ADHD knowledge were more likely to perceive a benefit of educational support services than those with low knowledge, and teachers with high ADHD knowledge were also more likely to endorse a need for, and seek out, those services compared to those with low knowledge. Furthermore, improving knowledge through psychoeducation may be important for improving fidelity to interventions in ADHD (Dahl et al., 2020 ; Nussey et al., 2013 ). Indeed, clinical guidelines recommend inclusion of psychoeducation in the treatment plan for children with ADHD and their families (NICE, 2018 ). Furthermore, Jones and Chronis-Tuscano ( 2008 ) found that educational ADHD training increased special education teachers’ use of behaviour management strategies in the classroom. Together, these findings suggest that understanding of ADHD may improve teachers’ selection and utilisation of appropriate strategies.
Child and teacher insight into strategy use in the classroom on a practical, day-to-day level may provide an opportunity to better understand how different strategies might benefit children, as well as the potential barriers or facilitators to implementing these in the classroom. Previous research with teachers has shown that aspects of the physical classroom can facilitate the implementation of effective strategies for autistic children, for example to support planning with the use of visual timetables (McDougal et al., 2020 ). Despite this, little research has considered the strategies that children with ADHD and their teachers are using in the classroom to support their difficulties and improve learning outcomes. Moore et al. ( 2017 ) conducted focus groups with UK-based educators (N = 39) at both primary and secondary education levels, to explore their experiences of responding to ADHD in the classroom, as well as the barriers and facilitators to supporting children. They found that educators mostly reflected on general inclusive strategies in the classroom that rarely targeted ADHD symptoms or difficulties specifically, despite the large number of strategies designed to support ADHD that are reported elsewhere in the literature (DuPaul et al., 2012 ; Richardson et al., 2015 ). Further to this, when interviewing teachers about their experiences of teaching pupils with ADHD, Lawrence et al. ( 2017 ) specifically asked about interventions or strategies used in the classroom with children with ADHD. The reported strategies were almost exclusively behaviourally based, for example, allowing children to fidget or move around the classroom, utilising rewards, using redirection techniques, or reducing distraction. This lack of focus on cognitive strategies is surprising, given the breadth of literature focusing on the cognitive difficulties in ADHD (e.g. Coghill, et al., 2014 ; Gathercole et al., 2018 ; Rhodes et al., 2012 ). Furthermore, to our knowledge research examining strategy use from the perspective of children with ADHD themselves, or strengths associated with ADHD, is yet to be conducted.
Knowledge and understanding of ADHD in children with ADHD has attracted less investigation than that of teachers. In a Canadian sample of 8- to 12-year-olds with ADHD (N = 29), Climie and Henley ( 2018 ) found that ADHD knowledge was highly varied between children; scores on the Children ADHD Knowledge and Opinions Scale ranged from 5 to 92% correct (M = 66.53%, SD = 18.96). The authors highlighted some possible knowledge gaps, such as hyperactivity not being a symptom for all people with ADHD, or the potential impact upon social relationships, however the authors did not measure participant’s ADHD symptoms, which could influence how children perceive ADHD. Indeed, Wiener et al ( 2012 ) has shown that children with ADHD may underestimate their symptoms. If this is the case, it would also be beneficial to investigate their understanding of their own strengths and difficulties, as well as of ADHD more broadly. Furthermore, if children do have a poor understanding of ADHD, they may benefit from psychoeducational interventions. Indeed, in their systematic review Dahl et al. ( 2020 ) found two studies in which the impact of psychoeducation upon children’s ADHD knowledge was examined, both of which reported an increase in knowledge as a consequence of the intervention. Understanding the strengths and difficulties of the child, from the perspective of the child and their teacher, will also allow the design of interventions that are individualised, an important feature for school-based programmes (Richardson et al., 2015 ). Given the above, understanding whether children have knowledge of their ADHD and are aware of strategies to support them would be invaluable.
Teacher and child knowledge of ADHD and strategies to support these children is important for positive developmental outcomes, however there is limited research evidence beyond quantitative data. Insights from children and teachers themselves is particularly lacking and the insights which are available do not always extend to understanding strengths which is an important consideration, particularly with regards to implications for pupil self-esteem and motivation. The current study therefore provides a vital examination of the perspectives of both strengths and weaknesses from a heterogeneous group of children with ADHD and their teachers. Our sample reflects the diversity encountered in typical mainstream classrooms in the UK and the matched pupil-teacher perspectives enriches current understandings in the literature. Specifically, we aimed to explore (1) child and teacher knowledge of ADHD, and (2) strategy use within the primary school classroom to support children with ADHD. This novel approach, from the dual perspective of children and teachers, will enable us to identify potential knowledge gaps, areas of strength, and insights on the use of strategies to support their difficulties.
Participants
Ten primary school children (3 female) aged 7 to 11 years (M = 8.7, SD = 1.34) referred to Child and Adolescent Mental Health Services (CAMHS) within the NHS for an ADHD diagnosis were recruited to the study. All participant characteristics are presented in Table 1 . All children were part of the Edinburgh Attainment and Cognition Cohort and had consented to be contacted for future research. Children who were under assessment for ADHD or who had received an ADHD diagnosis were eligible to take part. Contact was established with the parent of 13 potential participants. Two had undergone the ADHD assessment process with an outcome of no ADHD diagnosis and were therefore not eligible to take part, and one could not take part within the timeframe of the study. The study was approved by an NHS Research Ethics Committee and parents provided informed consent prior to their child taking part. Co-occurrences data for all participants was collected as part of a previous study and are reported here for added context. All of the children scored above the cut-off (T-score > 70) for ADHD on the Conners 3 rd Edition Parent diagnostic questionnaire (Conners, 2008 ). The maximum possible score for this measure is 90. At the point of interview, seven children had received a diagnosis of ADHD, two children were still under assessment, and one child had been referred for an ASD diagnosis (Table 1 ). The ADHD subtype of each participant was not recorded, however all children scored above the cut-off for both inattention (M = 87.3, SD = 5.03) and hyperactivity (M = 78.6, SD = 5.8) which is indicative of ADHD combined type. Use of stimulant medication was not recorded at the time of interview.
Following the child interview and receipt of parental consent, each child’s school was contacted to request their teacher’s participation in the study. Three teachers could not take part within the timeframe of the study, and one refused to take part. Six teachers (all female) were successfully contacted and gave informed consent to participate.
Due to the increased likelihood of co-occurring diagnoses in the target population, we also report Autism Spectrum Disorder (ASD) symptoms and Developmental Co-ordination Disorder (DCD) symptoms using the Autism Quotient 10-item questionnaire (AQ-10; Allison et al., 2012 ) and Movement ABC-2 Checklist (M-ABC2; Henderson et al., 2007 ) respectively, both completed by the child’s parent.
Scores of 6 and above on the AQ-10 indicates referral for diagnostic assessment for autism is advisable. All but one of the participants scored below the cut-off on this measure (M = 3.6, SD = 1.84).
The M-ABC2 checklist categorises children as scoring green, amber or red based on their scores. A green rating (up to the 85th percentile) indicates no movement difficulty, amber ratings (between 85 and 95th percentile) indicate risk of movement difficulty, and red ratings (95th percentile and above) indicate high likelihood of movement difficulty. Seven of the participants received a red rating, one an amber rating, and two green ratings.
Socioeconomic status (SES) is also known to impact educational outcomes, therefore the SES of each child was calculated using the Scottish Index of Multiple Deprivation (SIMD), which is an area-based measure of relative deprivation. The child’s home postcode was entered into the tool which provided a score of deprivation on a scale of 1 to 5. A score of 1 is given to the 20% most deprived data zones in Scotland, and a score of 5 indicates the area was within the 20% least deprived areas.
Semi-Structured Interview
The first author, who is a psychologist, conducted interviews with each participant individually, and then a separate interview with their teacher. This was guided by a semi-structured interview schedule (see Appendix A, Appendix B) developed in line with our research questions, existing literature, and using authors (T.S. and J.B.) expertise in educational practice. The questions were adapted to be relevant for the participant group. For example, children were asked “If a friend asked you to tell them what ADHD is, what would you tell them?” and teachers were asked, “What is your understanding of ADHD or can you describe a typical child with ADHD?”. The schedule comprised two key sections for both teachers and children. The first section focused on probing the participant’s understanding and knowledge of ADHD broadly. The second section focused on the participating child’s academic and cognitive strengths and weaknesses, and the strategies used to support them. Interviews with children took place in the child’s home and lasted between 19 and 51 min (M = 26.3, SD = 10.9). Interviews with teachers took place at their school and were between 28 and 50 min long (M = 36.5, SD = 7.61). Variation in interview length was mostly due to availability of the participant and/or age of the child (i.e. interviews with younger children tended to be shorter). All interviews were recorded on an encrypted voice recorder and transcribed by the first author prior to data analysis. Pseudonyms were randomly generated for each child to protect anonymity.
Reflexive thematic analysis was used to analyse the data (Braun & Clarke, 2019 ). This flexible approach allows the data to drive the analysis, putting the participant at the centre of the research and placing high value on the experiences and perspectives of individual participants (Braun & Clarke, 2006 ). The six phases of reflexive thematic analysis as outlined by Braun and Clarke were followed: (1) familiarisation, (2) generating codes, (3) constructing themes, (4) revising themes, (5) defining themes, (6) producing the report. Due to the exploratory nature of this study, bottom-up inductive coding was used. Two of the authors (E.M. and C.T.) worked collaboratively to construct and subsequently define the themes using the process described above. More specifically, one author (E.M.) generated codes, with support from another author (C.T.). Collated codes and data were then abstracted into potential themes, which were reviewed and refined using relevant literature, as well as within the wider context of the data. This process continued until all themes were agreed upon.
In the first part of the analysis, focus was placed on summarising the participants’ understanding of ADHD, as well as what they thought their biggest strengths and challenges were at school. Following this, an in-depth analysis of the strategies used in the classroom was conducted, taking into account the perspective of both teachers and children, aiming to generate themes from the data.
Knowledge of ADHD
Children and teachers were asked about their knowledge of ADHD. When asked if they had ever heard of ADHD, the majority of children said yes. Some of the children could not explain to the interviewer what ADHD was or responded in a way that suggested a lack of understanding ( “it helps you with skills” – Niall, 7 years; “ Well it’s when you can’t handle yourself and you’re always crazy and you can just like do things very fast”— Nathan, 8 years). Very few of the children were able to elaborate accurately on their understanding of ADHD, which exclusively focused on inattention. For example, Paige (8 years) said “ its’ kinda like this thing that makes it hard to concentrate ” and Finn (10 years) said “ they get distracted more just in different ways that other people would ”. This suggests that children with ADHD may lack or have a limited awareness or understanding of their diagnosis.
When asked about their knowledge of ADHD, teachers tended to focus on the core symptoms of ADHD. All teachers directly mentioned difficulties with attention, focus or concentration, and most directly or indirectly referred to hyperactivity (e.g. moving around, being in “ overdrive ”). Most teachers also referred to social difficulties as a feature of ADHD, including not following social rules, reacting inappropriately to other children and appearing to lack empathy, which they suggested could be linked to impulsivity. For example, “ reacting in social situations where perhaps other children might not react in a similar way” (Paige’s teacher) and “ They can react really really quickly to things and sometimes aggressively” (Eric’s teacher). Although no teachers directly mentioned cognitive difficulties, some referred to behaviours indicative of cognitive difficulties, for example, “ they can’t store a lot of information at one time” (Eric’s teacher) and, “ it’s not just the concentration it’s the amount they can take in at a time as well” (Nathan’s teacher), which may reflect processing or memory differences. Heterogeneity was mentioned, in that ADHD can mean different things for different children (e.g., “ I think ADHD differs from child to child and I think that’s really important” —Nathan’s teacher). Finally, academic difficulties as a feature of ADHD were also mentioned (e.g., “ a child… who finds some aspects of school life, some aspects of the curriculum challenging ”—Jay’s teacher).
After being asked to give a general description of ADHD, each child was asked about their own strengths at school and teachers were also asked to reflect on this topic for the child taking part.
When asked what they like most about school, children often mentioned art or P.E. as their preferred subjects. A small number of children said they enjoyed maths or reading, but this was not common and the majority described these subjects as a challenge or something they disliked. There was also clear link between the aspects of school children enjoyed, and what they perceived to be a strength for them. For example, when asked what he liked about school, Eric (10 years) said, “ Math, I’m pretty good at that”, or when later asked what they were good at, most children responded with the same answers they gave when asked what they liked about school. It is interesting to note that subjects such as art or P.E. generally have a different format to more traditionally academic subjects such as maths or literacy. Indeed, Felicity (11 years) said, “ I quite like art and drama because there’s not much reading…and not really too much writing in any of those” . Children also tended to mention the non-academic aspects of school, such as seeing their friends, or lunch and break times.
Teachers’ descriptions of the children’s strengths were much more variable compared to strengths mentioned by children. Like the children, teachers tended to consider P.E and artistic activities to be a strength for the child with ADHD. Multiple teachers referred to the child having a good imagination and creative skills. For example, “ she’s a very imaginative little girl, she has a great ability to tell stories and certainly with support write imaginative stories” (Paige’s teacher) . Teachers referred to other qualities or characteristics of the child as strengths, although these varied across teachers. These included openness, both socially but also in the context of willingness to learn or being open to new challenges, being a hard worker, or an enjoyable person to be around (e.g., “ he is the loveliest little boy, I’ve got a lot of time for [Nathan]. He makes me smile every day, you know, he just comes out with stuff he’s hilarious”— Nathan’s teacher). The most noticeable theme that emerged from this data was that when some teachers began describing one of the child’s strengths, it was suffixed with a negative. For example, Henry’s teacher said, “ He’s got a very good imagination, his writing- well not so much the writing of the stories, he finds writing quite a challenge, but his verbalising of ideas he’s very imaginative”. This may reflect that while these children have their own strengths, these can be limited by difficulties. Indeed, Paige’s teacher said, “ I think she’s a very able little girl without a doubt, but there is a definite barrier to her learning in terms of her organisation, in terms of her focus” , which reinforces this notion.
Children were asked directly about what they disliked about school, and what they found difficult. Children tended to focus more on specific subjects, with maths and aspects of literacy being the most frequently mentioned of these. Children referred to difficulties with or a dislike for reading, writing and/or spelling activities, for example, Rory (9 years) said “ Well I suppose spelling because … sometimes we have to do some boring tasks like we have to write it out three times then come up with the sentence for each one which takes forever and it’s hard for me to think of the sentences if I’m not ready” . Linking this with known cognitive difficulties in ADHD, it is interesting to note that both memory and planning are implicated in this quote from Rory about finding spelling challenging. In terms of writing, children referred to both the physical act of writing (e.g., “ probably writing cause sometimes I forget my finger spaces ”—Paige, 8 years; “ [writing the alphabet is] too hard… like the letters joined together … [and] I make mistakes” —Jay, 7 years) as well as the planning associated with writing a longer piece of work (e.g. “ when I run out of ideas for it, it’s really hard to think of some more so I don’t usually get that much writing done ”—Rory (9 years) .
Aside from academic subjects, several children referred to difficulties with focus or attention (e.g. “ when I find it hard to do something I normally kind of just zone out ”—Felicity, 11 years, “ probably concentrating sometimes ”—Rory, 9 years), but boredom was also a common and potentially related theme (e.g. “ Reading is a bit hard though … it just sometimes gets a bit boring” —Finn, 10 years, “ I absolutely hate maths … ‘cause it’s boring ”—Paige, 8 years). It could be that children with ADHD find it more difficult to concentrate during activities they find boring. Indeed, when Jay (7 years) was asked how it made him feel when he found something boring, he said “ it made me not do my work ”. Some children also alluded to the social difficulties faced at school, which included bullying and difficulties making friends (e.g. “ just making all kind of friends [is difficult] ‘cause the only friend that I’ve got is [name redacted] ”—Nathan, 8 years; “ sometimes finding a friend to play with at break time [is difficult] ” – Paige, 8 years; “ there’s a lot of people in my school that they bully me” —Eric, 10 years).
When asked what they thought were the child’s biggest challenges at school, teachers' responses were relatively variable, although some common themes were identified. As was the case for children, teachers reflected on difficulties with attention, which also included being able to sit at the table for long periods of time (e.g. “ I would say he struggles the most with sitting at his table and focusing on one piece of work ”—Henry’s teacher). Teachers did also mention difficulties with subjects such as maths and literacy, although this varied from child to child, and often they discussed these in the context of their ADHD symptom-related difficulties. For example, Eric’s teacher said, “ we’ve struggled to get a long piece of writing out of him because he just can’t really sit for very long ”. This quote also alludes to difficulties with evaluating the child’s academic abilities, due to their ADHD-related difficulties, which was supported by other teachers (e.g. “ He doesn’t particularly enjoy writing and he’s slow, very slow. And I don’t know if that’s down to attention or if that’s something he actually does find difficult to do ” —Henry’s teacher). Furthermore, some teachers reflected on the child’s confidence as opposed to a direct academic difficulty. For example, Luna’s teacher said, “ I think it’s she lacks the confidence in maths and reading like the most ” and later, elaborated with “ she’ll be like “I can’t do it” but she actually can. Sometimes she’s … even just anxious at doing a task where she thinks … she might not get it. But she does, she’s just not got that confidence”.
Teachers also commonly mentioned social difficulties, and referred to these difficulties as a barrier to collaborative learning activities (e.g. “ he doesn’t always work well with other people and other people can get frustrated” —Henry’s teacher; “ [during] collaborative group work [Paige] perhaps goes off task and does things she shouldn’t necessarily be doing and that can cause friction within the group” —Paige’s teacher). Teachers also mentioned emotion regulation, mostly in relation to the child’s social difficulties. For example, Eric’s teacher said “ I think as well he does still struggle with his emotions like getting angry very very quickly, and being very defensive when actually he’s taken the situation the wrong way” , which suggests that the child’s difficulty with regulating emotions may impact on their social relationships.
Strategy Use in the Classroom
Strategies to support learning fell into one of four categories: concrete or visual resources, information processing, seating and movement, and support from or influence of others. Examples of codes included in each of these strategy categories are presented in Table 2 .
Concrete or visual resources were the most commonly mentioned type of strategy by teachers and children, referring to the importance of having physical representations to support learning. Teachers spoke about the benefit of using visual aids (e.g. “ I think [Henry] is quite visual so making sure that there is visual prompts and clues and things like that to help him ”—Henry’s teacher), and teachers and children alluded to these resources supporting difficulties with holding information in mind. For example, when talking about the times table squares he uses, Rory said “ sometimes I forget which one I’m on…and it’s easier for me to have my finger next to it than just doing it in my head because sometimes I would need to start doing it all over again ”.
Seating and movement were also commonly mentioned, which seemed to be specific to children with ADHD in that it was linked to inattention and hyperactivity symptoms. For example, teachers referred to supporting attention or avoiding distraction by the positioning of a child’s location in the classroom (e.g. “ he’s so easily distracted, so he has an individual desk in the room and he’s away from everyone else because he wasn’t coping at a table [and] he’s been so much more settled since we got him an individual desk” —Eric’s teacher). Some teachers also mentioned the importance of allowing children to move around the room where feasible, as well as giving them errands to perform as a movement break (e.g. “ if I need something from the printer, [Nathan] is gonna go for it for me…because that’s down the stairs and then back up the stairs so if I think he’s getting a bit chatty or he’s not focused I’ll ask him to go and just give him that break as well” —Nathan’s teacher). Children also spoke about these strategies but didn’t necessarily describe why or how these strategies help them.
Information processing and cognitive strategies included methods that supported children to process learning content or instructions. For example, teachers frequently mentioned breaking down tasks or instructions into more manageable chunks (e.g. “ with my instructions to [Eric] I break them down … I’ll be like “we’re doing this and then we’re doing this” whereas the whole class wouldn’t need that ”—Eric’s teacher). Teachers and children also mentioned using memory strategies such as songs, rhymes or prompts. For example, Jay’s teacher said, “ if I was one of the other children I could see why it would be very distracting but he’s like he’s singing to himself little times table songs that we’ve been learning in class” , and Paige (8 years) referred to using mnemonics to help with words she struggles to spell, “ I keep forgetting [the word] because. But luckily we got the story big elephants can always understand little elephants [which helps because] the first letter of every word spells because” .
Both groups of participants mentioned support from and influence of others, and referred to working with peers, the teacher–child relationship, and one-to-one teaching. Peer support was a common theme across the data and is discussed in more detail in the thematic analysis findings, where teachers and children referred to the importance of the role of peers during learning activities. Understanding the child well and adapting to them was also seen as important, for example, Luna’s teacher said, “ with everything curricular [I] try and have an art element for her, just so I know it’ll engage her [because] if it’s like a boring old written worksheet she’s not gonna do it unless you’re sitting beside her and you’re basically telling her the answers” . As indicated in this quote, teachers also referred to the effectiveness of one-to-one or small group work with the child (e.g. “ when somebody sits beside her and explains it, and goes “come on [Paige] you know how to do this, let’s just work through a couple of examples”… her focus is generally better ” – Paige’s teacher), however this resource is not always available (e.g. “ I’d love for someone to be one-to-one with [Luna] but it’s just not available, she doesn’t meet that criteria apparently ” – Luna’s teacher). Children also referred to seeking direct support from their teacher (e.g. “if I can’t get an idea of what I’m doing then I ask the teacher for help” – Paige, 8 years), but were more likely to mention seeking support from their peers than the teacher.
Thematic Analysis
In addition to summarising the types of strategies that teachers and children reported using in the classroom, the data were also analysed using thematic analysis to generate themes. These are now presented. The theme names, definitions, and example quotes for each theme are presented in Table 3 .
Theme 1: Classroom-General Versus Individual-Specific Strategies
During the interviews, teachers spoke about strategies that they use as part of their teaching practice for the whole class but that are particularly helpful for the child/children with ADHD. These tended to be concrete or visual resources that are available in the classroom for anyone, for example, a visual timetable or routine checklist (e.g. “ there’s also a morning routine and listing down what’s to be done and where it’s to go … it’s very general for the class but again it’s located near her” —Paige’s teacher).
Teachers also mentioned using strategies that have been implemented specifically for that child, and these strategies tended to focus on supporting attention. For example, Nathan’s teacher spoke about the importance of using his name to attract his attention, “ maybe explaining to the class but then making sure that I’m saying “[Nathan], you’re doing this”, you know using his name quite a lot so that he knows it’s his task not just the everybody task ”, and this was a strategy that multiple teachers referred to using with the individual child and not necessarily for other children. Other strategies to support attention with a specific child also tended to be seating and movement related, such as having an individual desk or allowing them to fidget. For example, Luna’s teacher said, “ she’s a fidgeter so she’ll have stuff to fidget with … [and] even if she’s wandering around the classroom or she’s sitting on a table, I don’t let other kids do that, but as long as she’s listening, it’s fine [with me]” .
Similar to teachers, children spoke about strategies or resources that were in place for them specifically as well as about general things in the classroom that they find helpful. That said, it was less common for children to talk about why particular strategies were in place for them and how they helped them directly.
In addition to recognising strategies that teachers had put in place for them, children also referred to using their own strategies in the classroom. The most frequently mentioned strategy was fidgeting, and although some of the younger children spoke about having resources available in the classroom for fidgeting, some of the older children referred to using their own toy or an object that was readily available to them but not intended for fidgeting. For example, Finn (10 years) and Rory (9 years) both spoke about using items from their pencil case to fiddle with, and explained that this would help them to focus. (“ Sometimes I fidget with something I normally just have like a pencil holder under the table moving about … [and] it just keeps my mind clear and not from something else ”—Rory; “ Sometimes I fiddle with my fingers and that sometimes helps, but if not I get one of my coloured pencils and have a little gnaw on it because that actually takes my mind off some things and it’s easier for me to concentrate when I have something to do ”—Finn). Henry (9 years) spoke about being secretive with his fidgeting as it was not permitted in class, “ if you just bring [a fidget toy] in without permission [the teacher will] just take it off of you, so it has to be something that’s not too big. I bring in a little Lego ray which is just small enough that she won’t notice ”. Although some teachers did mention having fidget toys available, not all teachers seemed to recognise the importance of this for the child, and some children viewed fidgeting as a behaviour they should hide from the teacher.
Another strategy mentioned uniquely by children was seeing their peers as a resource for ideas or information. This is discussed in more detail in Theme 3—The role of peers , but reinforces the notion that children also develop their own strategies, independently from their teacher, rather than relying only on what is made available to them.
