- Open access
- Published: 10 June 2024

New advances in the diagnosis and treatment of autism spectrum disorders
- Lei Qin 1 ,
- Haijiao Wang 2 ,
- Wenjing Ning 1 ,
- Mengmeng Cui 1 &
- Qian Wang 3
European Journal of Medical Research volume 29 , Article number: 322 ( 2024 ) Cite this article
2869 Accesses
Metrics details
Autism spectrum disorders (ASD) are a group of neurodevelopmental disorders that affect individuals' social interactions, communication skills, and behavioral patterns, with significant individual differences and complex etiology. This article reviews the definition and characteristics of ASD, epidemiological profile, early research and diagnostic history, etiological studies, advances in diagnostic methods, therapeutic approaches and intervention strategies, social and educational integration, and future research directions. The highly heritable nature of ASD, the role of environmental factors, genetic–environmental interactions, and the need for individualized, integrated, and technology-driven treatment strategies are emphasized. Also discussed is the interaction of social policy with ASD research and the outlook for future research and treatment, including the promise of precision medicine and emerging biotechnology applications. The paper points out that despite the remarkable progress that has been made, there are still many challenges to the comprehensive understanding and effective treatment of ASD, and interdisciplinary and cross-cultural research and global collaboration are needed to further deepen the understanding of ASD and improve the quality of life of patients.
Autism spectrum disorders (ASD) are a broad group of neurodevelopmental disorders that affect an individual's social interactions, communication skills, and behavioral patterns [ 1 , 2 ]. The characteristics of ASD vary significantly between individuals, from mild social impairments to severe communication and behavioral problems, a diversity that reflects the use of the term “spectrum” [ 3 ]. Although the exact causes of ASD are not fully understood, research suggests that both genetic and environmental factors play a key role in its development [ 4 ].
Characteristics of ASD
Difficulties in social interaction.
Individuals with ASD often exhibit significant difficulties in social interactions. These difficulties may include difficulty understanding the feelings and intentions of others, maintaining eye contact and facial expressions, and adapting to social norms and expectations. Individuals with ASD may experience challenges in establishing and maintaining friendships, they may not understand the two-way nature of social interactions, or they may feel uncomfortable sharing interests and activities [ 5 ].
Communication disorders
Communication deficits are another core feature of ASD. This may manifest itself in delays in language development, including delays in uttering first words or simple sentences. Some individuals with ASD may not use language to communicate at all. Even among individuals with ASD who have normal language skills, they may have difficulty using language in conversations to communicate thoughts, feelings, or needs. In addition, nonverbal communication, such as the understanding and use of body language and facial expressions, may also be affected [ 6 ].
Repetitive behaviors and interests
Individuals with ASD often display restricted, repetitive patterns of behavior and interests. These may include a strong fixation on specific topics or activities, repetitive body movements (e.g., rocking, clapping), and an overreliance on daily routines. These repetitive behaviors are sometimes seen as a way of self-soothing or as an attempt to control an environment that otherwise feels unpredictable and overwhelming to them [ 7 ].
Sensory sensitivity
Many individuals with ASD have abnormalities in sensory processing and may have very strong or delayed responses to sound, light, touch, taste or odor. For example, some individuals with ASD may find background noises in their everyday environment unusually harsh, or they may not notice pain or other bodily sensations [ 8 ].
Epidemiologic profile of ASD
According to the World Health Organization (WHO), the average prevalence of ASD among children globally is approximately 1% [ 9 ]. However, this figure varies significantly between regions and countries. For example, the Centers for Disease Control and Prevention (CDC) reports that the prevalence of ASD among 8-year-olds in the U.S. is 1 to 54. ASD is significantly more prevalent in males than females, at a ratio of approximately 4:1 [ 10 ]. This gender difference may reflect differences in genetic susceptibility and/or gender bias in the diagnostic process. Early diagnosis is key to improving developmental outcomes for children with ASD. Despite this, many children are not diagnosed by age 3. The CDC reports that most children are first evaluated for ASD by age 4, but diagnosis may occur later. Research suggests that ASD is highly heritable, but multiple genetic variants are associated with disease risk and environmental factors also play a role [ 11 ]. For example, there is an increased risk of ASD in preterm and low birth weight infants. Socioeconomic factors influence ASD diagnosis and treatment access. Families of lower socioeconomic status may face greater challenges, including barriers to accessing early intervention services, etc. ASD is a global public health problem, and its incidence, time to diagnosis, and treatment access are influenced by multiple factors [ 12 ]. Ongoing epidemiologic research and the advancement of a deeper understanding of ASD are critical to the development of effective prevention, diagnosis, and interventions.