Theme 2: Heterogeneity of Strategies
Teachers spoke about the need for a variety of strategies in the classroom, for two reasons: (1) that different strategies work for different children (e.g. “ some [strategies] will work for the majority of the children and some just don’t seem to work for any of them ”—Jay’s teacher), and (2) what works for a child on one occasion may not work consistently for the same child (e.g. “ I think it’s a bit of a journey with him, and some things have worked and then stopped working, so I think we’re constantly adapting and changing what we’re doing ”—Eric’s teacher). One example of both of these challenges of strategy use came from Luna’s teacher, who spoke about using a reward chart with Luna and another child with ADHD, “ [Luna] and another boy in my class [with ADHD] both had [a reward chart]… but I think whereas the boy loved his and still loves his, she was getting a bit “oh I’m too cool for this” or that sort of age… so I stopped doing that for her and she’s not missing that at all” . These quotes demonstrate that strategies can work differently for different children, highlighting the need for a variety of strategies for teachers to access and trial with children.
Some children also referred to the variability of whether a strategy was helpful or not; for example, Henry (9 years) said that he finds it helpful to fidget with a toy but that sometimes it can distract him and prevent him from listening to the teacher. He said, “ Well, [the fidget toy] helps but it also gets me into trouble when the teacher spots me building it when I’m listening…but then sometimes I might not listen in maths and [use the fidget toy] which might make it worse”. This highlights that both children and teachers might benefit from support in understanding the contexts in which to use particular strategies, as well as why they are helpful from a psychological perspective.
For teachers, building a relationship with and understanding the child was also highly important in identifying strategies that would work. Luna’s teacher reflected upon the difference in Luna’s behaviour at the start of the academic year, compared to the second academic term, “ at the start of the year, we would just clash the whole time. I didn’t know her, she didn’t know me … and then when we got that bond she was absolutely fine so her behaviour has got way better ”. Eric’s teacher also reflected on how her relationship with Eric had changed, particularly after he received his diagnosis of ADHD, “ I think my approach to him has completely changed. I don’t raise my voice, I speak very calmly, I give him time to calm down before I even broach things with him. I think our relationship’s just got so much better ‘cause I kind of understand … where he’s coming from ”. She also said, “ it just takes a long time to get to know the child and get to know what works for them and trialling different things out ”, which demonstrates that building a relationship with and understanding the child can help to identify the successful strategies that work with different children.
Theme 3: The Role of Peers
Teachers and children spoke about the role of the child’s peers in their learning. Teachers talked about the benefit of partnering the child with good role models (e.g. “ I will put him with a couple of good role models and a couple of children who are patient and who will actually maybe get on with the task, and if [Jay] is not on task or not on board with what they’re doing at least he’s hearing and seeing good behaviour ”—Jay’s teacher), whereas children spoke more about their peers as a source of information, idea generation, or guidance on what to do next. For example, when asked what he does to help him with his writing, Henry (9 years) said, “ [I] listen to what my partner’s saying… my half of the table discuss what they’re going to do so I can literally hear everything they’re doing and steal some of their ideas ”. Henry wasn’t the only child to use their peers as a source of information, for example, Niall (7 years) said, “ I prefer working with the children because some things I might not know and the children might help me give ideas ”, and with a more specific example, Rory (9 years) said, “ somebody chose a very good character for their bit of writing, and I was like “I think I might choose that character”, and somebody else said “my setting was going to be the sea”, and I chose that and put that in a tiny bit of my story ”.
Some children also spoke about getting help from their peers in other ways, particularly when completing a difficult task. Paige (8 years) said, “ if the question isn’t clear I try and figure it out, and if I can’t figure it out then… don’t tell my teacher this but I sometimes get help from my classmates ”, which suggests some guilt associated with asking for help from her peers. This could be related to confidence and self-esteem, which teachers mentioned as a difficulty for some children with ADHD. In some instances, children felt it necessary to directly copy their peers’ work; for example, Nathan (8 years) spoke about needing a physical resource (i.e. “ fuzzies ”) to complete maths problems, but that when none were available he would “ just end up copying other people ”. This could also be related to a lack of confidence, as he may feel as though he may not be able to complete the task on his own. Indeed, Nathan’s teacher mentioned that when he is given the option to choose a task from different difficulty levels, Nathan would typically choose something easier, and that it was important to encourage him to choose something more difficult to build his confidence, “ I quite often say to him “come on I think you can challenge yourself” and [will] use that language”.
Peers clearly play an important role for the children with ADHD, and this is recognised both by the children themselves, and by their teachers. Teachers also mentioned that children with ADHD respond well to one-to-one learning with staff, indicating that it is important for these children to have opportunities to learn in different contexts: whole classroom learning, small group work and one-to-one.
In this study, a number of important topics surrounding ADHD in the primary school setting were explored, including ADHD knowledge, strengths and challenges, and strategy use in the classroom, each of which will now be discussed in turn before drawing together the findings and outlining the implications.
ADHD Knowledge
Knowledge of ADHD varied between children and their teachers. Whilst most of the children claimed to have heard of ADHD, very few could accurately describe the core symptoms. Previous research into this area is limited, however this finding supports Climie and Henley’s ( 2018 ) finding that children’s knowledge of ADHD can be limited. By comparison, all of the interviewed teachers had good knowledge about the core ADHD phenotype (i.e. in relation to diagnostic criteria) and some elaborated further by mentioning social difficulties or description of behaviours that could reflect cognitive difficulties. This supports and builds further upon existing research into teachers’ ADHD knowledge, demonstrating that although teachers understanding may be grounded in a focus upon inattention and hyperactivity, this is not necessarily representative of the range of their knowledge. By interviewing participants about their ADHD knowledge, as opposed to asking them to complete a questionnaire as previous studies have done (Climie & Henley, 2018 ; Latouche & Gascoigne, 2019 ; Ohan et al., 2008 ; Perold et al., 2010 ), the present study has demonstrated the specific areas of knowledge that should be targeted when designing psychoeducation interventions for children and teachers, such as broader aspects of cognitive difficulties in executive functions and memory. Improving knowledge of ADHD in this way could lead to increased positive attitudes and reduction of stigma towards individuals with ADHD (Mueller et al., 2012 ; Ohan et al., 2008 ), and in turn improving adherence to more specified interventions (Bai et al., 2015 ).
Strengths and Challenges
A range of strengths and challenges were discussed, some of which were mentioned by both children and teachers, whilst others were unique to a particular group. The main consensus in the current study was that art and P.E. tended to be the lessons in which children with ADHD thrive the most. Teachers elaborated on this notion, speaking about creative skills, such as a good imagination, and that these skills were sometimes applied in other subjects such as creative writing in literacy. Little to no research has so far focused on the strengths of children with ADHD, therefore these findings identify important areas for future investigation. For example, it is possible that these strengths could be harnessed in educational practice or intervention.
Although a strength for some, literacy was commonly mentioned as a challenge by both groups, specifically in relation to planning, spelling or the physical act of writing. Previous research has repeatedly demonstrated that literacy outcomes are poorer for children with ADHD compared to their typically developing peers (DuPaul et al., 2016; Mayes et al., 2020 ), however in these studies literacy tended to be measured using a composite achievement score, where the nuance of these difficulties can be lost. Furthermore, in line with a recent systematic review and meta-analysis (McDougal et al., 2022 ) the present study’s findings suggest that cognitive difficulties may contribute to poor literacy performance in ADHD. This issue was not unique to literacy, however, as teachers also spoke about academic challenges in the context of ADHD symptoms being a barrier to learning, such as finding it difficult to remain seated long enough to complete a piece of work. Children also raised this issue of engagement, who referred to the most challenging subjects being ‘boring’ for them. This link between attention difficulties and boredom in ADHD has been well documented (Golubchik et al., 2020 ). The findings here demonstrate the need for further research into the underlying cognitive difficulties leading to academic underachievement.
Both children and teachers also mentioned social and emotional difficulties. Research has shown that many different factors may contribute to social difficulties in ADHD (for a review see Gardner & Gerdes, 2015 ), making it a complex issue to disentangle. That said, in the current study teachers tended to attribute the children’s relationship difficulties to behaviour, such as reacting impulsively in social situations, or going off task during group work, both of which could be linked to ADHD symptoms. Despite these difficulties, peers were also considered a positive support. This finding adds to the complexity of understanding social difficulties for children with ADHD, demonstrating the necessity and value of further research into this key area.
The three key themes of classroom-general versus individual-specific strategies , heterogeneity of strategies and the role of peers were identified from the interview transcripts with children and their teachers. Within the first theme, classroom-general versus individual-specific strategies, it was clear that teachers utilise strategies that are specific to the child with ADHD, as well as strategies that are general to the classroom but that are also beneficial to the child with ADHD. Previously, Moore et al. ( 2017 ) found that teachers mostly reflected on using general inclusive strategies, rather than those targeted for ADHD specifically, however the methods differ from the current study in two key ways. Firstly, Moore et al.’s sample included secondary and primary school teachers, for whom the learning environment is very different. Secondly, focus groups were used as opposed to interviews where the voices of some participants can be lost. The merit of the current study is that children were also interviewed using the same questions as teachers; we found that children also referred to these differing types of strategies, and reported finding them useful, suggesting that the reports of teachers were accurate. Interestingly, children also mentioned their own strategies that teachers did not discuss and may not have been aware of. This finding highlights the importance of communication between the child and the teacher, particularly when the child is using a strategy considered to be forbidden or discouraged, for example copying a peer’s work or fidgeting with a toy. This communication would provide an understanding of what the child might find helpful, but more importantly identify areas of difficulty that may need more attention. Further to this, most strategies specific to the child mentioned by teachers aimed to support attention, and few strategies targeted other difficulties, particularly other aspects of cognition such as memory or executive function, which supports previous findings (Lawrence et al., 2017 ). The use of a wide range of individualised strategies would be beneficial to support children with ADHD.
Similarly, the second theme, heterogeneity of strategies , highlighted that some strategies work with some children and not others, and some strategies may not work for the same child consistently. Given the benefit of a wide range of strategy use, for both children with ADHD and their teachers, the development of an accessible tool-kit of strategies would be useful. Importantly, and as recognised in this second theme, knowing the individual child is key to identifying appropriate strategies, highlighting the essential role of the child’s teacher in supporting ADHD. Teachers mostly spoke about this in relation to the child’s interests and building rapport, however this could also be applied to the child’s cognitive profile. A tool-kit of available strategies and knowledge of which difficulties they support, as well as how to identify these difficulties, would facilitate teachers to continue their invaluable support for children and young people with ADHD. This links to the importance of psychoeducation; as previously discussed, the teachers in our study had a good knowledge of the core ADHD phenotype, but few spoke about the cognitive strengths and difficulties of ADHD. Children and their teachers could benefit from psychoeducation, that is, understanding ADHD in more depth (i.e., broader cognitive and behavioural profiles beyond diagnostic criteria), what ADHD and any co-occurrences might mean for the individual child, and why certain strategies are helpful. Improving knowledge using psychoeducation is known to improve fidelity to interventions (Dahl et al., 2020 ; Nussey et al., 2013 ), suggesting that this would facilitate children and their teachers to identify effective strategies and maintain these in the long-term.
The third theme, the role of peers , called attention to the importance of classmates for children with ADHD, and this was recognised by both children and their teachers. As peers play a role in the learning experience for children with ADHD, it is important to ensure that children have opportunities to learn in small group contexts with their peers. This finding is supported by Vygotsky’s ( 1978 ) Zone of Proximal Development; it is well established in the literature that children can benefit from completing learning activities with a partner, especially a more able peer (Vygotsky, 1978 ).
Relevance of Co-Occurrences
Co-occurring conditions are common in ADHD (Jensen & Steinhausen, 2015 ), and there are many instances within the data presented here that may reflect these co-occurrences, in particular, the overlap with DCD and ASD. For ADHD and DCD, the overlap is considered to be approximately 50% (Goulardins et al., 2015 ), whilst ADHD and autism also frequently co-occur with rates ranging from 40 to 70% (Antshel & Russo, 2019 ). It was not an aim of the current study to directly examine co-occurrences, however it is important to recognise their relevance when interpreting the findings. Indeed, in the current sample, scores for seven children (70%) indicated a high likelihood of movement difficulty. One child scored above the cut-off for autism diagnosis referral on the AQ-10, indicating heightened autism symptoms. Further to this, some of the discussions with children and teachers seemed to be related to DCD or autism, for example, the way that they can react in social situations, or difficulties with the physical act of handwriting. This finding feeds into the ongoing narrative surrounding heterogeneity within ADHD and individualisation of strategies to support learning. Recognising the potential role of co-occurrences should therefore be a vital part of any psychoeducation programme for children with ADHD and their teachers.
Limitations
Whilst a strong sample size was achieved for the current study allowing for rich data to be generated, it is important to acknowledge the issue of representativeness. The heterogeneity of ADHD is recognised throughout the current study, however the current study represents only a small cohort of children and young people with ADHD and their teachers which should be considered when interpreting the findings, particularly in relation to generalisation. Future research should investigate the issues raised using quantitative methods. Also on this point of heterogeneity, although we report some co-occurring symptoms for participants, the number of co-occurrences considered here were limited to autism and DCD. Learning disabilities and other disorders may play a role, however due to the qualitative nature of this study it was not feasible to collect data on every potential co-occurrence. Future quantitative work should aim to understand the complex interplay of diagnosed and undiagnosed co-occurrences.
Furthermore, only some of the teachers of participating children took part in the study; we were not able to recruit all 10. It may be, for example, that the six teachers who did take part were motivated to do so based on their existing knowledge or commitment to understanding ADHD, and the fact that not all child-teacher dyads are represented in the current study should be recognised. Another possibility is the impact of time pressures upon participation for teachers, particularly given the increasing number of children with complex needs within classes. Outcomes leading from the current study could support teachers in this respect.
It is also important to recognise the potential role of stimulant medication. Although it was not an aim of the current study to investigate knowledge or the role of stimulant medication in the classroom setting, it would have been beneficial to record whether the interviewed children were taking medication for their ADHD at school, particularly given the evidence to suggest that stimulant medication can improve cognitive and behavioural symptoms of ADHD (Rhodes et al., 2004 ). Examining strategy use in isolation (i.e. with children who are drug naïve or pausing medication) will be a vital aim of future intervention work.
Implications/Future Research
Taking the findings of the whole study together, one clear implication is that children and their teachers could benefit from psychoeducation, that is, understanding ADHD in more depth (i.e., broader cognitive and behavioural profiles beyond diagnostic criteria), what ADHD might mean for the individual child, and why certain strategies are helpful. Improving knowledge using psychoeducation is known to improve fidelity to interventions (Dahl et al., 2020 ; Nussey et al., 2013 ), suggesting that this would facilitate children and their teachers to identify effective strategies and maintain these in the long-term.
To improve knowledge and understanding of both strengths and difficulties in ADHD, future research should aim to develop interventions grounded in psychoeducation, in order to support children and their teachers to better understand why and in what contexts certain strategies are helpful in relation to ADHD. Furthermore, future research should focus on the development of a tool-kit of strategies to account for the heterogeneity in ADHD populations; we know from the current study’s findings that it is not appropriate to offer a one-size-fits-all approach to supporting children with ADHD given that not all strategies work all of the time, nor do they always work consistently. In terms of implications for educational practice, it is clear that understanding the individual child in the context of their ADHD and any co-occurrences is important for any teacher working with them. This will facilitate teachers to identify and apply appropriate strategies to support learning which may well result in different strategies depending on the scenario, and different strategies for different children. Furthermore, by understanding that ADHD is just one aspect of the child, strategies can be used flexibly rather than assigning strategies based on a child’s diagnosis.
This study has provided invaluable novel insight into understanding and supporting children with ADHD in the classroom. Importantly, these insights have come directly from children with ADHD and their teachers, demonstrating the importance of conducting qualitative research with these groups. The findings provide clear scope for future research, as well as guidelines for successful intervention design and educational practice, at the heart of which we must acknowledge and embrace the heterogeneity and associated strengths and challenges within ADHD.
Allison, C., Auyeung, B., & Baron-Cohen, S. (2012). Autism spectrum quotient: 10 items (AQ-10). Journal of the American Academy of Child and Adolescent Psychiatry., 51 (2), 202–212.
Article PubMed Google Scholar
Antshel, K. M., & Russo, N. (2019). Autism spectrum disorders and ADHD: Overlapping phenomenology, diagnostic issues, and treatment considerations. Current Psychiatry Reports, 21 (5), 34. https://doi.org/10.1007/s11920-019-1020-5
Arnold, L. E., Hodgkins, P., Kahle, J., Madhoo, M., & Kewley, G. (2020). Long-term outcomes of ADHD: Academic achievement and performance. Journal of Attention Disorders, 24 (1), 73–85. https://doi.org/10.1177/1087054714566076
Bai, G., Yang, L., Wang, Y., & Niu, W.-Y. (2015). Effectiveness of a focused, brief psychoeducation program for parents of ADHD children: Improvement of medication adherence and symptoms. Neuropsychiatric Disease and Treatment, . https://doi.org/10.2147/NDT.S88625
Article PubMed PubMed Central Google Scholar
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3 (2), 77–101. https://doi.org/10.1191/1478088706qp063oa
Article Google Scholar
Braun, V., & Clarke, V. (2019). Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise and Health, 11 (4), 589–597. https://doi.org/10.1080/2159676X.2019.1628806
Classi, P., Milton, D., Ward, S., Sarsour, K., & Johnston, J. (2012). Social and emotional difficulties in children with ADHD and the impact on school attendance and healthcare utilization. Child and Adolescent Psychiatry and Mental Health, 6 (1), 33. https://doi.org/10.1186/1753-2000-6-33
Climie, E. A., & Henley, L. (2018). Canadian parents and children’s knowledge of ADHD. Vulnerable Children and Youth Studies, 13 (3), 266–275. https://doi.org/10.1080/17450128.2018.1484975
Coghill, D. R., Seth, S., & Matthews, K. (2014). A comprehensive assessment of memory, delay aversion, timing, inhibition, decision making and variability in Attention Deficit Hyperactivity Disorder: Advancing beyond the three-pathway models. Psychological Medicine, 44 (9), 1989–2001. https://doi.org/10.1017/S0033291713002547
Conners, C. K., & Multi-Health Systems Inc. (2008). Conners Comprehensive Behavior Rating Scales (Conners CBRS): Manual . North Tonawanda, N.Y: Multi-Health Systems.
Dahl, V., Ramakrishnan, A., Spears, A. P., Jorge, A., Lu, J., Bigio, N. A., & Chacko, A. (2020). Psychoeducation interventions for parents and teachers of children and adolescents with ADHD: A systematic review of the literature. Journal of Developmental and Physical Disabilities, 32 (2), 257–292. https://doi.org/10.1007/s10882-019-09691-3
DuPaul, G. J., Eckert, T. L., & Vilardo, B. (2012). The effects of school-based interventions for Attention Deficit Hyperactivity Disorder: A meta-analysis. School Psychology Review, 41 (4), 387412. https://doi.org/10.1080/02796015.2012.12087496
Gardner, D. M., & Gerdes, A. C. (2015). A review of peer relationships and friendships in youth with ADHD. Journal of Attention Disorders, 19 (10), 844–855. https://doi.org/10.1177/1087054713501552
Gathercole, S. E., Astle, D. A., Manly, T., the CALM Team, & Holmes, J. (2018). Cognition and behaviour in learning difficulties and ADHD: A dimensional approach [Preprint]. Animal Behavior and Cognition . https://doi.org/10.1101/260265
Golubchik, P., Manor, I., Shoval, G., & Weizman, A. (2020). Levels of proneness to boredom in children with Attention-Deficit/Hyperactivity Disorder on and off methylphenidate treatment. Journal of Child and Adolescent Psychopharmacology, 30 (3), 173–176. https://doi.org/10.1089/cap.2019.0151
Goulardins, J. B., Rigoli, D., Licari, M., Piek, J. P., Hasue, R. H., Oosterlaan, J., & Oliveira, J. A. (2015). Attention Deficit Hyperactivity Disorder and developmental coordination disorder: Two separate disorders or do they share a common etiology. Behavioural Brain Research, 292 , 484–492. https://doi.org/10.1016/j.bbr.2015.07.009
Henderson, S. E., Sugden, D. A., & Barnett, A. L. (2007). Movement assessment battery for children – (2nd ed.). Harcourt Assessment.
Google Scholar
Jensen, C. M., & Steinhausen, H.-C. (2015). Comorbid mental disorders in children and adolescents with Attention-Deficit/Hyperactivity Disorder in a large nationwide study. ADHD Attention Deficit and Hyperactivity Disorders, 7 (1), 27–38. https://doi.org/10.1007/s12402-014-0142-1
Jones, H. A., & Chronis-Tuscano, A. (2008). Efficacy of teacher in-service training for attention-deficit/hyperactivity disorder: Teacher in-service training for ADHD. Psychology in the Schools, 45 (10), 918–929. https://doi.org/10.1002/pits.20342
Kuriyan, A. B., Jr., Molina, B. S. G., Waschbusch, D. A., Gnagy, E. M., Sibley, M. H., Babinski, D. E., Walther, C., Cheong, J., Yu, J., & Kent, K. M. (2013). Young adult educational and vocational outcomes of children diagnosed with ADHD. Journal of Abnormal Child Psychology, 41 , 27–41. https://doi.org/10.1007/s10802-012-9658-z
Latouche, A. P., & Gascoigne, M. (2019). In-service training for increasing teachers’ ADHD knowledge and self-efficacy. Journal of Attention Disorders, 23 (3), 270–281. https://doi.org/10.1177/1087054717707045
Law, G. U., Sinclair, S., & Fraser, N. (2007). Children’s attitudes and behavioural intentions towards a peer with symptoms of ADHD: Does the addition of a diagnostic label make a difference? Journal of Child Health Care, 11 (2), 98–111. https://doi.org/10.1177/1367493507076061
Lawrence, K., Estrada, R. D., & McCormick, J. (2017). Teachers’ experiences with and perceptions of students with Attention Deficit/hyperactivity Disorder. Journal of Pediatric Nursing, 36 , 141–148. https://doi.org/10.1016/j.pedn.2017.06.010
Mayes, S. D., Waschbusch, D. A., Calhoun, S. L., & Mattison, R. E. (2020). Correlates of academic overachievement, nondiscrepant achievement, and learning disability in ADHD, autism, and general population samples. Exceptionality, 28 (1), 60–75. https://doi.org/10.1080/09362835.2020.1727324
McDougal, E., Gracie, H., Oldridge, J., Stewart, T. M., Booth, J. N., & Rhodes, S. M. (2022). Relationships between cognition and literacy in children with attention‐deficit/hyperactivity disorder: A systematic review and meta‐analysis. British Journal of Developmental Psychology , 40 (1), 130–150. https://doi.org/10.1111/bjdp.12395
McDougal, E., Riby, D. M., & Hanley, M. (2020). Teacher insights into the barriers and facilitators of learning in autism. Research in Autism Spectrum Disorders, 79 , 101674. https://doi.org/10.1016/j.rasd.2020.101674
Mohr-Jensen, C., Steen-Jensen, T., Bang-Schnack, M., & Thingvad, H. (2019). What do primary and secondary school teachers know about ADHD in children? Findings from a systematic review and a representative, nationwide sample of Danish teachers. Journal of Attention Disorders, 23 (3), 206–219. https://doi.org/10.1177/1087054715599206
Moore, D. A., Russell, A. E., Arnell, S., & Ford, T. J. (2017). Educators’ experiences of managing students with ADHD: A qualitative study: Educators’ management of ADHD. Child: Care, Health and Development, 43 (4), 489–498. https://doi.org/10.1111/cch.12448
Mueller, A. K., Fuermaier, A. B., Koerts, J., & Tucha, L. (2012). Stigma in attention deficit hyperactivity disorder. Attention Deficit and Hyperactivity Disorders, 4 (3), 101–114. https://doi.org/10.1007/s12402-012-0085-3
National Institute for Health and Care Excellence (NICE). (2018). Attention deficit hyperactivity disorder: Diagnosis and management . Retrieved August 2021, from https://www.nice.org.uk/guidance/ng87/chapter/Recommendations#managing-adhd .
Nussey, C., Pistrang, N., & Murphy, T. (2013). How does psychoeducation help? A review of the effects of providing information about Tourette syndrome and attention-deficit/hyperactivity disorder: A review of psychoeducational approaches in TS and ADHD. Child Care, Health and Development, 39 (5), 617–627. https://doi.org/10.1111/cch.12039
Ohan, J. L., Cormier, N., Hepp, S. L., Visser, T. A. W., & Strain, M. C. (2008). Does knowledge about attention-deficit/hyperactivity disorder impact teachers’ reported behaviors and perceptions? School Psychology Quarterly, 23 (3), 436–449. https://doi.org/10.1037/1045-3830.23.3.436
Perold, M., Louw, C., & Kleynhans, S. (2010). Primary school teachers’ knowledge and misperceptions of attention deficit hyperactivity disorder (ADHD). South African Journal of Education, 30 (3), 457–473.
Rhodes, S. M., Coghill, D. R., & Matthews, K. (2004). Methylphenidate restores visual memory, but not working memory function in attention deficit-hyperkinetic disorder. Psychopharmacology (berl), 175 (3), 319–330. https://doi.org/10.1007/s00213-004-1833-7
Rhodes, S. M., Park, J., Seth, S., & Coghill, D. R. (2012). A comprehensive investigation of memory impairment in attention deficit hyperactivity disorder and oppositional defiant disorder: Memory in ADHD and ODD. Journal of Child Psychology and Psychiatry, 53 (2), 128–137. https://doi.org/10.1111/j.1469-7610.2011.02436.x
Richardson, M., Moore, D. A., Gwernan-Jones, R., Thompson-Coon, J., Ukoumunne, O., Rogers, M., Whear, R., Newlove-Delgado, T. V., Logan, S., Morris, C., Taylor, E., Cooper, P., Stein, K., Garside, R., & Ford, T. J. (2015). Non-pharmacological interventions for attention-deficit/hyperactivity disorder (ADHD) delivered in school settings: Systematic reviews of quantitative and qualitative research. Health Technology Assessment, 19 (45), 1–470. https://doi.org/10.3310/hta19450
Russell, G., Rodgers, L. R., Ukoumunne, O. C., & Ford, T. (2014). Prevalence of parent-reported ASD and ADHD in the UK: Findings from the millennium cohort Study. Journal of Autism and Developmental Disorders, 44 (1), 31–40. https://doi.org/10.1007/s10803-013-1849-0
Sayal, K., Prasad, V., Daley, D., Ford, T., & Coghill, D. (2018). ADHD in children and young people: Prevalence, care pathways, and service provision. The Lancet. Psychiatry, 5 (2), 175–186. https://doi.org/10.1016/S2215-0366(17)30167-0
Vygotsky, L. S. (1978). Mind in society: The development of higher psychological processes . Harvard University Press.
Wiener, J., Malone, M., Varma, A., Markel, C., Biondic, D., Tannock, R., & Humphries, T. (2012). Children’s perceptions of their ADHD symptoms: Positive illusions, attributions, and stigma. Canadian Journal of School Psychology, 27 (3), 217–242. https://doi.org/10.1177/0829573512451972
Download references
The funding was provided by Waterloo Foundation Grant Nos. (707-3732, 707-4340, 707-4614).
Author information
Authors and affiliations.
Centre for Clinical Brain Sciences, Child Life and Health, University of Edinburgh, Edinburgh, United Kingdom
Emily McDougal, Claire Tai & Sinéad M. Rhodes
Moray House School of Education and Sport, University of Edinburgh, Edinburgh, United Kingdom
Tracy M. Stewart & Josephine N. Booth
School of Psychology, University of Surrey, Guildford, United Kingdom
Emily McDougal
You can also search for this author in PubMed Google Scholar
Contributions
E.M. Conceptualization, Methodology, Investigation, Data Curation, Formal Analysis, Writing - original draft, C.T. Formal Analysis, Writing - review & editing, T.M.S., J.N.B. and S.M.R. Conceptualization, Methodology, Writing - review & editing.
Corresponding author
Correspondence to Sinéad M. Rhodes .
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Interview Schedule—Teacher
Demographic/experience.
How many years have you been teaching?
Are you currently teaching pupils with ADHD and around how many?
If yes, do you feel competent/comfortable/equipped teaching pupils with ADHD?
If no, how competent/comfortable/equipped would you feel to teach pupils with ADHD?
Would you say your experience of teaching pupils with ADHD is small/moderate/significant?
Psychoeducation
What is your understanding of ADHD/Can you describe a typical child with ADHD?
Probe behaviour knowledge
Probe cognition knowledge
Probe impacts of behaviour/cognition difficulties
Probe knowledge that children with ADHD differ from each other
Probe knowledge that children with ADHD have co-occurring difficulties as the norm
(If they do have some knowledge) Where did you learn about ADHD?
e.g. specific training, professional experience, personal experience, personal interest/research
Cognitive skills and strategies
Can you tell me about the pupil’s strengths?
Can you tell me about the pupil’s biggest challenges/what they need most support with?
When you are supporting the pupil with their learning, are there any specific things you do to help them? (i.e. strategies)
Probe internal
Probe external
Probe whether they think those not mentioned might be useful/feasible/challenges
Probe if different for different subjects/times of the day
In your experience, which of these you have mentioned are the most useful for the pupil?
Probe for examples of how they apply it to their learning
Probe whether these strategies are pupil specific or broadly relevant
Probe if specific to particular subjects/times of the day
In your experience, which of these you have mentioned are the least useful for the pupil?
What would you like to be able to support the pupil with that you don’t already do?
Probe why they can’t access this currently e.g. lack of training, resources, knowledge, time
Is there anything you would like to understand better about ADHD?
Probe behaviour
Probe cognition
Interview Schedule—Child
Script: We’re going to have a chat about a few different things today, mostly about your time at school. This will include things like how you get on, how you think, things you’re good at and things you find more difficult. I’ve got some questions here to ask you but try to imagine that I’m just a friend that you’re talking to about these things. There are no right or wrong answers, I’m just interested in what you’ve got to say. Do you have any questions?
Script: First we’re going to talk about ADHD (Attention Deficit Hyperactivity Disorder).
Have you ever heard of/has anyone ever told you what ADHD is?
(If yes) If a friend asked you to tell them what ADHD is, what would you tell them?
Is there anything you would like to know more about ADHD?
Cognition/strategy use
Script: Now we’re going to talk about something a bit different. Everyone has things they are good at, and things they find more difficult. For example, I’m quite good at listening to what people have to say, but I’m not so good at remembering people’s names. I’d like you to think about when you’re in school, and things you’re good at and things you are not so good at. It doesn’t just have to be lessons, it can be anything.
Do you like school?
Probe why/why not?
Probe favourite lessons
What sort of things do you find you do well at in school?
Is there anything you think that you find more difficult in school?
Probe: If I asked your teacher/parent what you find difficult, what would they say?
Probe: Is there anything at school you need extra help with?
Probe: Is there anything you do to help yourself with that?
Script: Some people do things to try to help themselves do things well. For example, when someone tells me a number to remember, I repeat it in my head over and over again.
Can you try to describe to me what you do to help you do these things?
Solving a maths problem
Planning your writing
Doing spellings
Trying to remember something
Concentrating/ignoring distractions
Listening to the teacher
Remaining seated in class when doing work
Working with other children in the class
Probe: Do you use anything in lessons to help you with your work?
Probe: What kind of things do you think could help you with your work?
Probe: Is there anything you do at home, such as when you’re doing your homework, to help you finish what you are doing to do it well?
Probe: Does someone help you with your homework at home? If yes, what do they do that helps? If no, what do you think someone could do to help?
Script: In this last part we’re going to talk about your time at school.
How many teachers are in your class?
Is there anyone who helps you with your work?
Do you work mostly on your own or in groups?
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
McDougal, E., Tai, C., Stewart, T.M. et al. Understanding and Supporting Attention Deficit Hyperactivity Disorder (ADHD) in the Primary School Classroom: Perspectives of Children with ADHD and their Teachers. J Autism Dev Disord 53 , 3406–3421 (2023). https://doi.org/10.1007/s10803-022-05639-3
Download citation
Accepted : 06 June 2022
Published : 01 July 2022
Issue Date : September 2023
DOI : https://doi.org/10.1007/s10803-022-05639-3
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Child and teacher interviews
- Strengths and difficulties
- Learning strategies
- Find a journal
- Publish with us
- Track your research
South East Bay Pediatric Medical Group | Fremont, CA

Request an Appointment: (510) 792-4373
2191 mowry ave. #600c, fremont ca 94538, mon-fri: 8:45 am – 5pm, sat/sun/holiday: call at 8 am for appointment, an introduction to attention deficit hyperactivity disorder (adhd).
Almost all children have times when their behavior veers out of control. They may speed about in constant motion, make noise nonstop, refuse to wait their turn, and crash into everything around them. At other times they may drift as if in a daydream, failing to pay attention or finish what they start.
However, for some children, these kinds of behaviors are more than an occasional problem. Children with attention-deficit/hyperactivity disorder (ADHD) have behavior problems that are so frequent and/or severe that they interfere with their ability to live normal lives. These children often have trouble getting along with siblings and other children at school, at home, and in other settings. Those who have trouble paying attention usually have trouble learning. Some have an impulsive nature and this may put them in actual physical danger. Because children with ADHD have difficulty controlling their behavior, they may be labeled as “bad kids” or “space cadets.” Left untreated, more severe forms of ADHD can lead to serious, lifelong problems such as poor grades in school, run-ins with the law, failed relationships, substance abuse and the inability to keep a job.
What is ADHD?
ADHD is a condition of the brain that makes it difficult for children to control their behavior. It is one of the most common chronic conditions of childhood. It affects 4% to 12% of school-aged children. About 3 times more boys than girls are diagnosed with ADHD.
What are the symptoms of ADHD?
ADHD includes 3 behavior symptoms: inattention, hyperactivity, and impulsivity. A child with inattention symptoms may have the following behaviors:
- Has a hard time paying attention, daydreams
- Does not seem to listen
- Is easily distracted from work or play
- Does not seem to care about details, makes careless mistakes
- Does not follow through on instructions or finish tasks
- Is disorganized
- Loses a lot of important things
- Forgets things
- Does not want to do things that require ongoing mental effort
A child with hyperactivity symptoms may have the following behaviors:
- Is in constant motion, as if “driven by a motor”
- Cannot stay seated
- Squirms and fidgets
- Talks too much
- Runs, jumps, and climbs when this is not permitted
- Cannot play quietly (video games do not count)
A child with impulsivity symptoms may have the following behaviors:
- Acts and speaks without thinking
- May run into the street without looking for traffic first
- Has trouble taking turns
- Cannot wait for things
- Calls out answers before the question is complete
- Interrupts others
What is the difference between ADD vs. ADHD?
ADD stands for Attention Deficit Disorder. This is an old term that is now officially called Attention Deficit Hyperactivity Disorder, Inattentive Type. More on this will discussed below.
Are there different types of ADHD?
Children with ADHD may have one or more of the 3 main symptoms categories listed above. The symptoms usually are classified as the following types of ADHD:
- Inattentive type (formerly known as attention-deficit disorder [ADD])—Children with this form of ADHD are not overly active. Because they do not disrupt the classroom or other activities, their symptoms may not be noticed. Among girls with ADHD, this form is most common.
- Hyperactive/Impulsive type—Children with this type of ADHD show both hyperactive and impulsive behavior, but can pay attention.
- Combined Inattentive/Hyperactive/Impulsive type—Children with this type of ADHD show all 3 symptoms. This is the most common type of ADHD.
How can I tell if my child has ADHD?
Remember, it is normal for all children to show some of these symptoms from time to time. Your child may be reacting to stress at school or home. She may be bored or going through a difficult stage of life. It does not mean he or she has ADHD. Sometimes a teacher is the first to notice inattention, hyperactivity, and/or impulsivity and bring these symptoms to the parents’ attention. Sometimes questions from your pediatrician can raise the issue. Parents also may have concerns such as behavior problems at school, poor grades, difficulty finishing homework and so on. If your child is 6 years of age or older and has shown symptoms of ADHD on a regular basis for more than 6 months, discuss this with your pediatrician.
What causes ADHD?
ADHD is one of the most studied conditions of childhood but the cause of ADHD is still not clear at this time. The most popular current theory of ADHD is that ADHD represents a disorder of “executive function.” This implies dysfunction in the prefrontal lobes so that the child lacks the ability for behavioral inhibition or self-regulation of such executive functions as nonverbal working memory, speech internalization, affect, emotion, motivation, and arousal. It is believed that children with ADHD lack the right balance of neurotransmitters, which are specific chemicals in their brains, that help them to focus and inhibit impulses.
Research to date has shown the following:
- ADHD is a biological disorder, not just “bad behavior.” In a child with ADHD, the brain’s ability to properly use important chemical messengers (neurotransmitters) is impaired.
- A lower level of activity in the parts of the brain that control attention and activity level may be associated with ADHD.
- ADHD appears to run in families. Sometimes a parent is diagnosed with ADHD at the same time as the child.
- Environmental toxins can play a role in the development of ADHD, but that is extremely rare.
- Very severe head injuries may cause ADHD in rare cases.
There is no significant evidence that ADHD is caused by the following:
- Eating too much sugar
- Food additives
- Immunizations
Your pediatrician will determine whether your child has ADHD using standard guidelines developed by the American Academy of Pediatrics. Unfortunately, there is no single test that can tell whether your child has ADHD. The diagnosis process requires several steps and involves gathering a lot of information from multiple sources. You, your child, your child’s school, and other caregivers should be involved in assessing your child’s behavior.
Generally, if your child has ADHD:
- Some symptoms will occur in more than one setting, such as home, school, and social events
- The symptoms significantly impair your child’s ability to function in some of the activities of daily life, such as schoolwork and relationships with family and friends
- They will start before your child reaches 7 years of age
- They will continue for more than six months
- They will make it difficult for your child to function at school, at home, and/or in social settings
In addition to looking at your child’s behavior, your pediatrician will do a physical examination. A full medical history will be needed to put your child’s behavior in context and screen for other conditions that may affect your child’s behavior.
One of the challenges in diagnosing ADHD is that many disorders can look a lot like ADHD – including depression, anxiety, visual and hearing difficulties, seizures, learning disorders and even improper sleep quality. These conditions can show the same type of symptoms as ADHD. For example if your child has sleep apnea, a condition that involves disordered breathing during sleep, he may show signs of inattention and inability to focus that can sometimes be similar to a child with ADHD. Another example is a child that may have a learning disability. He/she may not pay attention in class due to inability to process that information and therefore be labeled with “inattention”. The same child may also be frustrated because he can’t process the material being taught in the classroom and therefore disturbs the classroom and acts as if he/she is “hyperactive.” In the case of this child with a learning disability, all the effort needs to be focused on the actual underlying problem, which again is the learning disability, and not on immediately trying to treat ADHD. Similarly, in our child with sleep apnea, parents need to address the sleeping problem first and not rush to place their child on medication for ADHD. As you will read below, it is possible to have ADHD with other conditions, so children who do have sleep apnea or learning disabilities MAY ALSO have ADHD and may eventually require treatment for both conditions.
The diagnosis of ADHD takes time, and the evaluation process usually takes at least 2-3 visits before the diagnosis can be made. Occasionally the process can take longer if referrals to psychologists or psychiatrists are warranted. Blood tests may or may not be indicated, and this will be discussed during your visit.
Coexisting conditions
- Oppositional defiant disorder or conduct disorder —Up to 35% of children with ADHD also have oppositional defiant disorder or conduct disorder. Children with oppositional defiant disorder tend to lose their temper easily and annoy people on purpose and are defiant and hostile toward authority figures. Children with conduct disorder break rules, destroy property, and violate the rights of other people. Children with coexisting conduct disorder are at much higher risk for getting into trouble with the law than children who have only ADHD. Studies show that this type of coexisting condition is more common among children with the primarily hyperactive/impulsive and combination types of ADHD. Your pediatrician may recommend counseling for your child if she has this condition.
- Mood disorders/depression —About 18% of children with ADHD also have mood disorders such as depression. There is frequently a family history of these types of disorders. Coexisting mood disorders may put children at higher risk for suicide, especially during the teenage years. These disorders are more common among children with inattentive and combined types of ADHD. Children with mood disorders or depression often require a different type of medication than those normally used to treat ADHD.
- Anxiety disorders —These affect about 25% of children with ADHD. Children with anxiety disorders have extreme feelings of fear, worry, or panic that make it difficult to function. These disorders can produce physical symptoms such as racing pulse, sweating, diarrhea, and nausea. Counseling and/or medication may be needed to treat these coexisting conditions.
- Learning disabilities —Learning disabilities are conditions that make it difficult for a child to master specific skills such as reading or math. ADHD is not a learning disability. However, ADHD can make it hard for a child to do well in school. Diagnosing learning disabilities requires evaluations such as IQ and academic achievement tests.
- Target outcomes for behavior
- Follow-up activities
- Education about ADHD
- Team work among doctors, parents, teachers, caregivers, other healthcare professionals, and the child
Behavior therapy
- Parent training
- Individual and family counseling
Treatment for ADHD uses the same principles that are used to treat other chronic conditions like asthma or diabetes. Long-term planning is needed because these conditions continue or recur for a long time. Families must manage them on an ongoing basis. In the case of ADHD, schools and other caregivers must also be involved in managing the condition. Educating the people involved with your child about ADHD is a key part of treating your child. As a parent, you will need to learn about ADHD. Read about the condition and talk to people who understand it. This will help you manage the ways ADHD affects your child and your family on a day-to-day basis. It will also help your child learn to help himself.
For most children, stimulant medications are a safe and effective way to relieve ADHD symptoms. As glasses help people focus their eyes to see, these medications help children with ADHD focus their thoughts better and ignore distractions. This makes them more able to pay attention and control their behavior. Stimulants may be used alone or combined with behavior therapy. Studies show that about 80% of children with ADHD who are treated with stimulants improve a great deal.
Different types of stimulants are available, in both short-acting (immediate-release) and long-acting forms. Short- acting forms usually are taken every 4 hours when the medication is needed. Long-acting medications usually are taken once in the morning. Children who use long-acting forms of stimulants can avoid taking medication at school or after school.
It may take some time to find the best medication, dosage, and schedule for your child. Your child may need to try different types of stimulants. Some children respond to one type of stimulant but not another. The amount of medication (dosage) that your child needs also may need to be adjusted. Realize that the dosage of the medicine is not based solely on your child weight. Our goal is for your child to be on the dose that is helping her to maximize her potential with the least amount of side effects.
The medication schedule also may be adjusted depending on the target outcome. For example, if the goal is to get relief from symptoms at school, your child may take the medication only on school days and none during weekends, summer time, and vacations if desired. Your child will have close follow up initially and once the optimal medication and dosage is found she will be seen every 2-3 months to monitor progress and possible side effects.
What side effects can stimulants cause?
Side effects occur sometimes. These tend to happen early in treatment and are usually mild and short-lived. The most common side effects include the following:
Decreased appetite/weight loss.
- Sleep problems
- Stomachaches
Some less common side effects include the following:
- Jitteriness
- Social withdrawal
- Rebound effect (increased activity or a bad mood as the medication wears off)
- Transient tics
Very rare side effects include the following:
- Increase in blood pressure or heart rate
- Growth delay
Most side effects can be relieved using one of the following strategies:
- Changing the medication dosage
- Adjusting the schedule of medication
- Using a different stimulant
There are many forms of behavior therapy, but all have a common goal— to change the child’s physical and social environments to help the child improve his behavior. Under this approach, parents, teachers, and other caregivers learn better ways to work with and relate to the child with ADHD. You will learn how to set and enforce rules, help your child understand what he needs to do, use discipline effectively, and encourage good behavior. Your child will learn better ways to control his behavior as a result.
Behavior therapy has 3 basic principles:
- Set specific goals. Set clear goals for your child such as staying focused on homework for a certain time or sharing toys with friends.
- Provide rewards and consequences. Give your child a specified reward (positive reinforcement) when she shows the desired behavior. Give your child a consequence (unwanted result or punishment) when she fails to meet a goal.
- Keep using the rewards and consequences. Using the rewards and consequences consistently for a long time will shape your child’s behavior in a positive way.
Behavior therapy recognizes the limits that having ADHD puts on a child. It focuses on how the important people and places in the child’s life can adapt to encourage good behavior and discourage unwanted behavior. It is different from play therapy or other therapies that focus mainly on the child and his emotions. Specific behavior therapy techniques that can be effective with children with ADHD include:
- Positive reinforcement: Parents provide rewards or privileges in response to desired behavior. For example, your child completes an assignment and he is permitted to play on the computer.
- Time-out: one removes access to desired activity because of unwanted behavior. For example, your child hits a sibling and, as a result, must sit for 5 minutes in the corner of the room.
- Response cost: Parents withdraw rewards or privileges because of unwanted behavior. For example, your child loses free-time privileges for not completing homework.
- Token economy: Combining reward and consequence. The child earns rewards and privileges when performing desired behaviors. He loses the rewards and privileges as a result of unwanted behavior. For example, you child can earn stars for completing assignments and loses stars for getting out of seat. Then, he cashes in the sum of her stars at the end of the week for a prize.
Tips for helping your child control his behavior
- Keep your child on a daily schedule . Try to keep the time that your child wakes up, eats, bathes, leaves for school, and goes to sleep the same each day.
- Cut down on distractions . Loud music, computer games, and television can be over-stimulating to your child. Make it a rule to keep the TV or music off during mealtime and while your child is doing homework. Whenever possible, avoid taking your child to places that may be too stimulating, like busy shopping malls.
- Organize your house . If your child has specific and logical places to keep his schoolwork, toys, and clothes, he is less likely to lose them. Save a spot near the front door for his school backpack so he can grab it on the way out the door.
- Reward positive behavior . Offer kind words, hugs, or small prizes for reaching goals in a timely manner or good behavior. Praise and reward your child’s efforts to pay attention.
- Set small, reachable goals . Aim for slow progress rather than instant results. Be sure that your child understands that he can take small steps toward learning to control himself.
- Help your child stay “on task.” Use charts and checklists to track progress with homework or chores. Keep instructions brief. Offer frequent, friendly reminders.
- Limit choices . Help your child learn to make good decisions by giving your child only 2 or 3 options at a time.
- Find activities at which your child can succeed. All children need to experience success to feel good about themselves and boost their self-confidence.
- Use calm discipline. Use consequences such as time-out, removing the child from the situation, or distraction. Sometimes it is best to simply ignore the behavior. Physical punishment, such as spanking or slapping, is not helpful. Discuss your child’s behavior with him when both of you are calm.
How can I help my child control her behavior?
Taking care of yourself also will help your child. Being the parent of a child with ADHD can be tiring and trying. It can test the limits of even the best parents. Parent training and support groups made up of other families who are dealing with ADHD can be a great source of help. Learn stress-management techniques to help you respond calmly to your child. Seek counseling if you feel overwhelmed or hopeless.
Ask us to help you find parent training, counseling, and support groups in your community. Under the resources section we will leave the link of a few handouts published by the NICHQ (National Initiative for Children’s Healthcare Quality) including:
- How to Establish a School-Home Daily Report Card
Unproven treatments
You may have heard media reports or seen advertisements for “miracle cures” for ADHD. Carefully research any such claims. Consider whether the source of the information is valid. At this time, there is no scientifically proven cure for this condition. The following methods have not been proven to work in scientific studies:
- Optometric vision training (asserts that faulty eye movement and sensitivities cause the behavior problems)
- Megavitamins and mineral supplements
- Anti–motion-sickness medication (to treat the inner ear)
- Treatment for candida yeast infection
- EEG biofeedback (training to increase brain-wave activity)
- Applied kinesiology (realigning bones in the skull)
Always tell your pediatrician about any alternative therapies, supplements, or medications that your child is using. These may interact with prescribed medications and harm your child.
Frequently asked questions
Will my child outgrow adhd.
ADHD continues into adulthood in most cases. However, by developing their strengths, structuring their environments, and using medication when needed, adults with ADHD can lead very productive lives. In some careers, having a high-energy behavior pattern can be an asset.
Are stimulant medications “gateway drugs” leading to illegal drug or alcohol abuse?
People with ADHD are naturally impulsive and tend to take risks. But those with ADHD who are taking stimulants are actually at lower risk of using other drugs. Children and teenagers who have ADHD and also have coexisting conditions may be at high risk for drug and alcohol abuse, regardless of the medication used.
Are children getting high on stimulant medications?