Historical background
Early history of research and diagnosis of asd.
The concept of ASD was first clearly defined in the 1940s, when a group of children exhibiting extreme self-isolation and lack of responsiveness to the environment was first described by American psychiatrist Leo Kanner [ 13 ]. Almost simultaneously, Austrian child psychologist Hans Asperger described a similar but higher level of functioning in a condition that came to be known as Asperger’s syndrome [ 14 ]. These two independent studies laid the foundation for the modern understanding of ASD. For the first few decades, ASD was considered extremely rare and was often confused with schizophrenia. Due to a lack of in-depth understanding of ASD, early diagnostic criteria were unclear and treatment was largely limited to behavioral interventions and psychotherapy. Over time, researchers began to pay more attention to the genetic and neurobiological underpinnings of ASD, thus contributing to a more comprehensive understanding of this complex condition. Since the 1990s, the diagnosis of ASD has risen significantly, as diagnostic criteria have continued to be refined and public awareness has increased. This period has also witnessed an increased awareness of the importance of early diagnosis and intervention for ASD, which has led to significant improvements in the prognosis and quality of life for many children and adults with ASD [ 15 ].
Evolution of research paradigms
The research paradigm for ASD has undergone a remarkable evolution since the mid-twentieth century, a process that reflects a deepening of the understanding of ASD as well as advances in scientific research methods [ 16 ]. In the early stages, ASD research focused on behavioral observations and psychoanalysis, when ASD was often mistaken for an emotional disorder due to an indifferent mother. During this period, understanding of ASD was relatively limited and treatments focused primarily on psychotherapy and behavior modification. Into the second half of the twentieth century, with advances in genetics and neuroscience, researchers began to explore the biological basis of ASD. This marked a shift from a psychosocial to a biomedical model, and the focus of research gradually shifted to genetic factors and abnormalities in brain structure and function. Through a large number of family and twin studies, scientists found that ASD has a high genetic predisposition, while neuroimaging studies revealed the specificity of brain development in ASD patients. In the twenty-first century, with the application of bioinformatics and high-throughput gene sequencing technology, the study of ASD has entered a new stage [ 17 ]. Researchers have not only been able to identify specific genetic variants associated with ASD, but have also begun to explore the interaction between environmental factors and genetic susceptibility. In addition, the adoption of interdisciplinary research approaches, such as combining neuroscience, genetics, psychology, and computational modeling, has provided new perspectives for understanding the complexity of ASD.
Recently, the concepts of precision medicine and personalized treatment strategies have been introduced to the study of ASD, aiming to develop customized intervention programs based on each patient’s genetic background and symptom profile. With advances in technology and improved methods of data analysis, future research on ASD is expected to reveal more knowledge about its pathomechanisms and provide more effective support and treatment for patients with ASD.
Etiologic studies
Genetic factors, monogenic genetic cases.