There is no evidence that children are getting high on stimulant drugs used to treat ADHD. These drugs also do not sedate or tranquilize children and have no addictive properties. Stimulants are classified as Schedule II drugs by the US Drug Enforcement Administration. There are recent reports of abuse of this class of medication, especially by college students who trying to obtain an edge during exam times to stay up and study more. If your child is on medication, it is always best to supervise the use of the medication closely.
Why do so many children have ADHD?
The number of children who are being treated for ADHD has risen. It is not clear whether more children have ADHD or more children are being diagnosed with ADHD. ADHD is now one of the most common and most studied conditions of childhood. Because of more awareness and better ways of diagnosing and treating this disorder, more children are being helped.
- AAP (American Academy of Pediatrics)
- About Our Kids (from NYU Child Study Center)
- Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD)
Adapted directly from
- American Academy of Pediatrics
- The Zukerman Parker Handbook of Development and Behavioral Pediatrics for Primary care
ADHD Research Paper

This sample ADHD research paper features: 8200 words (approx. 27 pages), an outline, and a bibliography with 14 sources. Browse other research paper examples for more inspiration. If you need a thorough research paper written according to all the academic standards, you can always turn to our experienced writers for help. This is how your paper can get an A! Feel free to contact our writing service for professional assistance. We offer high-quality assignments for reasonable rates.

Academic Writing, Editing, Proofreading, And Problem Solving Services
Get 10% off with 24start discount code, i. introduction.
II. Historical Context
III. Description and Diagnosis
A. The Core Symptoms
B. associated cognitive impairments, iv. theoretical framework.
V. Potential Etiologies
VI. Epidemiology of ADHD
Vii. developmental course and adult outcome, viii. diagnostic criteria, ix. conclusion.
X. Bibliography
It is not unusual for young children to be energetic and active, or to become bored quickly and move from one activity to another as they explore their environment. A young child’s desire for immediate gratification is to be expected, rather than the restraint or self-control that would be demanded of someone older. However, some children persistently display levels of activity that are far in excess of their age group. Some are unable to sustain their attention to activities, their interest in tasks assigned to them by others, or their persistence in achieving long-term goals as well as their peers.
When a child’s impulse control, sustained attention, and general self-regulation lag far behind expectations for their developmental level, they are likely to be diagnosed as having ADHD. Children with ADHD have a greater probability of experiencing a number of problems in their social, academic, and emotional development and daily adaptive functioning.
Attention Deficit/Hyperactivity Disorder (ADHD) has captured public commentary and scientific interest for more than 100 years. While the diagnostic labels for disorders of inattention, hyperactivity, and impulsiveness have changed numerous times, the actual nature of the disorder has changed little, if at all, from descriptions provided at the turn of the century. During the past century, and especially during the last 30 years, thousands of published scientific papers have focused on ADHD, making it one of the most wellstudied childhood psychiatric disorders.
II. Historical Context of ADHD
Serious clinical interest in children who have severe problems with inattention, hyperactivity, and poor impulse control is first found in three published lectures by the English physician, George Still, presented to the Royal Academy of Physicians in 1902. Still reported on a group of 20 children in his clinical practice whom he defined as having a deficit in “volitional inhibition” or a “defect in moral control” over their own behavior. Still’s observations described many of the associated features of ADHD that would be supported by research almost a century later, such as an overrepresentation of boys compared to girls, the greater incidence of alcoholism, criminal conduct, and depression among the biological relatives, and a familial predisposition to the disorder.
Initial interest in children with these characteristics arose in North America around the time of the great encephalitis epidemics of 1917 and 1918. Children surviving these brain infections were noted to have many behavioral problems similar to those comprising contemporary ADHD. These cases, as well as others known to have arisen from birth trauma, head injury, toxin exposure, and infections, gave rise to the concept of a “brain-injured child syndrome,” often associated with mental retardation. This term was eventually applied to children without a history of brain damage or evidence of retardation but who manifested behavioral problems such as hyperactivity or poor impulse control. This concept would later evolve into that of “minimal brain damage,” and eventually “minimal brain dysfunction” (MBD), as challenges were raised to the label given the lack of evidence of brain injury in many of these cases.
During the 1950s researchers became increasingly interested in hyperactivity. “Hyperkinetic impulse disorder” was attributed to cortical overstimulation resuiting from ineffective filtering of stimuli entering the brain. These studies gave rise to the notion of the “hyperactive child syndrome” typified by daily motor movement that was far in excess of that seen in normal children of the same age.
By the 1970s research findings emphasized the importance of problems with sustained attention and impulse control in addition to hyperactivity in understanding the nature of the disorder. In 1983 Virginia Douglas proposed that the disorder was comprised of major deficits in four areas: (1) the investment, organization, and maintenance of attention and effort; (2) the ability to inhibit impulsive behavior; (3) the ability to modulate arousal levels to meet situational demands; and (4) an unusually strong inclination to seek immediate reinforcement. Douglas’ work, along with numerous subsequent studies of attention, impulsiveness, and other cognitive factors, eventually led to renaming the disorder “Attention Deficit Disorder” (ADD) in 1980.
Just as significant as the renaming of the condition at that time was the distinction made between two types of ADD: those with hyperactivity and those without it. Little research existed at the time on the latter subtype. However, later research suggested that ADD without hyperactivity might be a separate and distinct disorder of a different component of attention (selective or focused) than was the type of inattention seen in those with ADD with hyperactivity (persistence and distractibility). Thus, rather than being related subtypes of a single disorder with a shared, common impairment in attention, future research may show these subtypes to constitute separate disorders of attention altogether.
Within a few years of the creation of the label ADD, concern was raised by Barkley in 1990 and Weiss and Hechtman in 1993 that problems with hyperactivity and impulse control were features critically important to differentiating the disorder from other conditions and to predicting later developmental risks. In 1987 the disorder was renamed Attention Deficit Hyperactivity Disorder. Diagnostic symptoms were identified from a single list of items incorporating all three constructs: hyperactivity, impulsivity, and inattention. The subtype of ADD without Hyperactivity was now renamed Undifferentiated ADD and relegated to minor diagnostic status until further research could clarify its nature and relationship to ADHD.
Around this same time (mid-1980s to 1990s) reports began to appear that challenged the notion that ADHD was primarily a disturbance in attention. Over the previous decade, researchers studying information-processing capacities in children with ADHD were having difficulty demonstrating that the problems these children had with attending to tasks were actually attentional in nature (i.e., related to the processing of incoming information). Problems in response inhibition and preparedness of the motor control system appeared to be more reliably demonstrated. Researchers, moreover, were finding that the problems with hyperactivity and impulsivity were not separate constructs but formed a single dimension of behavior. All of this led to the creation of two separate lists of symptoms for ADHD when the latest diagnostic manual for psychiatry, The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (also known as the DSM-IV) was published by the American Psychiatric Association in 1994. In the DSM-IV, one symptom list now existed for inattention and another for hyperactive-impulsive behavior. The inattention list once again permitted the diagnosis of a subtype of ADHD that consisted principally of problems with attention (ADHD Predominantly Inattentive Type). But two other subtypes were also identified (Predominantly Hyperactive-Impulsive and Combined Types). As of this writing, debate continues over the core deficit(s) involved in ADHD, with increasing emphasis being given to a central problem specifically with behavioral inhibition and more generally with self-regulation or executive functioning.
III. ADHD Description and Diagnosis
Problems with attention consist of the child’s inability to sustain attention or respond to tasks or play activities as long as others of the same age or to follow through on rules and instructions as well as others. The child appears more disorganized, distracted, and forgetful than others of the same age. Parents and teachers frequently complain that these children do not seem to listen as well as they should for their age, cannot concentrate, are easily distracted, fail to finish assignments, daydream, and change activities more often than others.
Research corroborates that, when compared to normal children, ADHD children are often more “off-task,” less likely to complete as much work as others, look away more from the activities they are requested to do (including television), persist less in correctly performing boring activities, and are slower and less likely to return to an activity once interrupted. Yet objective research does not find children with ADHD to be generally more distracted by most forms of extraneous events occurring during their task performance, although distractors within the task may prove more disruptive to them than to normal children. Research instead documents that ADHD children are more active than other children, are less mature in controlling motor movements, and have considerable difficulties with stopping an ongoing behavior. They frequently talk more than others and interrupt others’ conversations. They are less able to resist immediate temptations and delay gratification and respond too quickly and too often when they are required to wait and watch for events to happen.
Recent research shows that the problems with behavioral or motor inhibition arise first, at age 3 to 4 years, with those related to inattention emerging somewhat later in the developmental course of ADHD, at age 5 to 7 years. Whereas the symptoms of disinhibition seem to decline with age, those of inattention remain relatively stable during the elementary grades. Yet even the inattentiveness may decline by adolescence in some cases.
A number of factors have been noted to influence the ability of children with ADHD to sustain their attention to task performance, to control their impulses to act, to regulate their activity level, and to produce work consistently. They include: time of day or fatigue; increasing task complexity where organizational strategies are required; extent of restraint demanded for the context; level of stimulation within the setting; the schedule of immediate consequences associated with the task; and the absence of adult supervision during task performance.
It has been shown that children with ADHD are most problematic in their behavior when persistence in work-related tasks is required (i.e., chores, homework, etc.) or where behavioral restraint is necessary, especially in settings involving reduced parental monitoring (i.e., in church, in restaurants, when a parent is on the phone, etc.). Such children are least likely to pose behavioral management problems during free play, when little self-control is required. Fluctuations in the severity of ADHD symptoms have also been documented across a variety of school contexts. In this case, classroom activities involving self-organization and task-directed persistence are the most problematic, with significantly fewer problems posed by contexts involving fewer performance demands (i.e., at lunch, in hallways, at recess, etc.), and even fewer problems posed during highly entertaining special events (i.e., field trips, assemblies, etc.).
Although ADHD is defined by the presence of the two major symptom dimensions of inattention and disinhibition (hyperactivity-impulsivity), research indicates that these children often demonstrate deficiencies in many other abilities. These include: motor coordination and sequencing; working memory and mental computation; planning and anticipation or preparedness for action; verbal fluency and confrontational communication; effort allocation; applying organization strategies; the internalization of self-directed speech; adhering to restrictive instructions; the self-regulation of emotions; and self-motivation. Several studies have also demonstrated what both Still (1902) and Douglas (1983) noted anecdotally years ago–ADHD may be associated with less mature or diminished moral reasoning and the moral control of behavior.
The commonality among most or all of these seemingly disparate abilities is that all fall within the neuropsychological domain described as executive functions. The neurologist Joaquim Fuster wrote in 1989 that these executive abilities are probably mediated by the frontal cortex of the brain, and particularly the prefrontal lobes. Barkley has recently defined executive functions as being those neuropsychological processes that permit or assist with human self-regulation. Self-regulation is then defined as any self-directed form of behavior (both overt and covert) that serves to modify the probability of a subsequent behavior by the individual so as to alter the probability of a later consequence. Such behavior may even involve forgoing immediate rewards for the sake of maximizing delayed outcomes or even exposing oneself to immediate aversive circumstances for this same purpose. Self-regulatory behavior, therefore, includes thinking within this realm of private or covert self-directed behavior. By appreciating the role of the frontal lobes and the prefrontal cortex in these executive abilities, it is easy to see why researchers have repeatedly speculated that ADHD probably arises out of some disturbance or dysfunction of this brain region.
Many different hypotheses on the nature of ADHD have been proposed over the past century, such as Still’s (1902) notion of defective volitional inhibition and moral regulation of behavior, and Douglas’ (1983) theory of deficient attention, inhibition, arousal, and preference for immediate reward. Few of these have produced models of the disorder that were widely adopted by both scientists and clinicians or that served to drive further programmatic research initiatives. Some of these theories have suggested that ADHD is a deficit in sensitivity to reinforcement, a more general motivational disorder, or a deficit in rule-governed behavior (i.e., the control of behavior by language). Most recently, several theorists working in this area have proposed that ADHD represents a deficit behavioral inhibition; an assertion for which there is substantial evidence, at least for those subtypes that involve hyperactive-impulsive symptoms.
Consistent with these proposals, Barkley outlined a model of ADHD in 1994 that was based upon an earlier theory by Jacob Bronowski first set forth in 1966 on the evolution of the unique properties of human language and their relationship to response inhibition. Bronowski’s model was subsequently combined with that of Juaquim Fuster published in 1989, which specified that the overarching role of the prefrontal cortex is the cross-temporal organization of behavior. Barkley’s hybrid theoretical model of ADHD places behavioral inhibition at a central point and supportive point in relation to four other executive functions dependent upon it for their own effective execution. These functions are working memory, the self-regulation of emotion/motivation, the internalization of speech, and reconstitution (analysis and synthesis of behavioral structures in the service of goal-directed behavioral creativity). The four functions are believed to permit and subserve human self-regulation, bringing behavior progressively under the control of internally represented information, often about the future, and transferring it at least partially away from the control of behavior by more immediate consequences and external events. The executive control of behavior afforded by these functions is proposed to result in a greater capacity for predicting and controlling one’s self and one’s environment so as to maximize future consequences over immediate ones for the individual. And, more generally, the interaction of these executive functions permits far more organized and effective adaptive functioning.
Several assumptions are important in understanding this model as it is applied to ADHD. First, the capacity for behavioral inhibition begins to emerge first in the child’s development, prior to or corresponding with the emergence of the four executive functions. Second, inhibition does not directly cause the activation of these executive functions but sets the occasion for their occurrence and is necessary for their effective performance. Third, these functions probably emerge at different times in the child’s development and may have relatively independent developmental trajectories, although interactive. Fourth, the sweeping cognitive impairments that ADHD creates across these executive functions are secondary to the primary deficit in behavioral inhibition, implying that if inhibition were to be improved, these executive functions would likewise improve.
The deficit in behavioral inhibition is thought to arise principally from genetic and neurodevelopmental origins, rather than from purely social ones, although its expression is certainly influenced by a variety of social factors. The secondary deficits in the executive functions and self-regulation created by the primary deficit in inhibition feedback to contribute to further deficits in behavioral inhibition because self-regulation is required for self-restraint.
Behavioral inhibition is viewed in the model as comprising three related processes: (1) the capacity to inhibit “prepotent” responses prior to their initiation; (2) the capacity to cease ongoing response patterns once initiated such that both (1) and (2) create delays in responding to events; and (3) the protection of this delay and the self-directed (often private or cognitive) actions occurring within it from interference by competing events and their prepotent responses (interference control). Prepotent responses are defined as those for which immediate reinforcement (both positive and negative) is available for their performance or for which there is a strong history of reinforcement in this context. Through the postponement of the prepotent, automatic responses and the creation of this protected period of delay, the occasion is set for the four executive functions to act effectively in modifying the individual’s eventual initial responding to events or modifying their ongoing responses to those events (creating a sensitivity to feedback or errors). The executive system described here may exist so as to achieve a net maximization of both temporally distant and immediate consequences rather than immediate consequences alone. The chain of goal-directed, future-oriented behaviors set in motion by these acts of self-regulation is then also protected from interference during its performance by this same process of inhibition (interference control). Even if disrupted, the individual retains the capacity or intention (via working memory) to return to the goal-directed actions until the outcome is successfully achieved or judged to be no longer necessary.
Space permits here only a brief description of each of the four executive components of this new model of ADHD. The first of these involves working memory, or the capacity for prolonging and manipulating mental representations of events and using such information to control motor behavior. This particular type of memory can be thought of as remembering so as to do and serves to sustain otherwise fleeting information that will be useful in controlling subsequent responding, such as is seen in privately rehearsing a telephone number in mind so as to later dial it accurately. One component of working memory may be related to self-speech (verbal working memory), while a second component is related to perceptual imagery (visual-spatial) and probably involves self-directed sensing, as in visual imagery or covert audition. This retention of information related to past events (retrospection) gives rise to the conjecturing of future events (prospection), which sets in motion a preparedness to act in anticipation of the arrival of these future events (anticipatory set). Out of this continuous referencing or sensing of past and future probably arises the psychological sense of time. These activities taking place in working memory appear to be dependent upon behavioral inhibition. Such working memory processes have been shown to exist in rudimentary form even in young infants permitting them to successfully perform delayed response tasks to a limited degree. As the capacity for inhibition increases developmentally, it probably contributes to the further efficiency and effectiveness of working memory.
According to this model of ADHD, behavioral inhibition also sets the stage for the development of the second executive component of this model, that being the self-regulation of emotion in children. The inhibition of the initial prepotent response includes the inhibition of the initial emotional reaction that it may have elicited. It is not that the child does not experience emotion; rather, the behavioral reaction to or expression of that emotion is delayed along with any motor behavior associated with it. The delay in responding this creates allows the child time to engage in self-directed behaviors that will modify both the eventual response to the event as well as the emotional reaction that may accompany it. Because emotions are themselves forms of both motivational and arousal states, the model argues that deficits in the self-regulation of emotion should be associated with deficits in self-motivation and the self-control of arousal, particularly in the service of goal-directed behavior.
The internalization of self-directed speech, as originally described by Vygotsky, forms the third executive component of this model of ADHD. During the early preschool years, speech, once developed, is initially employed for communication with others. As behavioral inhibition progresses, language becomes turned on the self. It now is not just a means of influencing the behavior of others but provides a means of reflection as well as a means for controlling one’s own behavior (instruction).
The fourth component of this model involves the capacity to rapidly take apart and recombine units of behavior, including language. The delay in responding that behavioral inhibition permits allows time for information related to the event to be mentally prolonged and then dissassembled so as to extract more information about the event that will aid in preparing a response to it. In a related fashion, previously learned response patterns can also be broken down into smaller units of behavior. This internal decomposition of information and its associated response patterns permits the complementary process to occur, that being synthesis, or the invention of novel combinations of behavioral structures, including words and ideas, in the service of goal-directed action. This gives a highly creative or generative character as well as a hierarchically organized nature to human goal-directed behavior.
Finally, the internally represented information and motivation generated by these four executive functions is used to control a separate unit within the model, that being motor behavior itself. Such information serves to program, execute, and sustain behavior directed toward goals and the future, giving human behavior an intentional or purposive quality. Task-irrelevant movement is now more effectively suppressed, goal-directed behavior better sustained, and this pattern of behavior more efficiently reengaged should disruption of the behavioral pattern occur because of the control afforded by the internal information being generated from the four executive functions.
The impairment in behavioral inhibition occurring in ADHD is hypothesized to disrupt the efficient execution of these executive functions, thereby limiting the capacity of these individuals for self-regulation. The result is an impairment in the cross-temporal organization of behavior, in the prediction and control of one’s own behavior and environment, and inevitably in the maximization of long-term consequences for the individual.
How does this model account for the problems with attention believed to exist in ADHD? According to this model, it is critical to distinguish between two forms of sustained attention that are traditionally confused in the research literature on ADHD. The first is called contingency-shaped attention. This refers to continued responding in a situation or to a task as a function of the immediate available contingencies of reinforcement provided by the task or its context. Responding that is maintained under these conditions then is directly dependent on the immediate environmental contingencies. Many factors affect this form of sustained attention or responding: the novelty of the task, the intrinsic interest the activity may hold for the individual, the immediate reinforcement it provides for responding in the task, the state of fatigue of the individual, and the presence or absence of an adult supervisor (or other stimuli which signal other consequences for performance that are outside the task itself). The model predicts that this type of sustained attention relatively unaffected by ADHD as it is behavior under the control of external events.
As children mature, however, a second form of sustained attention emerges described in the model as goal-directed persistence. This form of sustained responding arises as a direct consequence of the development of self-regulation or the control of behavior by internally represented information. Such persistence derives from the development of a progressively greater capacity by the child to hold events, goals, and plans in mind (working memory), to adhere to rules governing behavior and to formulate and follow such rules, to self-induce a motivational state supportive of the plans and goals formulated by the individual so as to maintain goal-directed behavior, and even to create novel behaviors in the service of the goal’s attainment. The capacity to initiate and sustain chains of goal-directed behavior in spite of the absence of immediate environmental contingencies for their performance is predicted to be the form of sustained attention disrupted by ADHD.
Apart from this heuristically valuable distinction in forms of sustained attention, this theoretical model of ADHD makes numerous predictions about the cognitive and behavioral deficits likely to be found in those with the disorder (i.e., impaired working memory and sense of time, delayed internalization of speech, etc.), many of which have received little or no attention in research on ADHD. It also provides a framework by which to better organize and understand the numerous cognitive deficits identified in previous studies of children with ADHD than does the current view of ADHD as being chiefly an attention deficit.
V. Potential Etiologies of ADHD
The precise causes of ADHD are unknown at the present time. Numerous causes have been proposed, but evidence for many has been weak or lacking entirely. However, a number of factors have been shown to be associated with a significantly increased risk for ADHD in children.
The vast majority of the potentially causative factors associated with ADHD that are supported by empirical research seem to be biological in nature; that is, they are factors known to be related to or to have a direct effect on brain development and/or functioning. The precise causal pathways by which these factors lead to ADHD, however, are simply not known at this time.
Even so, far less evidence is available to support any purely psychosocial etiology of ADHD. In the vast majority of cases where such psychosocial risks have been found to be significantly associated with ADHD or hyperactivity, more careful analysis has shown these to be either the result of ADHD in the child or, far more often, to be related to aggression or conduct disorder rather than to ADHD. For instance, the child management methods used by parents, parenting stress, marital conflict, or parental psychopathology have now been shown to be far more strongly associated with aggressive and antisocial behavior than with ADHD. The strong hereditary influence in ADHD may also contribute to an apparent link between ADHD and poor child management by a parent — a link that may be attributable to the parent’s own ADHD. The environment in which the child is raised and schooled probably plays a larger role in determining the outcomes of children with the disorder and a much lesser role in primary causation.
Throughout the century, investigators have repeatedly noted the similarities between symptoms of ADHD and those produced by lesions or injuries to the frontal lobes of the brain, particularly the prefrontal cortex. Both children and adults suffering injuries to the certain regions of prefrontal cortex demonstrate deficits in sustained attention, inhibition, working memory, the regulation of emotion and motivation, and the capacity to organize behavior across time.
Numerous other lines of evidence have been suggestive of a neurological origin to the disorder. Several studies have examined cerebral blood flow in ADHD and normal children. They have consistently shown decreased blood flow to the prefrontal regions of the brain and the striatum with which these regions are richly interconnected, particularly in its anterior portion. More recently, studies using positron emission tomography (PET) to assess cerebral glucose metabolism have found diminished metabolism in adults and adolescent females with ADHD although not in adolescent males with ADHD. However, significant correlations have been noted between diminished metabolic activity in the left anterior frontal region of the brain and severity of ADHD symptoms in adolescent males with ADHD. This demonstration of an association between the metabolic activity of certain brain regions and symptoms of ADHD is critical in demonstrating a connection between the findings pertaining to brain activation and the behavior comprising ADHD.
More detailed analysis of brain structures using high resolution magnetic resonance imaging (MRI) devices has also suggested differences in some brain regions in those with ADHD. Initial studies that focused on reading-disabled children and used ADHD children as a contrast group examined the region of the left and right temporal lobes (the planum temporale). These regions are thought to be involved with auditory detection and analysis and, therefore, with certain subtypes of reading disabilities. For some time, researchers studying reading disorders have focused on these brain regions because of their connection to the rapid analysis of speech sounds. Children with ADHD and children with reading disabilities were found to have smaller right hemisphere plana temporale than the control group, while only the reading disabled children had a smaller left plana temporale. In another study, the corpus callosum was examined in subjects with ADHD. This structure assists with the interhemispheric transfer of information. Those with ADHD were found to have a smaller callosum, particularly in the area of the genu and splenium and that region just anterior to the splenium. An attempt to replicate this finding, however, failed to show any differences between ADHD and control children in the size or shape of the entire corpus callosum with the exception of the posterior portion of the splenium, which was significantly smaller in subjects with ADHD. Two additional studies examining the corpus callosum, however, documented smaller anterior (rostral) regions in children with ADHD; findings more consistent with prior studies of brain anatomy and functioning in children with ADHD. Most recently, two studies using larger samples of ADHD and normal children and MRI technology have both documented a smaller right prefrontal cortex and smaller right striatum and right basal ganglia (of which the striatum is a part) in ADHD children. Thus, despite some inconsistencies in findings across some of the earlier studies of brain morphology and functioning in ADHD, more recent studies are increasingly identifying the prefrontal regions of the brain and certain regions of the basal ganglia, such as the striatum, as probably being involved in the disorder.
None of these studies found evidence of frank brain damage in any of these structures in those with ADHD. This is consistent with past reviews of the literature conducted by Michael Rutter in 1983 suggesting that brain damage was related to less than 5% of those with hyperactivity. It is also consistent with more recent studies of twins suggesting that nonshared environmental factors, such as pre-, peri-, and postnatal neurological insults, among other factors, account for approximately 15 to 20% of the differences among individuals in the behavioral pattern associated with ADHD (inattention and hyperactive-impulsive behavior). Where differences in brain structures are found, they are probably the result of abnormalities that arise in brain development (embryology) within these particular regions, the causes of which are not known but may have to do with particular genes responsible for the construction of these brain regions.
No evidence exists to show that ADHD is the result of abnormal chromosomal structures (as in Down’s Syndrome), their fragility (as in Fragile X) or transmutation, or of extra chromosomal material (as in XXY syndrome). Children with such chromosomal abnormalities may show greater problems with attention, but such abnormalities are very uncommon in children with ADHD.
By far, the preponderance of research evidence suggests that ADHD is a trait that is highly hereditary in nature, making heredity one of the most well substantiated among the potential etiologies for ADHD. Multiple lines of research support such a conclusion. For years, researchers have noted the higher prevalence of psychopathology in the parents and other relatives of children with ADHD. In particular, higher rates of ADHD, conduct problems, substance abuse, and depression have been repeatedly observed in these studies. Research such as that by Joseph Biederman and colleagues at the Harvard Medical School (Massachusetts General Hospital) shows that between 10 and 35% of the immediate family members of children with ADHD are also likely to have the disorder, with the risk to siblings of the ADHD children being approximately 32%. More recent studies even suggest that if either parent has ADHD, the risk to offspring for the disorder may be as high as 50%.
Another line of evidence for genetic involvement in ADHD has emerged from studies of adopted children, which have found higher rates of hyperactivity in the biological parents of hyperactive children than in adoptive parents of hyperactive children. Biologically related and unrelated pairs of international adoptees also identified a strong genetic component to the behavioral dimension underlying ADHD.
Studies of twins conducted in the United States, Australia, and the United Kingdom provide a third avenue of evidence for a genetic contribution to ADHD. In general, these studies suggest that if one twin is diagnosed with ADHD, the concordance for the disorder in the second twin may be as high as 81 to 92% in monozygotic twins but only 29 to 35% in dizygotic twins.
Quantitative genetic analyses of a large sample of families studied in Boston by Joseph Biederman and his colleagues suggest that a single gene may account for the expression of the disorder. The focus of research recently has been on the dopamine type 2 gene, given findings of its increased association with alcoholism, Tourette’s Syndrome, and ADHD. However, difficulties have arisen in the replication of this finding. More recent studies have implicated the dopamine transporter gene as being involved in ADHD as might the D4D repeator gene, which has shown an association with novelty-seeking and risk-taking personality traits. Clearly, research into the genetic mechanisms involved in the transmission of ADHD across generations will prove an exciting and fruitful area of research endeavor over the next decade as the human genome is mapped and better understood and as more sophisticated genetic technologies arising from this project come to be applied to the study of the genetics of ADHD.
Pre-, peri-, and postnatal complications, and malnutrition, diseases, trauma, and other neurologically compromising events may occur during the development of the nervous system before and after birth. Among these various biologically compromising events, several have been repeatedly linked to risks for inattention and hyperactive behavior. Elevated body lead burden has been shown to have a small but consistent and statistically significant relationship to the symptoms comprising ADHD. However, even at relatively high levels of lead, less than 38% of these children are rated as hyperactive on teacher rating scales, implying that most lead-poisoned children do not develop symptoms of ADHD. Other types of environmental toxins found to have some relationship to inattention and hyperactivity are prenatal exposure to alcohol and tobacco smoke.
The prevalence of ADHD, as reviewed by Peter Szatmari in 1992, using large epidemiological studies ranges from a low of 2 % to a high of 6.3 %, with most falling within the range of 4.2 to 6.3 %. Most studies have found similar prevalence rates in elementary school-aged children. Differences in prevalence rates are due in part to different methods of selecting these populations, to the criteria used to define a case of ADHD, and to the age range of the samples. For instance, prevalence rates may be 2 to 3% in females but 6 to 9% in males during the 6 to 12-year-old age period, but fall to 1 to 2% in females and 3 to 4.5 % in males by adolescence.
While the declining prevalence of ADHD with age may reflect real recovery from the disorder, it may also involve, at least in part, an artifact of methodology. This artifact results from the use of items in the diagnostic symptom lists across the life span that are were developed upon and chiefly applicable to young children. These items may reflect the underlying constructs of ADHD very well at younger ages but may be increasingly less appropriate for older age groups. This could create a situation where individuals remain impaired by ADHD characteristics as they mature, but outgrow the diagnostic symptom list for the disorder, resulting in an illusory decline in prevalence over development. Until more age-appropriate symptoms are studied for adolescent and adult populations, this issue remains unresolved.
Gender appears to play a significant role in determining prevalence of ADHD within a population. On average, males are between 2 and 6 times more likely than females to be diagnosed with ADHD in epidemiological samples of children, with the average being roughly 3:1. Within clinic-referred samples, the sex ratio can rise to 6:1 to 9:1, suggesting that males with ADHD are far more likely to be referred to clinics than females, especially if they have an associated oppositional or conduct disorder. It is unclear at this time why males should be more likely to have ADHD than females. This could result partly from an artifact of the relationship between male gender and more aggressive and oppositional behavior; such behavior is known to increase the probability of referral to mental health centers. Because such behavior is often associated with ADHD, clinic-referred males are also more likely to have ADHD. The greater preponderance of males might also, in part, be an artifact of applying a set of diagnostic criteria developed primarily on males to females. Using a predominantly male population to set diagnostic criteria as was done for the DSM-IV (see below) could create a higher threshold for diagnosis for females relative to other females than for males relative to other males. Such a circumstance argues for the eventual examination of whether separate diagnostic criteria (symptom thresholds) ought to be considered for each gender.
ADHD occurs across all socioeconomic levels. Where differences in prevalence rates are found across levels of social class, they may be artifacts of the source used to define the disorder or of the association of ADHD with other disorders known to be related to social class, such as aggression and conduct disorder. No one, however, has made the argument that the nature or qualitative aspects of ADHD differ across social classes.
Hyperactivity or ADHD is present in all countries studied so far, such as New Zealand, Japan, Italy, Germany, India, and Australia. While it may not receive the same diagnostic label in each country, the behavior pattern comprising the disorder appears to be present internationally. ADHD arises also in all ethnic groups studied so far.
Major follow-up studies of clinically referred hyperactive children have been ongoing during the last 25 years at five sites: Montreal, New York City, Iowa City, Los Angeles, and Milwaukee. Follow-up studies of children identified as hyperactive during epidemiological screenings of general populations have also been conducted in the United States, Australia, New Zealand, and England.
The onset of ADHD symptoms has been found to be generally in the preschool years, typically by age 3 or 4, and usually by entry into formal schooling. First to arise in many cases is the pattern of hyperactive-impulsive behavior and, in some cases, oppositional and aggressive conduct. Preschool-aged children with significant degrees of inattentive and hyperactive behavior who are difficult to manage for their parents or teachers and whose pattern of such behavior is persistent for at least a year or more are highly likely to have ADHD and to retain their symptoms into the elementary school years.
By the time ADHD children move into the age range of 6 to 12 years, the problems with hyperactive-impulsive behavior are increasingly associated with difficulties with the form of sustained attention referred to above as goal-directed persistence and distractibility (poor interference control). These symptoms of inattention appear to arise by the age of 5 to 7 years and may emerge out of the increasing difficulties ADHD children are having with self-regulation. The inattentiveness evident in children having ADD without Hyperactivity (Predominantly Inattentive Type of ADHD) may be of a qualitatively different form (focused or selective attention) and may not emerge or be impairing of the child’s school performance until even later, such as mid-to-late childhood.
When ADHD is present in clinic-referred children, the likelihood is that 50 to 80% will continue to have their disorder into adolescence. Although severity levels of symptoms are declining over development, this does not mean hyperactive children are necessarily outgrowing their disorder relative to normal children; like mental retardation, the disorder of ADHD is defined by a developmentally relative deficiency, rather than an absolute one, that persists in many children over time.
The persistence of ADHD symptoms across childhood as well as into early adolescence appears to be associated with the initial degree of hyperactive/impulsive behavior in childhood, the co-existence of conduct problems or oppositional/hostile behavior, poor family relations and conflict in parent-child interactions, as well as maternal depression. These predictors have also been associated with the development and persistence of oppositional and conduct disorder into adolescence.
The Montreal follow-up study of Weiss and Hechtman reported in 1993 that at least half of their subjects were still impaired by some symptoms of the disorder in adulthood. The New York City longitudinal study by Salvatore Mannuzza and Rachel Klein suggested that 18 to 30% of hyperactive children continue to have significant symptoms of ADHD into adulthood. Most recently, the Milwaukee follow-up study by Barkley and Fischer suggests that the source of information about the symptoms may be a significant factor in establishing the persistence of the disorder into adulthood. Less than 25 % of ADHD children reported having significant symptom levels of the disorder in adulthood when asked about themselves as young adults while their parents indicated that more than 60% of these subjects continued to have clinically significant degrees of the disorder as young adults. Until more studies report adult outcomes for ADHD children using clinical diagnostic criteria appropriate for adults and collecting information not only from the adult but from a parent or an immediate family member who knows them well, the true persistence of the disorder into adulthood will remain a matter of some controversy. At the very least, current research suggests it may be 30 to 50%, although the percentage may be higher among clinic-referred children followed to adulthood.
The most recent diagnostic criteria for ADHD are defined in the DSM-IV (1994). They stipulate that individuals have had their symptoms of ADHD for at least 6 months, that these symptoms exist to a degree that is developmentally deviant, and that they have developed by 7 years of age. From the Inattention item list, six of nine items must be endorsed as developmentally inappropriate. Likewise, from the Hyperactive-Impulsive item list, six of nine items must be endorsed as deviant. Depending upon whether criteria are met for either or both symptom lists will determine the type of ADHD that is to be diagnosed: Predominantly Inattentive, Predominantly Hyperactive-Impulsive, or Combined Type.
These diagnostic criteria are empirically derived and are the most rigorous ever available in the history of clinical diagnosis for this disorder. They were developed by a committee of some of the leading experts in the field, a literature review of research on ADHD, an informal survey of rating scales assessing the behavioral dimensions related to ADHD by the committee, and from statistical analyses of the results of a field trial of the items using a large sample of children from 10 different sites in North America.
Controversy continues over whether ADHD-Predominantly Inattentive Type represents a true subtype of ADHD. It is unclear if these children share a common attentional disturbance with the Combined Type and are distinguished simply by the relative absence of significant hyperactivity-impulsivity or whether they have a qualitatively different impairment in attention from that seen in the Combined Type. Several recent reviews of the literature have suggested that this is not in fact a true subtype but actually a separate, distinct disorder having a different attentional disturbance than the one present in ADHD-Combined Type. However, evidence for this subtype’s existence was at least strong enough to place it within the DSM-IV while awaiting more research on its course and treatment responsiveness to help clarify its status. The very limited research available to date suggests that Predominantly Inattentive ADHD children have more problems in the focused or selective component of attention, appear sluggish in their speed of information processing, and may have memory retrieval problems; in contrast, those with ADHD-Combined Type have more problems with persistence and distractibility as well as with poor inhibition.
The research criteria from the International Classification of Diseases (ICD-10) for Hyperkinetic Disorders closely resemble the DSM-IV in stressing two lists of symptoms related to inattention and overactivity and in requiring that pervasiveness across settings be demonstrated. The specific item contents, manner of presenting these symptoms lists within the home and school setting, requirement for office observation of the symptoms, and the earlier age of onset (age 6 years) clearly differs from the DSM-IV, as does the specification of a lower bound of IQ below which the diagnosis should not be given.
Social critics have charged that professionals have been too quick to label energetic and exuberant children as having this mental disorder and that educators also may be using these labels simply as an excuse for poor educational environments. This would imply that children who are hyperactive or are diagnosed with ADHD are actually normal but are being labelled as mentally disordered because of parent and teacher intolerance. If this were actually true, then we should find no differences of any cognitive, behavioral, or social significance between ADHD children and normal children. We should also find ADHD is not associated with any significant later risks in development for maladjustment within any domains of adaptive functioning, social, or school performance. Furthermore, research on potential etiologies for the disorder should also come up empty-handed. This is hardly the case. It should become clear from the totality of information on ADHD presented here and elsewhere in reviews such as those by Barkley in 1990 and Hinshaw in 1994 that those with ADHD have significant deficits in behavioral inhibition and associated executive functions that are critical for effective self-regulation, that these deficits are significantly associated with various biological factors, and particularly genetic and neurodevelopmental ones, and that ADHD symptoms and other associated disorders pose substantial risks for these individuals over the life span.
Future research needs to address the nature of the attentional problems in ADHD given that current research seriously questions whether these problems are actually within the realm of attention at all. Most studies of ADHD point to impairment within the motor, output, or motivational systems of the brain being most closely affiliated with ADHD rather than deficiencies in the sensory processing systems where attention has been traditionally thought to reside. Even the problem with sustained attention may represent a deficiency in a more complex form of goal-directed persistence that arises out of poor self-regulation rather than representing a disturbance in the more primitive form of sustained responding that is contingency shaped. Our understanding of the very nature of the disorder of ADHD is at stake in how research comes to resolve these issues.
Key to understanding ADHD is the notion that it is actually a disorder of behavioral performance and not one of skill; of how and when one’s intelligence comes to be applied in everyday effective adaptive functioning and not in that knowledge itself; of doing what one knows how to do rather than of knowing what to do. The concepts of time, timing, and timeliness are likely to prove increasingly crucial in deepening our understanding of ADHD. In particular, psychological time, how it is sensed, and how it is used in the crosstemporal organizing of complex, goal-directed behavior and in self-regulation may come to be a critical element in models of ADHD. Undoubtedly, research on brain function and structure is likely to further our understanding of the unique role of the prefrontal cortex and the midbrain structures with which it is closely associated in ADHD. But advances in theoretical models must also occur in order to better understand the nature and organization of the executive functions subserved by these brain regions and even the relationship of genetics, which builds these brain regions in embryological development, to ADHD and the deficits it produces in behavioral performance. And the current body of twin studies further suggests that while such genetic influences are important, there exists a lesser but still important role for unique (nonshared) environmental influences on the differences among individuals in symptoms of ADHD and its underlying behavioral traits. Some of these influences are no doubt social in nature while others are likely to be nongenetic pre-, peri-, and postnatal factors affecting brain development. Such studies, not only on the basic psychological nature of ADHD but also on its basic neuroanatomic and neurogenetic origins and the influence of unique social factors upon them, forebode further significant and exciting advances to come in the understanding and treatment of this fascinating developmental disorder.
Bibliography:
- American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
- Barkley, R. A. (1997a). Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychological Bulletin, 121, 65-94.
- Barkley, R. A. (1977b). ADHD and the nature of self-controI. New York: Guilford.
- Barkley, R. A. (1994). Impaired delayed responding: A unified theory of attention deficit hyperactivity disorder. In D. K. Routh (Ed.), Disruptive behavior disorders: Essays in honor of Herbert Quay (pp. 11-57). New York: Plenum.
- Barkley, R. A. (1990). Attention deficit hyperactivity disorder: A handbook for diagnosis and treatment. New York: Guilford.
- Biederman, J., Faraone, S. V., Keenan, K., & Tsuang, M. T. (1991 ). Evidence of a familial association between attention deficit disorder and major affective disorders. Archives of General Psychiatry, 48, 633-642.
- Bronowski, J. (1977). Human and animal languages. A sense of the future (pp. 104-131 ). Cambridge, MA: MIT Press.
- Denckla, M. B. (1994). Measurement of executive function. In G. R. Lyon (Ed.), Frames of reference for the assessment of learning disabilities: New view on measurement issues (pp. 117-142). Baltimore, MD: Paul H. Brookes.
- Douglas, V. I. (1983). Attention and cognitive problems. In M. Rutter (Ed.), Developmental neuropsychiatry (pp. 280-329). New York: Guilford.
- Fuster, J. M. (1989). The prefrontal cortex. New York: Raven.
- Hinshaw, S. P. (1994). Attention deficits and hyperactivity in children. Thousand Oaks, CA: Sage.
- Rutter, M. (1983). Introduction: Concepts of brain dysfunction syndromes. In M. Rutter, (Ed.), Developmental neuropsychiatry (pp. 1-14). New York: Guilford.
- Szatmari, P. (1992). The epidemiology of ADHD. In G. Weiss (Ed.), Child and adolescent psychiatric clinics of North America (Vol. 1, pp. 361-372). Philadelphia: W. B. Saunders.
- Weiss, G. & Hechtman, L. (1993). Hyperactive children grown up. New York: Guilford.
ORDER HIGH QUALITY CUSTOM PAPER

An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Front Psychiatry
The lived experiences of adults with attention-deficit/hyperactivity disorder: A rapid review of qualitative evidence
Callie m. ginapp.
1 Yale School of Medicine, Yale University, New Haven, CT, United States
Grace Macdonald-Gagnon
2 Department of Psychiatry, Yale School of Medicine, New Haven, CT, United States
Gustavo A. Angarita
3 Connecticut Mental Health Center, New Haven, CT, United States
Krysten W. Bold
Marc n. potenza.
4 Connecticut Council on Problem Gambling, Wethersfield, CT, United States
5 Child Study Center, Yale School of Medicine, New Haven, CT, United States
6 Department of Neuroscience, Yale University, New Haven, CT, United States
7 Wu Tsai Institute, Yale University, New Haven, CT, United States
Associated Data
Attention-deficit/hyperactivity disorder (ADHD) is a common condition that frequently persists into adulthood, although research and diagnostic criteria are focused on how the condition presents in children. We aimed to review qualitative research on lived experiences of adults with ADHD to characterize potential ADHD symptomatology in adulthood and provide perspectives on how needs might be better met. We searched three databases for qualitative studies on ADHD. Studies ( n = 35) in English that included data on the lived experiences of adults with ADHD were included. These studies covered experiences of receiving a diagnosis as an adult, symptomatology of adult ADHD, skills used to adapt to these symptoms, relationships between ADHD and substance use, patients’ self-perceptions, and participants’ experiences interacting with society. Many of the ADHD symptoms reported in these studies had overlap with other psychiatric conditions and may contribute to misdiagnosis and delays in diagnosis. Understanding symptomatology of ADHD in adults may inform future diagnostic criteria and guide interventions to improve quality of life.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) has an estimated prevalence of 7% among adults globally ( 1 ). ADHD has historically been considered a disorder of childhood; however, 40–50% of children with ADHD may meet criteria into adulthood ( 2 ). Diagnostic criteria for ADHD include symptoms of inattention, hyperactivity, and impulsiveness present since childhood ( 3 ). These criteria are largely based on presentations in children, although diagnostic criteria have changed over time to better but not completely encompass considerations of experiences of adults ( 3 , 4 ).
Although adult ADHD is highly treatable with stimulant medication ( 5 ), adults with ADHD often have unmet needs. Substance use disorders (SUDs) are approximately 2.5-fold more prevalent among adults with versus without ADHD ( 6 , 7 ). Adults with ADHD are particularly likely to be incarcerated, with 26% of people in prison having ADHD ( 8 ). As diagnosis of ADHD has increased considerably in recent decades ( 9 ), there are likely many adults with ADHD who were not originally diagnosed as children. In more recent years, ADHD is still frequently underdiagnosed or misdiagnosed as other psychiatric conditions such as mood or personality disorders ( 10 ). Even when patients are diagnosed with ADHD as children, many patients lose access to resources when transitioning from child to adult health services ( 11 ) which may contribute to less than half of people with ADHD adhering to stimulant medication ( 12 ).
Non-pharmacological interventions such as cognitive behavioral therapy (CBT) have shown promise with helping adults manage their ADHD symptoms, although such symptoms are not completely ameliorated by therapy ( 13 – 15 ). A more thorough understanding of the symptoms adults with ADHD experience and the effects that these symptoms have on their lives may allow for more efficacious or targeted therapeutic interventions.
Qualitative research may provide insight into lived experiences, and findings from such studies may direct future research into potential symptoms and therapeutic interventions. The aim of this review is to describe the current qualitative literature on the lived experiences of adults with ADHD. This review may provide insight into the symptomatology of adult ADHD, identify areas where patient needs could be better met, and define gaps in understanding.
Search strategy
Using rapid review methodology ( 16 ), PubMed, PsychInfo, and Embase were searched on October 11th, 2021 with no date restrictions. The search terms included “ADHD” and related terms as well as “qualitative methods” present in the titles or abstracts. The full search ( Supplementary Appendix 1 ) was conducted with the help of a clinical librarian. The search yielded 417 articles which were uploaded to Endnote X9 where 111 duplicates were removed. The remaining 307 articles were uploaded to Covidence Systematic Review Management Software for screening, with one additional duplicate removed. The search also yielded a previous review on the lived experiences of adults with ADHD ( 17 ). The ten articles present in this review were also uploaded to Covidence where two duplicates were removed resulting in 314 unique articles.
Study selection
Studies reporting original peer-reviewed qualitative data on the lived experience of adults with ADHD, including mixed-methods studies, were eligible for inclusion. “Adult” was defined as being 18 years of age or older; studies that included adolescent and young adult participants were only included if results were reported separately by age. Studies that included some participants without ADHD were included if results were reported separately by diagnosis. Any studies with adult participants who were exclusively reflecting on their childhood experiences with ADHD were considered outside this study’s scope, as were studies on family members, medical providers, or other groups commenting on adults with ADHD. Articles could be from any country, but needed to have been published in English. Individual case studies were not included due to concerns with generalizability.
Twenty percent of titles and abstracts were screened by two reviewers for meeting the inclusion criteria. Studies were not initially excluded based on participants’ ages as many titles and abstracts did not specify age. One reviewer screened the remaining abstracts; a second reviewer screened all excluded abstracts. For full-text screening, ten articles were screened by both reviewers to ensure consistency. One reviewer screened the remaining articles; a second reviewer screened all excluded articles.
Quality appraisal
Quality appraisal was completed by one reviewer using the Joanna Briggs Institute critical appraisal checklist for qualitative research ( 18 ). Half of included studies did not state philosophical perspectives, two-thirds did not locate researchers culturally or theoretically, nearly one-third did not include specific information about ethics approval, and only two studies commented on reflexivity ( Supplementary Appendix 2 ). Given the varied quality appraisal results and the small body of literature, all studies were included regardless of methodological rigor.
Data extraction
Data extracted included general study characteristics and methodology, participant characteristics (sample size, demographics, and country of residence), study aims, and text excerpts of qualitative results. Study characteristics were entered into a Google Sheets document. PDFs of all studies were uploaded into NVivo 12, and results sections were coded using grounded theory ( 19 ). One reviewer extracted and coded data; a second reviewed extracted data for thematic consistency.
Study characteristics
One-hundred-and-seventy-three articles were deemed relevant in title and abstract screening. Of these, 35 were included after the full-text review ( Figure 1 ). Articles were published between 2005 and 2021, and methodology mostly consisted of individual interviews (91%), with other studies utilizing focus groups (14%). Eight studies focused on young adults (18–35 years), and three were specific to older adults (>50 years). Two had exclusively male participants, and three had exclusively female participants. Nineteen were conducted in Europe, nine in North America, and three in Asia. No studies included participants from Africa, South America, or Oceania. In six studies, participants had current or prior SUDs, six studies focused on college students, four included participants diagnosed in adulthood, and two included highly educated/successful participants ( Table 1 ).

PRISMA flow diagram showing the search strategy for identifying qualitative studies on the lived experience of adult attention-deficit/hyperactivity disorder (ADHD).