The etiology of ASD is multifactorial, involving a complex interaction of genetic and environmental factors. Although most cases of ASD are thought to be the result of polygenic interactions, there are some cases that are directly associated with variations in a single gene, and these are referred to as monogenic genetic cases. Monogenic genetic cases provide an important window into understanding the genetic basis of ASD, although they represent a relatively small proportion of all ASD cases [ 18 ]. A number of specific genetic syndromes, such as fragile X syndrome, tuberous sclerosis, 15q11-q13 duplication syndrome, and Rett syndrome, have been found to be associated with a higher risk of ASD. These conditions, often caused by mutations or abnormalities in a single gene, can lead to significant differences in brain development and function, thereby increasing the probability of an ASD phenotype. Fragile X syndrome is one of the most common forms of inherited intellectual disability and the single-gene disorder known to be most strongly associated with ASD. It is caused by a repeat expansion on the FMR1 gene [ 19 ]. Tuberous sclerosis (TSC) is an inherited disorder that affects multiple systems and is caused by mutations in the TSC1 or TSC2 genes, and the prevalence of ASD is higher in patients with TSC. 15q11-q13 duplication syndrome (Dupuy 15q syndrome) involves a region of chromosome 15, the duplication of which is associated with an increased risk of ASD [ 20 ]. Rett syndrome, which predominantly affects females, is caused by mutations in the MECP2 gene, and patients often exhibit some of the features of ASD, such as impaired social interactions [ 21 ]. The association of these classical candidate genes with ASD is summarized in Table 1 .
The discovery of these monogenic genetic cases is not only crucial for understanding the genetic mechanisms of ASD, but also potentially valuable for the development of interventional and therapeutic strategies targeting specific genetic variants. However, even in these cases, the expression of the genetic variants showed a degree of heterogeneity, suggesting that the diversity of phenotypic features and clinical manifestations, even in monogenic genetic cases, may be influenced by other genetic and environmental factors. Therefore, an in-depth study of these conditions will not only improve our understanding of the genetic basis of ASD, but also provide clues for the development of more personalized therapeutic strategies.
Multigene interactions
The development of ASD is widely recognized as a result of the interaction of genetic and environmental factors, with polygenic interactions occupying a central position in the genetic background of the disease. Unlike monogenic cases, polygenic interactions involve variants or polymorphisms in multiple genes that together increase the risk of ASD. These genetic variants may contribute a smaller effect in each individual, but when acting together they can significantly increase the probability of ASD development [ 30 ]. Current research suggests that no single gene can explain all cases of ASD. Instead, hundreds of genetic loci have been identified that are associated with an increased risk of ASD. These genes are often involved in key processes such as brain development, neuronal signaling, and intercellular communication, suggesting that ASD involves extensive regulation of brain function and structure. The complexity of multigene interactions means that genetic studies of ASD require large-scale genomic data and sophisticated statistical methods to reveal those genomic variants that increase risk.
Meta-analyses of large-sample genome-wide association studies (GWAS) have identified several consistently replicated ASD risk gene loci, such as those in the chromosomal regions 3p21, 5p14, 7q35, and 20p12. These loci contain genes like CNTN4, CNTNAP2, and NRXN1, which play crucial roles in neurodevelopment and synaptic function, particularly in processes such as synaptic adhesion and neurotransmission. These findings provide a more robust understanding of the genetic architecture of ASD and highlight the importance of integrating genetic findings with functional studies to advance our understanding of the disorder. They also have implications for future research, such as the development of personalized diagnostic and therapeutic strategies based on an individual's genetic profile. Through genome-wide association studies (GWAS) and other genomic approaches, scientists are gradually unraveling the genetic landscape of this complex disease. Understanding the impact of multiple gene interactions on ASD not only helps us understand its genetic basis, but also opens up the possibility of developing personalized treatment and intervention strategies [ 31 ].
Environmental factors
Maternal exposure.
Exposure during pregnancy refers to a mother’s exposure to specific environmental factors or substances during fetal development, which may increase the child's risk of developing ASD in the future. These exposures include certain prescription medications (e.g., anti-seizure medications and opioids), environmental pollutants (e.g., heavy metals and air pollutants), infections (e.g., rubella and influenza viruses), and poor nutrition or deficiencies in specific nutrients (e.g., folic acid). These factors may increase the risk of ASD by affecting fetal brain development and the maturation process of the nervous system. Understanding the effects of exposure during pregnancy can help to take preventive measures to reduce the incidence of ASDs [ 32 ].