Article characteristics of included studies.
| Author | Aim | Country | Method | Age, years | Sex/gender | Race/ethnicity | |
| Ando et al. ( ) | How COVID-19 affects living conditions for adults receiving an adaptive coaching intervention | Japan | Interviews | 4 | 20s–40s | 50% male | – |
| Aoki et al. ( ) | Experience of being diagnosed in adulthood | Japan | Interviews | 12 | 20–60 | 50% male | – |
| Brod et al. ( ) | Burden of illness of ADHD | Canada, France, Germany, Italy, Netherlands, United Kingdom, and United States | Focus groups and interviews | 108 | 52% male | 74% white, 3% black, 3% Hispanic, 13% mixed | |
| Brod et al. ( ) | Examine quality of life issues | United States | Focus groups and interviews | 29 | 18–59 | 65% male | – |
| Canela et al. ( ) | Skills and coping strategies used before diagnosis or treatment | Switzerland | Interviews | 32 | 34% > 45 | 56% male | – |
| Canela et al. ( ) | Opinions and attitudes toward testing and stimulant treatment of children with ADHD | Switzerland | Interviews | 32 | 25% > 51; 22% 21–30 | 56% male | – |
| Ek et al. ( ) | How adults with ADHD perform everyday activities | Sweden | Interviews | 12 | 21–38 | 50% male | – |
| Goffer et al. ( ) | Occupational experiences of college students | Israel | Interviews | 20 | 25.4 (3.67) | 35% male | – |
| Hansson Halleröd et al. ( ) | Experience of being diagnosed in adulthood | Sweden | Interviews | 21 | 32 (9) | 48% male | – |
| Henry and Jones ( ) | Experiences of women in late adulthood | United States | Interviews | 9 | >60 | 100% female | 78% white 22% Hispanic |
| Kronenberg et al. ( ) | Consequences of SUDs for everyday life | Netherlands | Interviews | 11 | 43 | 73% male | – |
| Kronenberg et al. ( ) | Process of recovery from SUDs | Netherlands | Interviews | 9 | 36 (29–54) | 89% male | – |
| Kwon et al. ( ) | Difficulties in university life | South Korea | Interviews | 12 | 22.2 (20–29) | 41% male | – |
| Lasky et al. ( ) | Role of context in declining symptoms in adulthood for people diagnosed as children | 7 North American sites | Interviews | 125 | 24 (1.7) | 76% male | 72% white, 10% black, 12% mixed |
| Lefler et al. ( ) | What is it like to be a college student and what resources are utilized | United States | Focus groups | 36 | 18–39; median 20 | 66% male | 88% white |
| Liebrenz et al. ( ) | Perceptions of cigarette use | Switzerland | Interviews | 20 | 25–54 | 50% male | – |
| Liebrenz et al. ( ) | Perceptions of smoking cessation and withdrawal | Switzerland | Interviews | 12 | 25–53, 40 | 41% male | |
| Maassen et al. ( ) | What do participants consider to be good healthcare | Netherlands | Focus groups | 30 | – | – | – |
| Matheson et al. ( ) | Experience of diagnosis, treatment, and impairments between those diagnosed as children and adults | United Kingdom | Interviews | 30 | 18–56+ | 43% male | 80% white |
| Meaux et al. ( ) | Factors that help and hinder college students | United States | Interviews | 15 | 18–21 | 60% male | 87% white |
| Meaux et al. ( ) | Experience of stimulant use in college students diagnosed as children | United States | Interviews | 15 | 18–21 | 60% male | 86% white |
| Michielsen et al. ( ) | How ADHD affects lives of older adults unaware of diagnosis | Netherlands | Interviews | 17 | 67–86 | 41% male | – |
| Mitchell et al. ( ) | Factors that delay diagnosis in children and why symptoms may emerge in adulthood | United States | Interviews | 14 | 22–25 | 85% male | 71% white |
| Mitchell et al. ( ) | Relationship between substance use and disrupted emotional functioning in those diagnosed as children | United States | Interviews, mixed methods | 70 | 21–26 | 74% male | 77% white, 10% black, 10% mixed |
| Nehlin et al. ( ) | Perception of substances in people with SUDs | Sweden | Interviews | 14 | 29.6 (7.8), median 25.5 | 42% male | – |
| Nordby et al. ( ) | Experience of participating in a group-based intervention for goal management training | Norway | Interviews | 10 | 21–49 | 70% male | – |
| Nystrom et al. ( ) | Day to day life of people older than 50 | Sweden | Interviews | 10 | 51–74 | 70% female | – |
| Schreuer et al. ( ) | Experiences of women in the workplace; strategies and accommodations used | Israel | Interviews | 11 | 33.5 (6.61) | 100% female | – |
| Schrevel et al. ( ) | Perspectives, problems, and needs in daily life | Netherlands | Focus groups | 52 | 43 (9.5) | 46% male | – |
| Sedgwick et al. ( ) | Positive aspects of ADHD among highly successful adults | United Kingdom | Interviews | 6 | 30–65 | 100% male | |
| Toner et al. ( ) | How people manage their symptoms | Australia | Interviews | 10 | 30–57 | 100% male | – |
| Waite and Tran ( ) | Experience of ethnic minority women in college | United States | Interviews | 16 | 18–45 | 100% female | 31% black 19% Hispanic 6% American Indian 13% Asian 25% other |
| Watters et al. ( ) | Lived experience | Ireland | Interviews | 11 | 20–54, mean 37 | 81% male | – |
| Weisner et al. ( ) | Beliefs on ADHD, stimulant use, and substance use among those diagnosed as children | United States | Interviews | 125 | 24.4 (1.18) | 76% male | 72% white 10% black 12% mixed |
| Young et al. ( ) | Experience of diagnosis in adulthood | United Kingdom | Interviews | 8 | 21–50 (mean 39) | 50% male | – |
1 Ages not reported consistently across studies.
2 Substance use disorder.
An overview of the identified themes is described in Figure 2 , and Table 2 provides a summary of main findings. Several of the themes overlap with each other, and such areas are identified in the main text.

Schematic diagram of the domains of features linked to the lived experiences of adults with ADHD.
Summary of results.
| Adult diagnosis | Process of being diagnosed was laborious and initial misdiagnosis was frequent. | |
| Diagnosis commonly caused feelings of relief as well as identity changes including self-acceptance and emotional turmoil. | ||
| Participants wished they had been diagnosed sooner in life. | ||
| Symptomatology of ADHD | Inattention | Attention was influenced by the environment and interest in the present task; participants did not experience a pervasive deficit of attention. |
| Impulsivity | Resulted in risk-taking and impulsive speech. | |
| Hyperactivity | Less commonly reported; usually inner feelings of restlessness as opposed to physical hyperactivity. | |
| Chaos | Internal feelings of chaos as well as disorganized lives were common. | |
| Structure | Decreased structure in adulthood was difficult to manage. | |
| Emotions | Participants experienced emotional dysregulation, unpleasant emotions, and difficulty recognizing emotions. | |
| Positive aspects of ADHD | ADHD was seen as promoting spontaneity, creativity, energy, and resilience. | |
| Adapting to symptoms | Coping skills | Organization strategies, environmental modifications, physical activity, and awareness of diagnosis were seen as helpful. |
| Medications | Stimulants helped with achieving goals and increasing productivity. | |
| Adverse effects included difficulties socializing, somatic effects, changes in emotion, and rebound symptoms. | ||
| Outside support | Workplace and school accommodations were helpful. | |
| Individual therapy such as CBT was seen as helpful, although it needed to be more tailored to ADHD. | ||
| Support groups were desired to help build community and learn coping skills. | ||
| Substance use | Reasons for substance use | Self-medication and impulsive decision-making contributed to substance use. |
| Quitting | Although a difficult process, quality of life improved after discontinuing substances. | |
| Stimulants and other substances | Stimulants were seen as both a protective factor against substance use and as increasing risk of substance use by different participants. | |
| Perceptions of self and diagnosis | Self-esteem | Low self-esteem due to external pressures was common, although self-esteem often improved in adulthood. |
| Views of ADHD | Some viewed ADHD as a difference instead of a disability; others found the diagnosis limiting. | |
| There were mixed opinions regarding whether participants wished ADHD could be cured. | ||
| Interactions with society | Relationships with others | Participants struggled with interpersonal relationships and feeling different from others. |
| Outside perceptions of ADHD | Stigma about the legitimacy of adult ADHD was common; many did not disclose their diagnosis to others. | |
| Societal expectations | Failure to keep up with activities of daily living resulted in low self-esteem. | |
| Education and occupation | Underachievement was widespread; medications, accommodations, and tailoring tasks to personal interests were seen as helpful. | |
| Accessing services | Receiving medications, counseling, and appointments were difficult to navigate and often required self-advocacy. |
Adult diagnosis
Assessment and diagnosis of adult ADHD were reported as laborious and included prior misdiagnoses ( 20 – 22 ), lack of psychiatric resources ( 23 ), and physicians’ stigma regarding adult ADHD ( 24 ). Participants were often diagnosed only after their children were diagnosed ( 23 , 24 ). However, after receiving a diagnosis, relief was commonly reported initially. Adults noted that receiving a diagnosis helped explain previously seemingly inexplicable symptoms and feelings of being different, and allowed for participants to blame themselves less for perceived shortcomings ( 24 – 31 ).
Identity changes were another reported finding after diagnosis, both positive and negative. Some participants reported experiencing existential questioning of their identities ( 25 , 26 ); others reported feeling increased levels of self-awareness ( 26 , 28 ). Some participants reported having initial doubts about the validity of their diagnoses ( 26 , 28 ). Some reported experiencing emotional turmoil and concerns about the future ( 25 , 26 , 29 ). A commonly reported late step involved acceptance, both of themselves and their diagnoses, sometimes coupled with increased interest in researching ADHD ( 24 , 25 , 28 , 29 , 32 ). A ubiquitous finding was participant regret that they had not been diagnosed earlier, largely because of the many years they had gone without understanding their condition or receiving treatment ( 22 , 24 , 26 – 30 ). In one study, participants who had been diagnosed as children had better emotional control and self-esteem ( 33 ). No studies reported participant regret about their ADHD diagnosis.
Symptomatology of attention-deficit/hyperactivity disorder
Inattention, impulsivity, and hyperactivity.
Consistent with current diagnostic conceptualizations, difficulties with attention and concentration were described. These difficulties hindered completion of daily life tasks at home, school, and work ( 24 , 27 , 28 , 32 , 34 – 37 ). Some participants reported not experiencing a pervasive deficit of attention, but rather only struggling when the topic was not of personal interest and could sustain attention on interesting tasks for long periods of time ( 33 , 38 – 42 ). Attention could be influenced by the environment; for example, attention worsened in distracting environments or improved in intense, stimulating environments ( 40 , 41 ).
Impulsivity was widely reported and reflected in risk-taking including reckless driving, unprotected sex, and extreme sports ( 20 , 24 , 28 , 33 , 36 , 43 ). Impulsive spending was noted ( 20 , 36 – 38 , 44 ). Impulsive speech (“blurting out”) was common and often led to strained interpersonal relationships ( 24 , 32 , 33 , 36 , 37 , 40 ).
Fewer studies described participants’ struggles with hyperactivity, such as with staying still or not being constantly busy ( 24 , 34 , 36 ). Hyperactivity was reported as an internal symptom by some participants, noted as inner feelings of restlessness ( 22 , 36 , 37 , 39 ), or described as resulting in excessive talking ( 36 ). This more subtle hyperactivity was mostly reported by women or older adults.
Chaos, lack of structure, and emotions
Living in chaos was often reported, whether involving internal feelings of being unsettled ( 28 ), or external aspects such as turbulent schedules or disorganized living spaces ( 22 , 24 , 27 , 36 ). Participants often struggled with maintaining structure in daily routines, resulting in irregular sleeping and eating, difficulty completing household tasks, and strained social lives ( 36 – 38 , 43 , 44 ). Increased autonomy in adulthood was often perceived as difficult to manage compared to more highly structured childhoods.
Although lacking from current diagnostic criteria, emotional dysregulation was often noted. Participants reported experiencing extreme emotional reactions to interpersonal conflicts such as terminations of romantic relationships or receiving negative feedback at work ( 24 , 34 , 38 , 40 ). Negative feelings of anxiety and agitation were common ( 22 , 24 , 29 , 31 , 33 , 34 , 36 , 38 , 44 ), as was difficulty with controlling, recognizing, naming, and managing emotions ( 30 , 40 , 41 , 44 ). One study noted that emotional lability has positive aspects since participants’ emotional highs were higher ( 45 ).
Positive aspects of attention-deficit/hyperactivity disorder
Not all aspects of ADHD were perceived as negative. Impulsivity was reported by some as fun and spontaneous ( 26 , 37 , 45 ), struggles with attention were reported as promoting creativity and motivating focus on details ( 21 , 33 , 40 , 41 , 45 ), and hyperactivity was described as providing energy to pursue one’s passions ( 40 , 45 ). Learning to live with ADHD-related impairments was reported as promoting resilience and humanity ( 45 ), and increased tendencies to keep calm in chaotic settings ( 40 ). Ability to maintain focus for extended periods on topics of personal interest was sometimes seen as helpful, although unpredictable ( 33 ).
Adapting to symptoms
Coping skills.
Participants reported compensatory organizational strategies that increased structure in their daily lives. Creating regimented sleeping, eating, working, and relaxing schedules ( 30 , 35 , 42 , 44 , 46 ), and keeping to-do lists or using reminder apps ( 24 , 32 , 37 , 40 , 42 , 46 ) were frequently-reported strategies. Some participants reported thriving without formal structure while working from home since they were able to maintain daily routines and were free from distractions ( 34 ).
Participants reported being able to adjust their environment to best suit their needs, whether that be decreasing distracting stimulation ( 32 , 46 ) or cultivating a highly stressful and stimulating environment ( 39 ). Creating space for physical activity was reported as a helpful outlet for hyperactivity ( 24 , 33 , 39 , 43 , 46 ). Having awareness of their diagnosis allowed newly-diagnosed participants to attribute their symptoms to their disorder, thereby decreasing self-blame ( 24 , 26 , 32 ). In one study, participants engage in self-talk to modify their behavior ( 32 ). Participants reported implementing social skills to prevent interrupting others and adjusting their social circles to accommodate their symptoms ( 24 , 35 , 46 ).
Substance use was also described as a coping strategy, although there were also drawbacks associated with using substances. Such findings are discussed under “substance use.”
Stimulant medications were commonly used to help manage ADHD symptoms; participants reported that stimulants facilitated task prioritization, goal achievement, and productivity often to “life-changing” extents ( 22 , 24 – 27 , 29 , 32 , 35 , 40 , 46 – 48 ). Stimulants were sometimes reported as assisting with social and emotional functioning by promoting calmness ( 22 , 24 , 30 , 40 ). Some participants took their medications on an as-needed basis, choosing to take them only when they had much work ( 20 , 27 , 32 , 33 , 47 ). In one study, participants reported feeling pressured to sell their medication, and in another, participants reported increasing their dosages to stay up all night in order to better complete school work ( 27 , 47 ).
Participant ambivalence or hesitation to take stimulants was reported due to therapeutic and adverse effects. Reported adverse effects included “not feeling like oneself,” resulting in difficulties with socializing and creativity ( 22 , 27 , 35 , 40 , 47 ), somatic effects such as appetite suppression and insomnia ( 22 , 27 , 35 , 40 , 47 ), unpleasant emotions including irritability and numbness ( 35 , 40 , 47 ), and rebound symptoms and withdrawal side effects when the medications wore off ( 29 , 47 ).
Outside support
Studies noted participants adapting to living with their symptoms by receiving formal accommodations at work and school. Reported workplace accommodations included reduction of auditory distractions and bosses who would provide organizational advice or extra reminders about due dates ( 24 , 25 , 40 ). Reported accommodations in college consisted of separate testing environments and extra time on examinations. However, inaccessibility of disability offices, limited willingness of professors to comply with accommodations, and lack of participant engagement with accommodations due to not wanting to seem different resulted in many participants not utilizing such resources ( 27 , 32 ).
Individual therapy was reported as helpful for managing symptoms and acquiring self-knowledge, especially therapeutic interventions designed for ADHD and CBT ( 22 , 23 , 27 , 41 ). However, some participants reported minimal benefits from seeing therapists who did not specialize in ADHD, and CBT was reported to need improvement to be specially tailored to adults with ADHD such as being more engaging or being reframed as ADHD coaching ( 22 , 27 , 33 ). Community care workers added structure to some participants’ lives and aided with motivation in one study ( 42 ).
In some studies, participants expressed desires to be involved with support groups for adults with ADHD in order to learn new coping skills and find community, but not knowing where to access such services ( 28 , 40 ). Those who had participated in ADHD support or focus groups reported feeling validated and less isolated, as well leaving with improved strategies for symptom management ( 24 , 31 , 41 , 49 ). Support was also reported in personal relationships. Having a supportive partner often helped participants tremendously with organization and life tasks, especially for men married to women ( 24 , 43 ). A close friend or family member encouraging accountability and creating a sense of togetherness was viewed as advantageous ( 32 , 42 ).
Substance use and addiction
Reasons for substance use.
The SUDs were commonly reported among adults with ADHD and often seen as a form of self-medication. In every study that discussed self-medication, participants reported using substances to feel calm and relaxed; substances included nicotine/tobacco, alcohol, marijuana, cocaine, and methamphetamine ( 20 , 24 , 32 , 46 , 50 – 52 ). Nicotine/tobacco, marijuana, ecstasy (MDMA), and methamphetamine were used to help improve focus, particularly before diagnosis and subsequent to stimulant treatment ( 20 , 24 , 32 , 51 , 52 ). Participants also reported using substances to help feel “normal” as they facilitated social interactions and helped complete activities of daily life ( 20 , 50 , 52 ). One study described college males’ experiences with video game addictions which resulted in neglecting schoolwork ( 32 ).
The tendencies of people with ADHD to make impulsive decisions were suggested as linking ADHD and substance use ( 20 , 52 ). Substance use worsened ADHD symptoms, most notably impulsivity ( 44 , 52 ). One study attributed high rates of substance use to participants with ADHD being less fearful and more rebellious than individuals without ADHD ( 50 ).
Although discontinuing substance use was regarded as a difficult process with frequent relapses, participants considered their quality of life to improve after quitting ( 30 , 44 , 53 ). Nicotine withdrawal was reported to worsen ADHD symptoms, and participants desired smoking-cessation programs specifically tailored for those with ADHD ( 53 ). Even after discontinuation of substance use, participants reported difficulties accessing stimulant medication due to their substance-use histories ( 52 ).
Stimulants and use of other substances
Findings relating stimulant use and use of other substances were mixed. Prescription stimulant usage was reported as a protective factor against use of other substances. Participants who had previously been self-medicating reported that when they had been on stimulants, they did not need other substances to help them feel calm and focused ( 46 , 47 , 50 , 52 ). Stimulants were reported to decrease cigarette cravings ( 50 ). In one study, a participant commented that her stimulant prescription generated a hatred of taking pills, which she reported subsequently prevented her from using drugs ( 54 ).
Some participants reported stimulant prescriptions as increasing risk of substance use. Some reported that stimulants directly increased nicotine cravings ( 50 ). Indirect connections were reported, such as feelings of social exclusion due to being labeled as medicated or due to participants feeling used to taking drugs since childhood ( 54 ). Other participants reported no connection between stimulant medication and use of other substances ( 50 , 54 ).
Perceptions of self and diagnosis
Self-esteem.
Participants often reported experiencing low self-esteem which they attributed to feeling unable to keep up with work or school, being told they were not good enough by others, and frequently failing at life goals ( 24 , 27 – 29 , 33 , 36 , 37 , 41 , 43 ). Low self-image was typically worse in childhood and improved over time, especially after receiving a diagnosis ( 28 , 36 , 43 ). In one study, some participants did not see themselves as having any flaws despite repeatedly being told otherwise, possibly due to being distracted from the emotional impact of these remarks ( 29 ).
Views of attention-deficit/hyperactivity disorder
Some participants viewed ADHD as a personality trait or difference as opposed to a disorder or disability ( 31 , 32 , 39 , 41 , 45 ). Some participants reported finding the ADHD diagnosis limiting and not wanting the disorder to define who they were ( 27 , 28 ). When asked if they would want their ADHD “cured” in one study, participants’ responses ranged from “definitively yes” to “definitely no.” Many reported feeling ambivalent as they described both positive and negative aspects of ADHD ( 20 ).
Interactions with society
Relationships with others.
Difficulties building and maintaining relationships with others were regularly reported. Participants reported that impulsivity hindered their social interactions due to their tendencies to make inappropriate remarks, engage in reckless behaviors, and agree to engagements without thinking through consequences, resulting in being associated with people to whom they did not want to be linked ( 20 , 22 , 32 , 33 , 36 , 43 ). Reported organizational struggles contributed to participants frequently being late and having cluttered living spaces ( 24 , 38 ). Participants reported misunderstanding social norms and hierarchies and being hesitant about starting conversations ( 28 , 30 , 40 , 43 ). They reported feeling overwhelmed by others’ emotions and unsure how to respond to them ( 44 ). Some participants reported choosing to hide their ADHD diagnoses, and the resultant barrier made socializing feel exhausting ( 24 ). Participants reported that these factors made sustaining long-term relationships especially difficult ( 22 , 31 , 38 , 43 ).
Feeling different from others was widely reported, most notably in childhood ( 20 , 24 , 27 , 29 , 31 , 32 ). This experience was described as feeling misunderstood, like a misfit, abnormal, and/or like there was something wrong with them ( 20 , 24 , 27 , 29 , 33 , 43 , 45 , 50 ). Participants reported consciously pretending to be normal as an attempt to fit in ( 28 , 41 ). Some participants reported seeing themselves as more brave or rebellious than their peers, which sometimes resulted in positive self-images ( 24 , 36 , 50 ). A strong desire to advocate for “the underdog” in interpersonal relationships was described by some women ( 31 ). In one study, most participants did not describe feeling different from others, but reported having felt misunderstood as children ( 36 ).
Participants with ADHD who also had children diagnosed with ADHD reported that their approaches to their children’s diagnoses were shaped by their own ADHD experiences. Parents reported uniform support of diagnostic testing, although the best time for testing was not agreed-upon ( 26 , 48 ). Opinions on starting their children on stimulants varied, ranging from enthusiastic support to viewing medication as a last resort, even among participants who had responded positively to stimulants themselves ( 48 ). Most participants reported supporting shared decision-making with the child.
Outside perceptions of attention-deficit/hyperactivity disorder
Participants reported their social networks often expressed preconceived notions about the diagnosis, such as ADHD being “fake” or restricted to children ( 27 – 29 , 37 , 41 ). Stigma about ADHD was reported as having prevented many from disclosing their diagnosis both personally and professionally ( 24 , 26 , 28 , 29 , 32 ). Increased awareness and education about ADHD were desired by participants to help them function better in society ( 28 , 41 ).
Societal expectations
Some studies discussed participants’ difficulties with meeting societal expectations. Participants reported struggling to keep up with daily tasks such as maintaining their living spaces, paying bills and remembering to eat ( 28 , 33 , 35 , 41 ). These difficulties were reported to result in exasperation, low self-esteem, and exhaustion ( 29 , 33 ).
Education and occupation
Academic underachievement was widely reported; most studies focused on postsecondary education. Some participants reported having to try harder than their peers for the same results ( 28 , 35 ), while others reported that they fell behind due to not putting in much effort ( 24 , 27 ). Reports of low motivation to complete assignments until the last minute, as it then became easier to focus, led to missed deadlines ( 32 , 35 , 38 ). Participants reported difficulties paying attention in class ( 24 , 27 , 32 , 35 ), struggling with reading comprehension ( 27 , 32 ), and needing extra tutoring ( 24 , 28 ). Participants reported these difficulties prevented them from “reaching their potential” as they were unable to complete advanced courses or degrees necessary for their careers of choice ( 20 , 22 , 31 , 37 , 39 ). A third of participants in one study noted that they did not struggle academically ( 31 ). Reported coping mechanisms for mitigating academic impairment included medications ( 35 , 47 ), active engagement with materials facilitated by small class sizes or study groups ( 23 , 35 ), and studying from home with fewer distractions ( 34 ). Formal academic accommodations are discussed under the outside support subheading of adapting to symptoms.
Occupational struggles were commonly reported, with many studies detailing participant underemployment or unemployment and high job-turnover rates ( 22 , 31 , 33 , 37 , 41 , 43 ). Difficulties with punctuality and keeping up with tasks and deadlines were reported to generate tensions in the workplace ( 20 , 22 , 24 , 33 , 35 , 39 ), and participants reported frequently being bored and unable to stay focused on their responsibilities, with noisy workplaces promoting distractibility ( 20 , 24 , 33 , 35 , 39 , 40 ). Some studies noted difficulties understanding and navigating social hierarchies in the workplace ( 20 , 40 ). In one study, participants reported feeling unable to maintain work-life balance, overworking until they felt burnt out ( 36 ). Working in fields of intrinsic interest, multitasking, and self-employment were reported strategies used to achieve occupational success ( 24 , 31 , 40 ). Having an understanding employer who could assist with task delegation and understand their needs was described as promoting positive workplace dynamics ( 25 , 33 , 40 ). Clearly defied roles and working with others helped some participants remain engaged in work ( 42 ). College students often reported part-time jobs as rewarding, with responsibilities helping them manage their academic pursuits ( 35 ).
Accessing services
Adults described difficulties accessing healthcare for ADHD. Most reported having to fight to receive a diagnosis and medication due to perceptions of stigma from physicians about adult ADHD ( 22 ). After diagnosis, participants often felt they did not receive adequate counseling or follow-up, especially when seeing general practitioners ( 22 , 26 ). Many participants reported not seeing physicians regularly for medication management due to bureaucratic difficulties ( 21 ); college students reported often having their former pediatricians refill prescriptions without regular appointments ( 47 ). Many participants in one study had little knowledge of ADHD services available to them despite regular appointments ( 32 ).
This review characterizes the current literature on the lived experiences of adults with ADHD. This includes experiences of having been diagnosed as an adult, symptomatology of adult ADHD, skills used to adapt to ADHD symptoms, relationships between ADHD and substance use, individual perceptions of self and of having received ADHD diagnoses, and social experiences interacting in society.
Similar themes were noted in a previous review on lived experiences of adults with ADHD consisting of ten studies, three of which were included here ( 17 ). Such themes included participants feeling different from others, perceiving themselves as creative, and implementing coping skills. There were also other similar findings from a review of eleven studies on the experiences of adolescents with ADHD ( 55 ). Overlapping themes included participants feeling that ADHD symptomatology has some benefits, experiencing difficulties with societal expectations, emotions and interpersonal conflicts, struggling with identity and stigma, and having varying experiences with stimulants. The overlaps in findings from these two reviews suggest there are shared experiences between adolescents and adults with ADHD. Unique from previous reviews on lived experiences of people with ADHD are the present qualitative findings of experiences of having received diagnoses in adulthood, reflections on ADHD and substance use, occupational struggles, attention dysregulation, and emotional symptoms of ADHD.
The relationship between ADHD effects and poor occupational performance has been previously described. People with ADHD often struggle with unemployment and underemployment and functional impairment at work ( 56 – 58 ). The findings of this review suggest that adults with ADHD may benefit from workplace accommodations and from decreased stigma around adult ADHD.
Findings suggest that people with ADHD often experience attention dysregulation as opposed to attention deficits, per se . This notion builds on previous clinical observations ( 59 ) and quantitative literature ( 60 , 61 ) documenting that adults with ADHD may hyperfocus on tasks of interest. These findings suggest that inattention does not fully capture the attentional symptoms of the condition and suggest a possible need for updated diagnostic criteria.
Emotional dysregulation was described by many studies in this review, and there were no studies in which participants denied struggling with emotions. These findings provide support for a conceptual model of ADHD that presents emotional dysregulation as a core feature of ADHD, as opposed to models stating that emotional dysregulation is a subtype of ADHD or simply that the domains are correlated ( 62 ). Debates exist regarding whether or not specific clinical aspects of disorders constitute core or diagnostic features ( 63 ). The DSM-5 and ICD-11 have viewed differently the criteria for specific disorders, including with respect to engagement for emotional regulation or stress-reduction purposes [e.g., behavioral addictions like gambling and gaming disorders, and other behaviors relating to compulsive sexual engagement ( 3 , 64 , 65 )]. Because emotional dysregulation is often overlooked as being associated with ADHD, patients experiencing such symptoms may be mistaken for having other conditions such as mood or personality disorders. Appreciating the emotional symptoms of ADHD may help psychiatrists, psychologists, and social workers more accurately diagnose ADHD in adults and decrease misdiagnosis.
The recurrent themes of difficulty naming and recognizing emotions found here suggest that ADHD may be associated with alexithymia. One study found that 22% of adults with ADHD were highly alexithymic but their mean scores on the rating scale for alexithymia were not significantly different from controls ( 66 ). Parenting style, attachment features, and ADHD symptoms have been found to predict emotional processing and alexithymia measures among adults with ADHD ( 67 ). More research is needed into the relationship between ADHD symptoms and alexithymia.
There was considerable heterogeneity in wishes regarding cures for ADHD (suggesting both perceived benefits and detriments) and stimulant use being association with SUDs. From a clinical perspective, both points will be important to understand better. With regard to the latter, ADHD and SUDs frequently co-occur; one meta-analysis found that 23% of people with SUDs met criteria for ADHD ( 68 ). Furthermore, youth with ADHD are seven-fold more likely than those without to experience/develop SUDs; however, early treatment with stimulants appeared to decrease this risk ( 69 ). Understanding better motivations for substance use in adults with ADHD as may be gleaned through considering lived experiences may help decrease ADHD/SUD co-occurrence and improve quality of life.
This review highlights gaps in the qualitative literature on adult ADHD. Nearly all included studies took place in Europe, North America or Asia; there is a dearth of qualitative research on ADHD in the Global South. Although most studies did not report race, those that did often had a majority of White participants. Racial/ethnic disparities in ADHD diagnosis may contribute to the relatively low diversity of study participants ( 9 ), and such disparities are further reason to expand research focused on non-White individuals with ADHD. Most studies focused on young or middle-aged adults and most participants were male; more research is needed on how ADHD may impact older adults and other gender identities. Although long considered to disproportionately affect male children at approximately 3:1 ( 70 ), ADHD in adults has been reported to have gender ratios of 1.5:1 ( 71 ). Among the adult psychiatric population, some studies have found no gender difference in prevalence or up to a 2.5:1 female predominance ( 72 ). This finding suggests that women often may not receive diagnoses until adulthood and there may be strong links with other psychopathologies in women. The lived experience of women with ADHD should be further examined; this insight may help to understand why women often go undiagnosed and experience other psychiatric concerns.
Future qualitative studies should explore how ADHD symptoms change over the lifespan as this was not addressed in any of the included studies. There were very few findings relating to how adults with ADHD conceptualize the condition and how their diagnosis interacts with their identities. Some studies reported on difficulties adults with ADHD have with accessing services; further exploration is needed into how the medical community can better meet the needs of this population. Findings from this review may be used to inform future ADHD screening tools. The Adult ADHD Self-Report Scale (ASRS) is a widely used screening tool that covers symptoms of inattention, impulsivity, and hyperactivity ( 73 ). This review suggests that symptoms may be more expansive than what is included in the ASRS and that questions on attentional dysregulation and hyperfocusing, emotional dysregulation, internal chaos, low self-esteem, and strained interpersonal relationships could be tested for validity for inclusion. The Conners’ Adult ADHD Rating Scales (CAARS) includes questions on emotional lability and low self-esteem in addition to symptoms covered by the ASRS ( 74 ), although the scale has been found to have high false-positive and false-negative rates ( 75 ). Further studies are needed to develop screening tools that capture the lived experience of adults with ADHD while maintaining appropriate sensitivity and specificity. This review may also inform tailoring CBT and other therapeutic interventions for ADHD. For example, CBT may help develop skills for volitional hyperfocusing on productive tasks instead of feeling pulled away from daily activities.
This study has limitations. Being a rapid review, it was not an exhaustive search of the available literature and may have missed some relevant studies that would have been identified by a systematic search. The search strategy consisted of ADHD and qualitative research methods; studies that did not include “qualitative” in their titles or abstracts may not have been identified. This may explain why the previous review on the lived experiences of adults with ADHD ( 17 ) included studies not identified by this search. Although a formal quality appraisal was completed, all studies were included regardless of the quality assessment as to not further narrow the review. For example, studies were not excluded based on how they verified ADHD diagnosis as many studies did not specify if or how this was completed. Although restricting studies based on quality metrics may have made the present findings more robust, the amount of data that would have been excluded would have been considerable and may have resulted in omitting important findings. These variable quality metrics not only limit the findings of the present review, but also speak to limitations in the methodological rigor of qualitative research on adult ADHD.
Attention-deficit/hyperactivity disorder is a relatively common diagnosis among adults. Exploration of the lived experiences of adults with ADHD may illuminate the breadth of symptomatology of the condition and should be considered in the diagnostic criteria for adults. Understanding symptomatology of adults with ADHD and identifying areas of unmet need may help guide intervention development to improve the quality of life of adults with ADHD.
Author contributions
CG and MP contributed to the conception of the review. CG and GM-G performed the abstract and full text screening. CG performed the data synthesis and wrote the first draft of the manuscript. GM-G, GA, KB, and MP contributed to the revising and editing the manuscript. All authors read and approved the submitted version.
Acknowledgments
We would like to express gratitude to clinical librarian Courtney Brombosz for her assistance in developing the search strategy.
This work was supported by the Yale School of Medicine Office of Student Research One-Year Fellowship and the K12 DA000167 grant.
Conflict of interest
MP has consulted for and advised Opiant Pharmaceuticals, Idorsia Pharmaceuticals, BariaTek, AXA, Game Day Data, and the Addiction Policy Forum; has been involved in a patent application with Yale University and Novartis; has received research support from the Mohegan Sun Casino and Connecticut Council on Problem Gambling; has participated in surveys, mailings or telephone consultations related to drug addiction, impulse control disorders or other health topics; and has consulted for law offices and gambling entities on issues related to impulse control or addictive disorders. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.949321/full#supplementary-material
- Introduction
- Conclusions
- Article Information
ADHD indicates attention-deficit/hyperactivity disorder; CVD, cardiovascular disease.
a Controls were derived from the same base cohort as the cases; thus, a case with a later date of CVD diagnosis could potentially serve as a control for another case in the study.
Crude odds ratios (ORs) were based on cases and controls matched on age, sex, and calendar time. Adjusted ORs (AORs) were based on cases and controls matched on age, sex, and calendar time and adjusted for country of birth, educational level, somatic comorbidities (type 2 diabetes, obesity, dyslipidemia, and sleep disorders), and psychiatric comorbidities (anxiety disorders, autism spectrum disorder, bipolar disorder, conduct disorder, depressive disorder, eating disorders, intellectual disability, personality disorders, schizophrenia, and substance use disorders).
The solid lines represent the adjusted odds ratios, and the shaded areas represent the 95% CIs. In restricted cubic splines analysis, knots were placed at the 10th, 50th, and 90th percentiles of ADHD medication use.
eTable 1. International Classification of Diseases (ICD) Codes from the Swedish National Inpatient Register
eTable 2. Type of Cardiovascular Disease in Cases
eTable 3. Risk of CVD Associated With ADHD Medication Use Across Different Average Defined Daily Doses
eTable 4. Risk of CVD Associated With Cumulative Duration of Use of Different Types of ADHD Medications
eTable 5. Sensitivity Analyses of CVD Risk Associated With Cumulative Use of ADHD Medications, Based On Different Cohort, Exposure, and Outcome Definitions
eFigure. Risk of CVD Associated With Cumulative Use of ADHD Medications, Stratified by Sex
Data Sharing Statement
- Long-Term ADHD Medications and Cardiovascular Disease Risk JAMA Medical News in Brief December 26, 2023 Emily Harris
- Long-Term Cardiovascular Effects of Medications for ADHD—Balancing Benefits and Risks of Treatment JAMA Psychiatry Editorial February 1, 2024 Samuele Cortese, MD, PhD; Cristiano Fava, MD, PhD
See More About
Select your interests.
Customize your JAMA Network experience by selecting one or more topics from the list below.
- Academic Medicine
- Acid Base, Electrolytes, Fluids
- Allergy and Clinical Immunology
- American Indian or Alaska Natives
- Anesthesiology
- Anticoagulation
- Art and Images in Psychiatry
- Artificial Intelligence
- Assisted Reproduction
- Bleeding and Transfusion
- Caring for the Critically Ill Patient
- Challenges in Clinical Electrocardiography
- Climate and Health
- Climate Change
- Clinical Challenge
- Clinical Decision Support
- Clinical Implications of Basic Neuroscience
- Clinical Pharmacy and Pharmacology
- Complementary and Alternative Medicine
- Consensus Statements
- Coronavirus (COVID-19)
- Critical Care Medicine
- Cultural Competency
- Dental Medicine
- Dermatology
- Diabetes and Endocrinology
- Diagnostic Test Interpretation
- Drug Development
- Electronic Health Records
- Emergency Medicine
- End of Life, Hospice, Palliative Care
- Environmental Health
- Equity, Diversity, and Inclusion
- Facial Plastic Surgery
- Gastroenterology and Hepatology
- Genetics and Genomics
- Genomics and Precision Health
- Global Health
- Guide to Statistics and Methods
- Hair Disorders
- Health Care Delivery Models
- Health Care Economics, Insurance, Payment
- Health Care Quality
- Health Care Reform
- Health Care Safety
- Health Care Workforce
- Health Disparities
- Health Inequities
- Health Policy
- Health Systems Science
- History of Medicine
- Hypertension
- Images in Neurology
- Implementation Science
- Infectious Diseases
- Innovations in Health Care Delivery
- JAMA Infographic
- Law and Medicine
- Leading Change
- Less is More
- LGBTQIA Medicine
- Lifestyle Behaviors
- Medical Coding
- Medical Devices and Equipment
- Medical Education
- Medical Education and Training
- Medical Journals and Publishing
- Mobile Health and Telemedicine
- Narrative Medicine
- Neuroscience and Psychiatry
- Notable Notes
- Nutrition, Obesity, Exercise
- Obstetrics and Gynecology
- Occupational Health
- Ophthalmology
- Orthopedics
- Otolaryngology
- Pain Medicine
- Palliative Care
- Pathology and Laboratory Medicine
- Patient Care
- Patient Information
- Performance Improvement
- Performance Measures
- Perioperative Care and Consultation
- Pharmacoeconomics
- Pharmacoepidemiology
- Pharmacogenetics
- Pharmacy and Clinical Pharmacology
- Physical Medicine and Rehabilitation
- Physical Therapy
- Physician Leadership
- Population Health
- Primary Care
- Professional Well-being
- Professionalism
- Psychiatry and Behavioral Health
- Public Health
- Pulmonary Medicine
- Regulatory Agencies
- Reproductive Health
- Research, Methods, Statistics
- Resuscitation
- Rheumatology
- Risk Management
- Scientific Discovery and the Future of Medicine
- Shared Decision Making and Communication
- Sleep Medicine
- Sports Medicine
- Stem Cell Transplantation
- Substance Use and Addiction Medicine
- Surgical Innovation
- Surgical Pearls
- Teachable Moment
- Technology and Finance
- The Art of JAMA
- The Arts and Medicine
- The Rational Clinical Examination
- Tobacco and e-Cigarettes
- Translational Medicine
- Trauma and Injury
- Treatment Adherence
- Ultrasonography
- Users' Guide to the Medical Literature
- Vaccination
- Venous Thromboembolism
- Veterans Health
- Women's Health
- Workflow and Process
- Wound Care, Infection, Healing
Others Also Liked
- Download PDF
- X Facebook More LinkedIn
Zhang L , Li L , Andell P, et al. Attention-Deficit/Hyperactivity Disorder Medications and Long-Term Risk of Cardiovascular Diseases. JAMA Psychiatry. 2024;81(2):178–187. doi:10.1001/jamapsychiatry.2023.4294
Manage citations:
© 2024
- Permissions
Attention-Deficit/Hyperactivity Disorder Medications and Long-Term Risk of Cardiovascular Diseases
- 1 Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden
- 2 Unit of Cardiology, Heart and Vascular Division, Department of Medicine, Karolinska University Hospital, Karolinska Institutet, Stockholm, Sweden
- 3 School of Medical Sciences, Faculty of Medicine and Health, Örebro University, Örebro, Sweden
- 4 Department of Applied Health Science, School of Public Health, Indiana University, Bloomington
- 5 Department of Psychological and Brain Sciences, Indiana University, Bloomington
- Editorial Long-Term Cardiovascular Effects of Medications for ADHD—Balancing Benefits and Risks of Treatment Samuele Cortese, MD, PhD; Cristiano Fava, MD, PhD JAMA Psychiatry
- Medical News in Brief Long-Term ADHD Medications and Cardiovascular Disease Risk Emily Harris JAMA
Question Is long-term use of attention-deficit/hyperactivity disorder (ADHD) medication associated with an increased risk of cardiovascular disease (CVD)?
Findings In this case-control study of 278 027 individuals in Sweden aged 6 to 64 years who had an incident ADHD diagnosis or ADHD medication dispensation, longer cumulative duration of ADHD medication use was associated with an increased risk of CVD, particularly hypertension and arterial disease, compared with nonuse.
Meaning Findings of this study suggest that long-term exposure to ADHD medications was associated with an increased risk of CVD; therefore, the potential risks and benefits of long-term ADHD medication use should be carefully weighed.
Importance Use of attention-deficit/hyperactivity disorder (ADHD) medications has increased substantially over the past decades. However, the potential risk of cardiovascular disease (CVD) associated with long-term ADHD medication use remains unclear.
Objective To assess the association between long-term use of ADHD medication and the risk of CVD.
Design, Setting, and Participants This case-control study included individuals in Sweden aged 6 to 64 years who received an incident diagnosis of ADHD or ADHD medication dispensation between January 1, 2007, and December 31, 2020. Data on ADHD and CVD diagnoses and ADHD medication dispensation were obtained from the Swedish National Inpatient Register and the Swedish Prescribed Drug Register, respectively. Cases included individuals with ADHD and an incident CVD diagnosis (ischemic heart diseases, cerebrovascular diseases, hypertension, heart failure, arrhythmias, thromboembolic disease, arterial disease, and other forms of heart disease). Incidence density sampling was used to match cases with up to 5 controls without CVD based on age, sex, and calendar time. Cases and controls had the same duration of follow-up.
Exposure Cumulative duration of ADHD medication use up to 14 years.
Main Outcomes and Measures The primary outcome was incident CVD. The association between CVD and cumulative duration of ADHD medication use was measured using adjusted odds ratios (AORs) with 95% CIs.
Results Of 278 027 individuals with ADHD aged 6 to 64 years, 10 388 with CVD were identified (median [IQR] age, 34.6 [20.0-45.7] years; 6154 males [59.2%]) and matched with 51 672 control participants without CVD (median [IQR] age, 34.6 [19.8-45.6] years; 30 601 males [59.2%]). Median (IQR) follow-up time in both groups was 4.1 (1.9-6.8) years. Longer cumulative duration of ADHD medication use was associated with an increased risk of CVD compared with nonuse (0 to ≤1 year: AOR, 0.99 [95% CI, 0.93-1.06]; 1 to ≤2 years: AOR, 1.09 [95% CI, 1.01-1.18]; 2 to ≤3 years: AOR, 1.15 [95% CI, 1.05-1.25]; 3 to ≤5 years: AOR, 1.27 [95% CI, 1.17-1.39]; and >5 years: AOR, 1.23 [95% CI, 1.12-1.36]). Longer cumulative ADHD medication use was associated with an increased risk of hypertension (eg, 3 to ≤5 years: AOR, 1.72 [95% CI, 1.51-1.97] and >5 years: AOR, 1.80 [95% CI, 1.55-2.08]) and arterial disease (eg, 3 to ≤5 years: AOR, 1.65 [95% CI, 1.11-2.45] and >5 years: AOR, 1.49 [95% CI, 0.96-2.32]). Across the 14-year follow-up, each 1-year increase of ADHD medication use was associated with a 4% increased risk of CVD (AOR, 1.04 [95% CI, 1.03-1.05]), with a larger increase in risk in the first 3 years of cumulative use (AOR, 1.08 [95% CI, 1.04-1.11]) and stable risk over the remaining follow-up. Similar patterns were observed in children and youth (aged <25 years) and adults (aged ≥25 years).
Conclusions and Relevance This case-control study found that long-term exposure to ADHD medications was associated with an increased risk of CVDs, especially hypertension and arterial disease. These findings highlight the importance of carefully weighing potential benefits and risks when making treatment decisions about long-term ADHD medication use. Clinicians should regularly and consistently monitor cardiovascular signs and symptoms throughout the course of treatment.
Attention-deficit/hyperactivity disorder (ADHD) is a common psychiatric disorder characterized by developmentally inappropriate inattentiveness, impulsivity, and hyperactivity. 1 , 2 Pharmacological therapy, including both stimulants and nonstimulants, is recommended as the first-line treatment for ADHD in many countries. 1 , 3 The use of ADHD medication has increased greatly in both children and adults during the past decades. 4 Although the effectiveness of ADHD medications has been demonstrated in randomized clinical trials (RCTs) and other studies, 5 , 6 concerns remain regarding their potential cardiovascular safety. 7 Meta-analyses of RCTs have reported increases in heart rate and blood pressure associated with both stimulant and nonstimulant ADHD medications. 5 , 7 - 9
As RCTs typically evaluate short-term effects (average treatment duration of 75 days), 7 it remains uncertain whether and to what extent the increases in blood pressure and heart rate associated with ADHD medication lead to clinically significant cardiovascular disease (CVD) over time. Longitudinal observational studies 10 - 12 examining the association between ADHD medication use and serious cardiovascular outcomes have emerged in recent years, but the findings have been mixed. A meta-analysis 13 of observational studies found no statistically significant association between ADHD medication and risk of CVD. However, the possibility of a modest risk increase cannot be ruled out due to several methodological limitations in these studies, including confounding by indication, immortal time bias, and prevalent user bias. Additionally, most of these studies had an average follow-up time of no more than 2 years. 13 , 14 Thus, evidence regarding the long-term cardiovascular risk of ADHD medication use is still lacking.
Examining the long-term cardiovascular risk associated with ADHD medicine use is clinically important given that individuals with a diagnosis of ADHD, regardless of whether they receive treatment, face an elevated risk of CVD. 15 Additionally, a substantial proportion of young individuals with ADHD continues to have impairing symptoms in adulthood, 16 necessitating prolonged use of ADHD medication. Notably, studies have indicated a rising trend in the long-term use of ADHD medications, with approximately half of individuals using ADHD medication for over 5 years. 17 Furthermore, evidence is lacking regarding how cardiovascular risk may vary based on factors such as type of CVD, type of ADHD medication, age, and sex. 13 Therefore, there is a need for long-term follow-up studies to address these knowledge gaps and provide a more comprehensive understanding of the cardiovascular risks associated with ADHD medication use. This information is also crucial from a public health perspective, particularly due to the increasing number of individuals receiving ADHD medications worldwide. 4
This study aimed to assess the association between cumulative use of ADHD medication up to 14 years and the risk of CVD by using nationwide health registers in Sweden. We hypothesized that longer cumulative use of ADHD medication would be associated with increased CVD risk. In addition, we aimed to examine whether the associations differ across types of ADHD medication, types of CVD, sex, and age groups.
We used data from several Swedish nationwide registers linked through unique personal identification numbers. 18 Diagnoses were obtained from the National Inpatient Register, 19 which contains data on inpatient diagnoses since 1973 and outpatient diagnoses since 2001. Information on prescribed medications was retrieved from the Swedish Prescribed Drug Register, which contains all dispensed medications in Sweden since July 2005 and includes information on drug identity based on the Anatomical Therapeutic Chemical (ATC) classification, 20 dispensing dates, and free-text medication prescriptions. Socioeconomic factors were obtained from the Longitudinal Integrated Database for Health Insurance and Labour Market studies. 21 Information on death was retrieved from the Swedish Cause of Death Register, 22 which contains information on all deaths since 1952. The study was approved by the Swedish Ethical Review Authority. Informed patient consent is not required for register-based studies in Sweden. The study followed the Reporting of Studies Conducted Using Observational Routinely Collected Health Data–Pharmacoepidemiological Research ( RECORD-PE ) guideline. 23
We conducted a nested case-control study of all individuals residing in Sweden aged 6 to 64 years who received an incident diagnosis of ADHD or ADHD medication dispensation 15 between January 1, 2007, and December 31, 2020. The diagnosis of ADHD ( International Statistical Classification of Diseases and Related Health Problems, Tenth Revision [ ICD-10 ] code F90) was identified from the National Inpatient Register. Incident ADHD medication dispensation was identified from the Swedish Prescribed Drug Register and was defined as a dispensation after at least 18 months without any ADHD medication dispensation. 24 Baseline (ie, cohort entry) was defined as the date of incident ADHD diagnosis or ADHD medication dispensation, whichever came first. Individuals with ADHD medication prescriptions for indications other than ADHD 25 and individuals who emigrated, died, or had a history of CVD before baseline were excluded from the study. The cohort was followed until the case index date (ie, the date of CVD diagnosis), death, migration, or the study end date (December 31, 2020), whichever came first.