Effects of early developmental stages
The early developmental stages of ASD are influenced by a variety of factors that include genetic predisposition, environmental exposures, and early life experiences. During a child's early development, the brain experiences rapid growth and the formation of neural networks. Any disruption during this critical period may interfere with the proper development of brain structure and function, thereby increasing the risk of ASD. For example, very early lack of social interaction, delayed language development or abnormal sensory processing may be early signs of ASD. These developmental abnormalities reflect difficulties in the brain’s nervous system in processing information, making connections and adapting to environmental changes. Early identification and intervention are essential to promote optimal development in children with ASD [ 33 ].
Genetic–environmental interactions
The genetic–environmental interactions are summarized in Fig. 1 . ASD develops as a result of the interaction between genetic and environmental factors, and this interaction reflects the complexity of the combination of genetic background and external environmental factors that influence ASD risk. Specifically, certain genetic susceptibilities may be activated in response to environmental triggers, leading to the development of ASD. For example, genetic variants may make individuals more sensitive to certain environmental exposures (e.g., substance use during pregnancy, environmental pollutants, or maternal nutritional status), which together may increase the risk of ASD by acting on key brain developmental stages [ 34 ]. This complex genetic–environmental interaction underscores the need to understand multifactorial etiological models of ASD and the importance of developing personalized intervention strategies.

Advances in diagnostic methods
Traditional diagnostic methods.
Traditional diagnostic methods for ASD rely heavily on detailed assessments of behavior and developmental history. These assessments are usually conducted by specialized health care providers such as pediatricians, neuropsychologists, or psychiatrists. The diagnostic process encompasses direct observation of the child as well as in-depth interviews with parents or caregivers to gather information about the child's social interactions, communication skills, and behavioral patterns [ 35 ]. Diagnostic tools include, but are not limited to, the Childhood Autism Rating Scale (CARS), the Autism Diagnostic Observation Scale (ADOS), and the Autism Diagnostic Interview-Revised (ADI-R). These tools are designed to identify core symptoms of ASD, such as social communication deficits and repetitive behaviors or interests. In addition, the doctor may perform a series of developmental or cognitive assessments to rule out other conditions that may explain the child’s behavior, such as language disorders or other neurodevelopmental disorders [ 36 ]. While these traditional diagnostic methods are highly effective in recognizing ASD, they rely on subjective assessments and the experience of the professional, and therefore may have some degree of variability. In recent years, with a deeper understanding of ASDs, new diagnostic techniques and methods are being developed and adopted to improve diagnostic accuracy and efficiency.
Latest diagnostic techniques and tools
Genetic testing.
Genetic testing for ASD is a method of identifying risks associated with ASD by analyzing genetic variants in an individual's DNA. This testing looks for specific genetic variants that have been linked by scientific research to the development of ASD. Although the genetic background of ASD is extremely complex, involving multiple genes and the interaction of genes with environmental factors, variants in specific genes have been identified as having a significant impact on ASD risk [ 37 ]. For example, variants in the SHANK3 gene are associated with Phelan–McDermid syndrome, and patients with this syndrome often exhibit ASD features. Variants in the FMR1 gene are responsible for fragile X syndrome, which is the most common single-gene cause of ASD known to be associated with ASD. Mutations in the MECP2 gene have been associated with Rett syndrome, and patients with Rett syndrome often exhibit ASD condition. In addition, variants in the NRXN1 and NLGN3/4 genes have been found to increase the risk of ASD [ 38 ]. Genetic testing can help provide more precise diagnostic information, and in those cases of ASD where the cause is unknown, it may even reveal the underlying genetic cause. This will not only help to understand the genetic mechanisms of ASD, but also provide more targeted intervention and support strategies for patients and families.
Neuroimaging
Neuroimaging techniques in the study of ASD provide a non-invasive way to explore changes in brain structure and function, helping scientists better understand the biological basis of ASD. These techniques include functional magnetic resonance imaging (fMRI), structural magnetic resonance imaging (sMRI), diffusion tensor imaging (DTI), and positron emission tomography (PET). Through these neuroimaging techniques, researchers are able to observe structural and functional differences in specific regions and networks of the brain in individuals with ASD [ 39 ]. For example, fMRI can reveal patterns of brain activity when performing specific tasks, helping to understand the impairments in social, language, and cognitive functioning in individuals with ASD. dTI focuses on the microstructure of the brain’s white matter, revealing the connections of bundles of nerve fibers, which can help to study neural connectivity issues in ASD. PET scans, on the other hand, are able to assess the activity of specific chemicals in the brain, providing clues to study the neurochemical basis of ASD [ 40 ]. With these advanced neuroimaging techniques, researchers will not only be able to delve deeper into the neurodevelopmental abnormalities of ASD, but also identify possible novel therapeutic targets that can provide a scientific basis for developing more effective interventions. However, while these techniques provide valuable perspectives in understanding ASD, a complete understanding of the complexity of the brain remains a challenge for future research.
Early screening methods
Recently, the field of early screening for ASD has witnessed the application of a number of innovative techniques designed to improve the accuracy and convenience of screening. One notable new approach is the use of artificial intelligence (AI) and machine learning techniques to analyze children's behavioral videos and biomarkers. By training algorithms to recognize specific behavioral patterns and physiological signals associated with ASD, these technologies can help physicians and researchers identify potential ASD symptoms earlier [ 41 ]. Another area of innovation is eye-tracking technology, which assesses children’s social and cognitive development by analyzing their eye movement patterns when viewing pictures or videos. Studies have shown that the eye movement patterns of children with ASD while viewing social scenes differ from those of typically developing children, providing a non-invasive window for early screening [ 42 ]. The application of these state-of-the-art technologies not only improves the efficiency and accessibility of early screening, but also provides new perspectives for understanding the complexity and individual differences in ASD [ 43 ]. Although these approaches are still in the research and development stage, they demonstrate the great potential of utilizing technological advances to improve the process of ASD screening and diagnosis. With further validation and refinement of these techniques, it is expected that they will make a significant contribution to the early identification and intervention of ASD in the future.
Treatment approaches and intervention strategies
Behavioral and educational interventions, applied behavior analysis (aba).
Applied behavior analysis (ABA) is an intervention approach based on the principles of behavioral psychology that is widely used in the treatment of children with autism spectrum disorders (ASD). ABA works to understand and improve specific behaviors, particularly to enhance social, communication, academic skills, and daily living skills, while reducing maladaptive behaviors. It helps individuals learn new skills and behaviors by systematically applying reinforcement strategies that encourage and reward desired behaviors [ 44 ]. ABA therapy is highly individualized and customized to each child’s specific needs and abilities. Treatment planning begins with a detailed behavioral assessment to identify target behaviors and intervention strategies. Learned behaviors are then reinforced and cemented through one-on-one teaching sessions using positive reinforcement. ABA also emphasizes the importance of data, which is collected and analyzed on an ongoing basis by the therapist to monitor progress and adjust the treatment plan as necessary [ 45 ]. Research has shown that ABA is an effective way to improve social interactions, communication skills, and learning in children with ASD. Through early and consistent intervention, ABA can significantly improve the independence and overall quality of life of children with ASD. Although ABA treatment requires a commitment of time and resources, the long-term benefits it brings to children with ASD and their families are immeasurable.
Social skills training
Social skills training (SST) for children with autism spectrum disorders (ASD) is an intervention designed to improve their ability to interact socially in everyday life. This training focuses on teaching children with ASD the ability to understand social cues, establish effective communication skills, and develop friendships. Through SST, children learn how to recognize and interpret other people's facial expressions, body language, and social etiquette, which are essential for building positive relationships [ 46 ]. Social skills training typically includes a series of structured instructional activities such as role-playing, social stories, interactive group exercises, and peer modeling. These activities are designed to provide practice in real-world social situations in a supportive and interactive manner, helping children with ASD learn and practice new skills in a safe environment [ 47 ]. In addition, SST can include teaching emotion management and conflict resolution skills to help children with ASD better understand and express their emotions and cope with challenges in social interactions. Through regular and consistent practice, children with ASD can improve their self-confidence, increase their social engagement, and ultimately improve their social competence and quality of life. SST has been shown to be significantly effective in enhancing social adjustment and interpersonal interactions in children with ASD [ 48 ].