Within the study cohort, we identified cases as individuals with an incident diagnosis of any CVD (including ischemic heart diseases, cerebrovascular diseases, hypertension, heart failure, arrhythmias, thromboembolic disease, arterial disease, and other forms of heart disease; eTable 1 in Supplement 1 ) during follow-up. For each case, the date of their CVD diagnosis was assigned as the index date. Using incidence density sampling, 26 up to 5 controls without CVD were randomly selected for each case from the base cohort of individuals with ADHD. The matching criteria included age, sex, and calendar time, ensuring that cases and controls had the same duration of follow-up from baseline to index date. Controls were eligible for inclusion if they were alive, living in Sweden, and free of CVD at the time when their matched case received a diagnosis of CVD, with the index date set as the date of CVD diagnosis of the matched case ( Figure 1 ). Controls were derived from the same base cohort as the cases. Thus, a case with a later date of CVD diagnosis could potentially serve as a control for another case in the study. 26
The main exposure was cumulative duration of ADHD medication use, which included all ADHD medications approved in Sweden during the study period, including stimulants (methylphenidate [ATC code N06BA04], amphetamine [ATC code N06BA01], dexamphetamine [ATC code N06BA02], and lisdexamfetamine [ATC code N06BA12]) as well as nonstimulants (atomoxetine [ATC code N06BA09] and guanfacine [ATC code C02AC02]). Duration of ADHD medication use was derived from a validated algorithm that estimates treatment duration from free text in prescription records. 25 The cumulative duration of ADHD medication use was calculated by summing all days covered by ADHD medication between baseline and 3 months prior to the index date. The last 3 months before the index date were excluded to reduce reverse causation, as clinicians’ perception of potential cardiovascular risks may influence ADHD medication prescription. This time window was chosen because routine psychiatric practice in Sweden limits a prescription to a maximum 3 months at a time. 27 Individuals with follow-up of less than 3 months were excluded.
We conducted conditional logistic regression analyses to estimate odds ratios (ORs) for the associations between cumulative durations of ADHD medication use and incident CVD. Crude ORs were adjusted for all matching variables (age, sex, and calendar time) by design. Adjusted ORs (AORs) were additionally controlled for country of birth (Sweden vs other), highest educational level (primary or lower secondary, upper secondary, postsecondary or postgraduate, or unknown; individuals aged <16 years were included as a separate category), and diagnoses of somatic (type 2 diabetes, obesity, dyslipidemia, and sleep disorders) and psychiatric comorbidities (anxiety disorders, autism spectrum disorder, bipolar disorder, conduct disorder, depressive disorder, eating disorders, intellectual disability, personality disorders, schizophrenia, and substance use disorders; eTable 1 in Supplement 1 ) before baseline. The association between cumulative ADHD medication use and incident CVD was assessed using both continuous and categorical measures (no ADHD medication use, 0 to ≤1, 1 to ≤2, 2 to ≤3, 3 to ≤5, and >5 years). To capture potential nonlinear associations, we used restricted cubic splines to examine ADHD medication use as a continuous measure throughout follow-up. 28 The associations were examined in the full sample and stratified by age at baseline, that is, children or youth (<25 years old) and adults (≥25 years old). Furthermore, to evaluate the association with dosage of ADHD medication, we estimated the risk of CVD associated with each 1-year increase in use of ADHD medication across different dosage groups categorized by the average defined daily dose (DDD; for instance, 1 DDD of methylphenidate equals 30 mg) during follow-up. 29
In subgroup analyses, we examined the associations between ADHD medication use and specific CVDs, including arrhythmias, arterial disease, cerebrovascular disease, heart failure, hypertension, ischemic heart disease, and thromboembolic disease (eTable 1 in Supplement 1 ). Additionally, we investigated the associations with CVD risk for the most commonly prescribed ADHD medications in Sweden, ie, methylphenidate, lisdexamfetamine, and atomoxetine, while adjusting for other ADHD medication use. We also examined sex-specific associations.
To further examine the robustness of our findings, we conducted 4 sensitivity analyses. First, we restricted the sample to ever users of ADHD medication to reduce unmeasured confounding between ADHD medication users and nonusers. Second, we assessed ADHD medication exposure over the entire follow-up period without excluding the 3 months prior to the index date. Third, to capture fatal cardiovascular events, we additionally included death by CVD in the outcome definition. Finally, we constructed a conditional logistic regression model that adjusted for propensity scores of ADHD medication use. Data management was performed using SAS, version 9.4 (SAS Institute Inc) and all analyses were performed using R, version 4.2.3 (R Foundation for Statistical Computing).
The study cohort consisted of 278 027 individuals with ADHD aged 6 to 64 years. The incidence rate of CVD was 7.34 per 1000 person-years. After applying exclusion criteria and matching, the analysis included 10 388 cases (median [IQR] age at baseline, 34.6 (20.0-45.7) years; 6154 males [59.2%] and 4234 females [40.8%]) and 51 672 matched controls (median [IQR] age at baseline, 34.6 [19.8-45.6] years; 30 601 males [59.2%] and 21 071 females [40.8%]) ( Figure 1 and Table 1 ). Median (IQR) follow-up in both groups was 4.1 (1.9-6.8) years. Among the controls, 3363 had received a CVD diagnosis after their index dates. The most common types of CVD in cases were hypertension (4210 cases [40.5%]) and arrhythmias (1310 cases [12.6%]; eTable 2 in Supplement 1 ). Table 1 presents the sociodemographic information and somatic and psychiatric comorbidities in cases and controls. In general, cases had higher rates of somatic and psychiatric comorbidities and a lower level of educational attainment compared with controls.
A similar proportion of cases (83.9%) and controls (83.5%) used ADHD medication during follow-up, with methylphenidate being the most commonly dispensed type, followed by atomoxetine and lisdexamfetamine. Longer cumulative duration of ADHD medication use was associated with an increased risk of CVD compared with nonuse (0 to ≤1 year: AOR, 0.99 [95% CI, 0.93-1.06]; 1 to ≤2 years: AOR, 1.09 [95% CI, 1.01-1.18]; 2 to ≤3 years: AOR, 1.15 [95% CI, 1.05-1.25]; 3 to ≤5 years: AOR, 1.27 [95% CI, 1.17-1.39]; and >5 years: AOR, 1.23 [95% CI, 1.12-1.36]) ( Figure 2 ). The restricted cubic spline model suggested a nonlinear association, with the AORs increasing rapidly for the first 3 cumulative years of ADHD medication use and then becoming stable thereafter ( Figure 3 ). Throughout the entire follow-up, each 1-year increase in the use of ADHD medication was associated with a 4% increased risk of CVD (AOR, 1.04 [95% CI, 1.03-1.05]), and the corresponding increase for the first 3 years was 8% (AOR, 1.08 [95% CI, 1.04-1.11]). We observed similar results when examining children or youth and adults separately ( Figure 2 ). The restricted cubic spline model suggested a similar nonlinear association, with higher AORs in children or youth than in adults, but the 95% CIs largely overlapped ( Figure 3 ). Furthermore, similar associations were observed for females and males (eFigure in Supplement 1 ). The dosage analysis showed that the risk of CVD associated with each 1 year of ADHD medication use increased with higher average DDDs. The risk was found to be statistically significant only among individuals with a mean dose of at least 1.5 times the DDD (eTable 3 in Supplement 1 ). For example, among individuals with a mean DDD of 1.5 to 2 or less (eg, for methylphenidate, 45 to ≤60 mg), each 1-year increase in ADHD medication use was associated with a 4% increased risk of CVD (AOR, 1.04 [95% CI, 1.02-1.05]). Among individuals with a mean DDD >2 (eg, for methylphenidate >60 mg), each 1-year increase in ADHD medication use was associated with 5% increased risk of CVD (AOR, 1.05 [95% CI, 1.03-1.06]).
When examining the risk for specific CVDs, we found that long-term use of ADHD medication (compared with no use) was associated with an increased risk of hypertension (AOR, 1.72 [95% CI, 1.51-1.97] for 3 to ≤5 years; AOR, 1.80 [95% CI 1.55-2.08] for >5 years) ( Table 2 ), as well as arterial disease (AOR, 1.65 [95% CI, 1.11-2.45] for 3 to ≤5 years; AOR, 1.49 [95% CI 0.96-2.32] for >5 years). However, we did not observe any statistically significant increased risk for arrhythmias, heart failure, ischemic heart disease, thromboembolic disease, or cerebrovascular disease ( Table 2 ). Furthermore, long-term use of methylphenidate (compared with no use) was associated with an increased risk of CVD (AOR, 1.20 [95% CI, 1.10-1.31] for 3 to ≤5 years; AOR, 1.19 [95% CI, 1.08-1.31]) for >5 years; eTable 4 in Supplement 1 ). Compared with no use, lisdexamfetamine was also associated with an elevated risk of CVD (AOR, 1.23 [95% CI, 1.05-1.44] for 2 to ≤3 years; AOR, 1.17 [95% CI, 0.98-1.40] for >3 years), while the AOR for atomoxetine use was significant only for the first year of use (1.07 [95% CI 1.01-1.13]; eTable 4 in Supplement 1 ).
In sensitivity analyses, we observed a similar pattern of estimates when the analysis was restricted to ever users of ADHD medications. Significantly increased risk of CVD was found when comparing ADHD medication use for 1 year or less with use for 3 to 5 or less years (AOR, 1.28 (95% CI, 1.18-1.38) or for use for more than 5 years (AOR, 1.24 [95% CI, 1.13-1.36]) (eTable 5 in Supplement 1 ). When assessing ADHD medication use across the entire follow-up period, and compared with no use, the pattern of estimates was similar to the main analysis (3 to ≤5 years: AOR, 1.28 [95% CI, 1.18-1.39]; >5 years: AOR, 1.25 [95% CI, 1.14-1.37]) (eTable 5 in Supplement 1 ). The analysis that included cardiovascular death as a combined outcome also had results similar to the main analysis. Moreover, when adjusting for propensity scores of ADHD medication use, the findings remained consistent (eTable 5 in Supplement 1 ).
This large, nested case-control study found an increased risk of incident CVD associated with long-term ADHD medication use, and the risk increased with increasing duration of ADHD medication use. This association was statistically significant both for children and youth and for adults, as well as for females and males. The primary contributors to the association between long-term ADHD medication use and CVD risk was an increased risk of hypertension and arterial disease. Increased risk was also associated with stimulant medication use.
We found individuals with long-term ADHD medication use had an increased risk of incident CVD in a dose-response manner in the first 3 years of cumulative ADHD medication use. To our knowledge, few previous studies have investigated the association between long-term ADHD medication use and the risk of CVD with follow-up of more than 2 years. 13 The only 2 prior studies with long-term follow-up (median, 9.5 and 7.9 years 30 , 31 ) found an average 2-fold and 3-fold increased risk of CVD with ADHD medication use compared with nonuse during the study period, yet 1 of the studies 30 included only children, and participants in the other study 31 were not the general population of individuals with ADHD (including those with ADHD and long QT syndrome). Furthermore, both studies were subject to prevalent user bias. Results from the current study suggest that the CVD risk associated with ADHD medication use (23% increased risk for >5 years of ADHD medication use compared with nonuse) is lower than previously reported. 30 , 31 Furthermore, we observed that the increased risk stabilized after the first several years of medication use and persisted throughout the 14-year follow-up period.
The association between ADHD medication use and CVD was significant for hypertension and arterial disease, while no significant association was observed with other types of cardiovascular events. To our knowledge, only 1 previous study 12 has examined the association between ADHD medication use and clinically diagnosed hypertension, and it found an increased risk, although the increase was not statistically significant. Furthermore, increased blood pressure associated with ADHD medication use has been well documented. 7 , 9 One study 32 found that blood pressure was mainly elevated during the daytime, suggesting that the cardiovascular system may recover at night. However, the cross-sectional nature of that study cannot preclude a long-term risk of clinically diagnosed hypertension associated with ADHD medication use. We also identified an increased risk for arterial disease. To date, no previous study has explored the association between ADHD medication use and arterial disease. A few studies have reported that ADHD medication may be associated with changes in serum lipid profiles, but the results were not consistent. 33 , 34 Further research is needed on the potential implications of ADHD medications for individuals’ lipid profiles. We did not observe any association between ADHD medication use and the risk of arrhythmias. A recent systematic review of observational studies of ADHD medication use reported an elevated risk of arrhythmias, but the finding was not statistically significant. 13 A review of RCTs also found that the use of stimulants was associated with an average increase in heart rate of 5.7 beats/min, 9 but no evidence of prolonged QT interval or tachycardia was found based on electrocardiograms. 7 Additionally, it is worth noting that some individuals receiving ADHD medications might be prescribed antiarrhythmic β-blockers to alleviate palpitation symptoms, thus potentially attenuating an association between ADHD medications and arrhythmias. Nevertheless, the absence of an association between ADHD medication use and clinically diagnosed arrhythmias in the present study does not rule out an increased risk for mild arrhythmias or subclinical symptoms, as palpitations and sinus tachycardia are not routinely coded as arrhythmia diagnoses. Further research is necessary to replicate our findings.
Regarding types of ADHD medication, findings of the present study suggest that increasing cumulative durations of methylphenidate and lisdexamfetamine use were associated with incident CVD, while the associations for atomoxetine were statistically significant only for the first year of use. Previous RCTs have reported increased blood pressure and heart rate with methylphenidate, lisdexamfetamine, and atomoxetine, 5 , 35 , 36 but the mechanisms behind these adverse effects are still a topic of debate; there might be differences in cardiovascular adverse effects in stimulants vs nonstimulants. 37
We found that the association between cumulative duration of ADHD medication use and CVD was similar in females and males. Previous investigations exploring sex-specific association found higher point estimates in females, although the differences were not statistically significant. 13 Research has indicated that females diagnosed with ADHD may demonstrate different comorbidity patterns and potentially have different responses to stimulant medications compared with males. 38 - 40 Therefore, additional studies are needed to explore and better understand the potential sex-specific differences in cardiovascular responses to ADHD medications.
A strength of this study is that data on ADHD medication prescriptions and CVD diagnoses were recorded prospectively, so the results were not affected by recall bias. The findings should, however, be interpreted in the context of several limitations. First, our approach for identification of patients with CVD was based on recorded diagnoses and there could be under ascertainment of cardiovascular diagnoses in the registers used. This means that some controls may have had undiagnosed CVD that did not yet require medical care, which would tend to underestimate associations between ADHD medication use and CVD. Second, exposure misclassification may have occurred if patients did not take their medication as prescribed. This misclassification, if nondifferential, would tend to reduce ORs such that the estimates we observed were conservative. Third, while we accounted for a wide range of potential confounding variables, considering the observational nature of the study and the possibility of residual confounding, we could not prove causality. It is possible that the association observed might have been affected by time-varying confounders. For example, other psychotropic medications and lifestyle factors could have affected both ADHD medication use and the occurrence of cardiovascular events. 41 , 42 Confounding by ADHD severity is also a potential factor to consider, as individuals with more severe ADHD symptoms may have more comorbidities and a less healthy lifestyle, which could affect the risk of CVD. Fourth, the study did not examine the risk of CVD among individuals with preexisting CVD. Individuals with preexisting CVD represent a distinct clinical group that requires careful monitoring; thus, evaluating the risk among them necessitates a different study design that carefully considers the potential impact of prior knowledge and periodic monitoring. Finally, the results by type of ADHD medication and type of CVD need to be replicated by studies with larger sample sizes.
The results of this population-based case-control study with a longitudinal follow-up of 14 years suggested that long-term use of ADHD medication was associated with an increased risk of CVD, especially hypertension and arterial disease, and the risk was higher for stimulant medications. These findings highlight the importance of carefully weighing potential benefits and risks when making treatment decisions on long-term ADHD medication use. Clinicians should be vigilant in monitoring patients, particularly among those receiving higher doses, and consistently assess signs and symptoms of CVD throughout the course of treatment. Monitoring becomes even more crucial considering the increasing number of individuals engaging in long-term use of ADHD medication.
Accepted for Publication: August 29, 2023.
Published Online: November 22, 2023. doi:10.1001/jamapsychiatry.2023.4294
Open Access: This is an open access article distributed under the terms of the CC-BY License . © 2023 Zhang L et al. JAMA Psychiatry .
Corresponding Authors: Zheng Chang, PhD ( [email protected] ) and Le Zhang, PhD ( [email protected] ), Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Nobels väg 12A, 171 65 Stockholm, Sweden.
Author Contributions: Dr Zhang and Prof Chang had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: Zhang, Johnell, Larsson, Chang.
Acquisition, analysis, or interpretation of data: Zhang, Li, Andell, Garcia-Argibay, Quinn, D'Onofrio, Brikell, Kuja-Halkola, Lichtenstein, Johnell, Chang.
Drafting of the manuscript: Zhang.
Critical review of the manuscript for important intellectual content: All authors.
Statistical analysis: Zhang, Li.
Obtained funding: Larsson, Chang.
Administrative, technical, or material support: Garcia-Argibay, D'Onofrio, Kuja-Halkola, Lichtenstein, Chang.
Supervision: Andell, Lichtenstein, Johnell, Larsson, Chang.
Conflict of Interest Disclosures: Dr Larsson reported receiving grants from Takeda Pharmaceuticals and personal fees from Takeda Pharmaceuticals, Evolan, and Medici Medical Ltd outside the submitted work. No other disclosures were reported.
Funding/Support: This study was supported by grants from the Swedish Research Council for Health, Working Life, and Welfare (2019-01172 and 2022-01111) (Dr Chang) and the European Union’s Horizon 2020 research and innovation program under grant agreement 965381 (Dr Larsson).
Role of the Funder/Sponsor: The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Data Sharing Statement: See Supplement 2 .
- Register for email alerts with links to free full-text articles
- Access PDFs of free articles
- Manage your interests
- Save searches and receive search alerts
COMMENTS
1. Introduction. Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder (NDD) presenting with inattention, hyperactivity, and impulsivity. It can be classified in three subtypes, depending on the intensity of the symptoms: predominantly inattentive, predominantly hyperactive-impulsive, and combined [ 1, 2 ].
ADHD increases the risk of substance misuse disorders 1.5-fold (2.4-fold for smoking) and problematic media use 9.3-fold in adolescence 55 56 and increases the risk of becoming obese 1.23-fold for adolescent girls. 57 58 59 It is also associated with different forms of dysregulated eating in children and adolescents.
Introduction. With an estimated worldwide prevalence around 5-7 ... JAACAP was the journal with the highest number of citations of papers on ADHD, followed by the American Journal of Psychiatry ... We hope that the present scientometric study will increase awareness of ADHD research trend over time and its future directions among clinicians ...
Attention-deficit hyperactivity disorder (ADHD), like other psychiatric disorders, represents an evolving construct that has been refined and developed over the past several decades in response to research into its clinical nature and structure. The clinical presentation and course of the disorder have been extensively characterised. Efficacious medication-based treatments are available and ...
Twin and family studies have found that the same genetic factors influence both the disorder of ADHD and lower levels of ADHD symptoms in the general population 61,64, and that shared genetic ...
While much research has reported on the benefits and adverse effects of different interventions for ADHD, these individual research reports and the reviews, meta-analyses and guidelines summarizing their findings are sometimes inconsistent and difficult to interpret. ... Introduction. Attention deficit ... The purpose of this paper is to ...
1. Introduction. Nearly two decades ago, an international team of scientists published the first International Consensus Statement on attention-deficit hyperactivity disorder (ADHD) (Barkley, 2002).They sought to present the wealth of scientific data attesting to the validity of ADHD as a mental disorder and to correct misconceptions about the disorder that stigmatized affected people, reduced ...
Introduction. The combination of psychological theory and interpretation of research have been highlighted as critical influencers guiding decision-making for clinical treatment design and development for Attention Deficit Hyperactivity Disorder (ADHD) [1, 2].ADHD is a neurodevelopmental disorder of self-regulation with symptoms negatively affecting daily functioning at work and at home, with ...
The introduction of machine learning approaches, ... Probably, the most crucial area of future treatment research in ADHD will be to gain insight into the long-term positive and negative effects of treatments, using randomised trials with withdrawn designs, as well as additional population-based studies with self-controlled methodologies and ...
Affiliations 1 Academic Unit of Psychology, Center for Innovation in Mental Health, University of Southampton, Southampton, UK.; 2 Clinical and Experimental Sciences (CNS and Psychiatry), Faculty of Medicine, University of Southampton, Southampton, UK.; 3 Solent NHS Trust, Southampton, UK.; 4 New York University Child Study Center, New York City, New York, USA.
A robust body of evidence suggests that children with ADHD are at increased risk for other co-occurring conditions, including depression, anxiety, and substance use disorders (Asherson et al., 2016; Costa Dias et al., 2013).Additionally, ADHD is associated with lower educational or occupational achievement, reduced social functioning (Costa Dias et al., 2013; Franke et al., 2018), and ...
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder in which patients present inattention, hyperactivity, and impulsivity. The etiology of this condition is diverse, including environmental factors and the presence of variants of some genes. However, a great diversity exists among patients regarding the presence of these ADHD-associated factors. Moreover, there are ...
ADHD is a chronic disorder with identified genetic underpinnings, neurochemical and structural brain abnormalities, and common symptom presentations. ADHD related dysfunction includes occupational, academic, family, social, emotional and interpersonal functional impairments. There is a need for a clear and concise approach to a complex disorder ...
Introduction. The combination of psychological theory and interpretation of research have been highlighted as critical influencers guiding decision-making for clinical treatment design and development for Attention Deficit Hyperactivity Disorder (ADHD) [1, 2].ADHD is a neurodevelopmental disorder of self-regulation with symptoms negatively affecting daily functioning at work and at home, with ...
Systematic Search for and Retrieval of Research Reports. The inclusion criteria (see Table 1) were defined as studies on children's and adolescents' experiences and understanding of their ADHD, whereby qualitative methods were used for collecting and analysing data.The children and adolescents, diagnosed with ADHD, had to be under 19 years of age at the time the study was conducted.
Children with Attention Deficit Hyperactivity Disorder (ADHD) are more at risk for academic underachievement compared to their typically developing peers. Understanding their greatest strengths and challenges at school, and how these can be supported, is vital in order to develop focused classroom interventions. Ten primary school pupils with ADHD (aged 6-11 years) and their teachers (N = 6 ...
Introduction: Attention Deficit Hyperactive Disorder (ADHD) has been described by the American Psychiatric Association (APA, 1994) as age-inappropriate inattention, impulsivity, and hyperactivity.
The assessment of impairment in every given ADHD evaluation can be seen as a gatekeeper that protects against over-diagnosis. In contrast, the presence of ADHD symptoms without the experience of functional impairment does not fulfill the criteria of a mental disorder (Spitzer et al., 2018) and represents a serious threat for diagnostic validity and common reason for false positives (Sibley, 2021).
Conclusion This research highlights the experiences of adults with ADHD. It is important for practitioners to be aware of the perceived positive and negative effects of the disorder, and how it ...
Research to date has shown the following: ADHD is a biological disorder, not just "bad behavior." In a child with ADHD, the brain's ability to properly use important chemical messengers (neurotransmitters) is impaired. A lower level of activity in the parts of the brain that control attention and activity level may be associated with ADHD.
Attention deficit/hyperactivity disorder (ADHD) is among the most common neurobehavioral disorders presenting for treatment in children and adolescents. ADHD is often chronic with prominent symptoms and impairment spanning into adulthood. ADHD is often associated with co-occurring disorders including disruptive, mood, anxiety, and substance abuse.
Statement of the Problem. The purpose of this study is to further explore, through the published literature, the social effects that ADHD has on a student's social skill development and how a. student's lack of social competence effects relationships with their peers. By exploring.
ADHD Research Paper. This sample ADHD research paper features: 8200 words (approx. 27 pages), an outline, and a bibliography with 14 sources. Browse other research paper examples for more inspiration. If you need a thorough research paper written according to all the academic standards, you can always turn to our experienced writers for help.
Racial/ethnic disparities in ADHD diagnosis may contribute to the relatively low diversity of study participants , and such disparities are further reason to expand research focused on non-White individuals with ADHD. Most studies focused on young or middle-aged adults and most participants were male; more research is needed on how ADHD may ...
Very happy to research gaps being filled on long-term CVD risk of stimulant medication for ADHD and this paper adds a lot here. After review of the paper and supplemental materials, I am wondering if amphetamines other than lisdexamphetamine showed similar risk - I don't see that table, maybe sample sizes were too small for those drugs.