Medical treatment
While there is no cure for ASD, certain medications can be used to manage specific symptoms associated with ASD, such as behavioral problems, attention deficits, anxiety, and mood swings that are common in individuals with autism. Medication is often used as part of a comprehensive intervention program designed to improve the quality of life and daily functioning of the patient [ 49 ]. Medications commonly used for ASD symptom management include antipsychotics, antidepressants, stimulants, and anxiolytics. For example, two antipsychotics, risperidone and aripiprazole, have been approved by the FDA for the treatment of stereotypic and aggressive behavior in children and adolescents with ASD. In addition, selective serotonin reuptake inhibitors (SSRIs) may be helpful in managing anxiety and depressive symptoms in individuals with ASD.
Importantly, medication needs to be closely monitored by a physician to ensure the effectiveness and safety of the medications, as they may have side effects. We have summarized the research evidence on the efficacy and safety of commonly used medications in ASD, including antipsychotics for treating irritability and aggression, antidepressants for co-occurring anxiety and depression, and other medications such as stimulants and melatonin. While these medications can be helpful in managing specific symptoms, they also carry potential side effects and risks, such as weight gain, metabolic disturbances, and behavioral activation. Therefore, a thorough diagnostic evaluation, individualized treatment planning, close monitoring, and regular follow-up are essential when considering pharmacotherapy for individuals with ASD. The decision to medicate should be based on an individualized assessment that takes into account the patient’s specific needs, the severity of symptoms, and possible side effects. At the same time, pharmacological treatments are often used in combination with non-pharmacological treatments such as behavioral interventions and educational support to achieve optimal therapeutic outcomes [ 50 ].
Biofeedback and neuromodulation
Biofeedback and neuromodulation are innovative approaches that have been explored in recent years in the treatment of ASD, aiming to reduce ASD symptoms by improving brain function. Biofeedback techniques enable individuals to learn how to control physiological processes that are not normally under conscious control, such as heart rate, muscle tension, and brainwave activity. Through real-time feedback, patients can learn how to regulate their physiology, resulting in improved concentration, reduced anxiety, and improved emotional regulation. Neuromodulation, specifically transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS), affects neural activity in the brain through external stimulation. tMS utilizes a magnetic field to affect neuronal activity in specific areas of the brain, while tDCS modulates neuronal excitability by applying a weak electrical current. These methods have been studied for improving social communication skills and reducing stereotypical behaviors in people with ASD [ 51 ].
Biofeedback helps individuals develop self-regulation skills by providing real-time feedback on physiological states, while neuromodulation techniques like TMS and tDCS modulate cortical excitability and neural plasticity in aberrant circuits implicated in ASD. Current research suggests potential benefits of these techniques in improving emotional regulation, social functioning, and cognitive performance, but mixed results highlight the need for larger, well-controlled trials to validate efficacy, safety, and optimal protocols. Despite challenges, these techniques show promise as adjunctive therapies in the comprehensive management of ASD, warranting further research to guide their translation into clinical practice. Although biofeedback and neuromodulation show potential in the treatment of ASD, research on these techniques is currently in its infancy. More clinical trials and studies are needed to evaluate their effectiveness, safety, and long-term effects and to determine which patients may benefit from these interventions. Nevertheless, as non-pharmacologic treatments, they offer promising complementary options to the comprehensive treatment of ASD.
Emerging intervention approaches
Technology-assisted interventions.
Technology-assisted interventions have become an important development in the field of ASD treatment in recent years, providing new ways for children with ASD to learn and communicate. These interventions utilize computers, tablets, smartphone apps, and virtual reality technology to design a range of interactive learning tools and games designed to improve social skills, communication, and cognitive functioning in children with ASD [ 52 ]. A key advantage of technology-assisted interventions is their ability to provide highly personalized learning experiences. Software and applications can be adapted to a child's specific needs and interests, ensuring that learning content is both engaging and appropriate to the individual's developmental level. In addition, the feedback provided by technology is often immediate and consistent, helping children with ASD to better understand and process information. The use of virtual reality technology, by simulating social situations, provides a safe and controlled environment for children with ASD to practice social interaction and problem-solving skills, which is often difficult to achieve in traditional educational and therapeutic settings [ 53 ]. Although technology-assisted interventions have demonstrated great potential, research on their long-term effects and optimal implementation is still ongoing. To maximize the benefits of these tools, it is often recommended that technology-assisted interventions be used in conjunction with other therapeutic approaches to provide a comprehensive intervention program.
Diet and nutrition interventions
Dietary and nutritional interventions have received increasing attention in the treatment of ASD, based on the observed potential link between nutritional imbalances and ASD symptoms. This intervention approach aims to improve the behavioral performance and overall health of children with ASD by optimizing their diet. Specific strategies include restricting certain foods that may exacerbate symptoms, such as gluten and lactose, as well as increasing intake of foods rich in essential nutrients to support brain development and function [ 54 ]. Several studies support the potential benefits of specific dietary interventions, such as implementing a gluten-free lactose-free (GFCF) diet, which may help improve behavioral and digestive symptoms in some children with ASD. In addition, supplementation with omega-3 fatty acids, vitamins, and minerals (e.g., magnesium and zinc) have been proposed as potentially beneficial strategies to support neurologic health and alleviate ASD-related symptoms [ 55 ]. However, the effectiveness of dietary and nutritional interventions may vary by individual and more scientific research is needed to gain a deeper understanding of their long-term effects on children with ASD. Before implementing any dietary intervention, it is recommended to consult with a physician or nutritional expert to ensure that the individual needs of the child are met and to avoid malnutrition. In combination, dietary and nutritional interventions can be used as part of a comprehensive treatment plan for ASD, complementing traditional behavioral and educational interventions.
Social and educational integration
Educational integration of children with asd.
Educational integration of children with ASD is an inclusive educational practice that seeks to integrate children with ASD into the mainstream educational system to learn and grow with their typically developing peers. This integration model emphasizes individualized learning plans and adaptive teaching strategies to meet the unique needs of children with ASD while promoting their social inclusion and emotional development. Through educational integration, children with ASD are provided with opportunities to interact with other children, which is essential for them to learn social skills, enhance their communication abilities, and improve their ability to adapt to society. To support the successful integration of children with ASD, schools often provide special education services such as speech and language therapy, occupational therapy, and behavioral interventions, which take place in classroom settings to ensure their academic and social progress. Educational inclusion is not only beneficial for children with ASD, but it also helps to foster a sense of inclusion and diversity among their peers. By learning and playing together, all children learn to respect and understand differences, laying the foundation for a more inclusive society. However, effective integrated education requires close collaboration among teachers, parents and professionals, as well as the availability of appropriate resources and support systems [ 56 ].
Social integration and employment of adults with ASD
The social integration and employment of adults with ASD is a current focus of attention in ASD research and social services. For many adults with ASD, social integration challenges include establishing stable relationships, participating in community activities, and finding and keeping a job. Although adults with ASD may have unique skills and interests in specific areas, social communication deficits and fixed patterns of behavior may make it difficult for them in traditional work settings. In recent years, more and more organizations and businesses have begun to recognize the value of diversity and inclusion and are working to create work environments that are better suited for adults with ASD. This includes providing flexible work arrangements, clear communication guidelines, and individualized support measures such as workplace co-worker support and professional career counseling. In addition, social service programs and non-profit organizations offer training and job readiness programs specifically designed for adults with ASD to help them develop necessary vocational skills and social competencies. Through these efforts, adults with ASD will not only be able to find jobs that meet their interests and abilities, but also find a place for themselves in society, enhancing their independence and life satisfaction. However, the realization of this goal requires sustained social awareness-raising and the construction of an ASD-friendly environment [ 57 ].
Future research directions
Application of precision medicine in asd treatment.
The application of precision medicine in the treatment of ASD represents a paradigm of a personalized treatment strategy that aims to tailor the treatment plan to each patient's genetic information, biomarkers, history of environmental exposure, and lifestyle factors. The philosophy behind this approach is that, although ASD is classified as a spectrum, each patient's etiology, symptoms, and their severity are different, and therefore treatment should be highly individualized [ 58 , 59 ]. By fully sequencing a patient's genome, scientists and physicians can identify specific genetic variants that may affect ASD symptoms, allowing them to develop targeted treatments. For example, if a particular ASD patient's symptoms are linked to an abnormality in a specific metabolic pathway, that pathway could be modulated through dietary adjustments, nutritional supplements, or specific medications with a view to improving symptoms. In addition, precision medicine involves the consideration of environmental factors and personal behavior to ensure that treatment options are not only scientifically effective, but also appropriate to the patient's lifestyle. Although precision medicine is still in its early stages in the field of ASD, it offers great potential for delivering more personalized and effective treatment regimens, which are expected to significantly improve the quality of life of people with ASD [ 60 ].
Prospects for emerging biotechnologies
Emerging biotechnologies in the field of ASD, such as gene editing, stem cell therapies, and biomarker development, are opening up new possibilities for treating and understanding ASD. Gene editing technologies, particularly the CRISPR-Cas9 system, provide researchers with the means to precisely modify genetic variants associated with ASD, promising to reveal how specific genetic variants affect brain development and function, thereby providing clues for the development of targeted therapies [ 61 ]. Stem cell therapies utilize a patient's own induced pluripotent stem cells (iPSCs) to study the pathomechanisms of ASD by mimicking the neurodevelopmental process in vitro, as well as exploring potential cellular alternative treatments. In addition, the discovery of biomarkers facilitates early diagnosis and monitoring of disease progression, making personalized treatment possible [ 62 ]. In addition, induced pluripotent stem cell (iPSC)-derived brain organoids from ASD patients have emerged as a powerful tool for studying the neurodevelopmental abnormalities associated with ASD. These 3D, self-organizing models recapitulate key features of human brain development in vitro, allowing researchers to investigate the cellular and molecular mechanisms underlying ASD pathogenesis. By comparing brain organoids derived from ASD patients with those from healthy controls, researchers can identify alterations in neuronal differentiation, migration, and connectivity that may contribute to the development of ASD. Moreover, patient-derived brain organoids provide a personalized platform for drug screening and testing, enabling the identification of targeted therapies that can be tailored to an individual's genetic background. This approach has the potential to revolutionize the development of precision medicine strategies for ASD, by providing a more accurate and relevant model system for investigating disease mechanisms and testing novel therapeutic interventions. As the field continues to advance, iPSC-derived brain organoids are expected to play an increasingly important role in unraveling the complex etiology of ASD and guiding the development of personalized treatment strategies [ 63 ]. The development of these technologies has not only improved our understanding of the complex etiology of ASD, but also provided more precise and effective treatment options for ASD patients. Although most of these emerging biotechnologies are still in the research phase, they bring hope and anticipation for the future of ASD treatment and management. As research progresses and technology matures, it is expected that these innovative approaches will bring substantial benefits to individuals with ASD and their families.
Interaction between social policy and ASD research
The interaction between social policy and ASD research is key to achieving better social inclusion and quality of life for individuals with ASD and their families. Effective social policies can provide the necessary financial support and legal framework for ASD research, promoting a deeper understanding of ASD and the development of new treatments. For example, policies can promote collaboration in interdisciplinary research, encourage the use of innovative technologies and methods, and support long-term follow-up studies. In addition, social policies play a crucial role in ensuring that ASD research results are translated into practical applications and that education, employment, and social services are provided to individuals with ASD. Through the development of inclusive education policies, employment assistance programs, and the provision of integrated social services, policies can help individuals with ASD realize their potential and better integrate into society. At the same time, advances in ASD research also provide a scientific basis for the development of more targeted and effective social policies, helping policymakers understand the needs of individuals with ASD and develop more precise support measures. Thus, there is a close interplay between social policy and ASD research, which together have contributed to the advancement of the understanding of ASD and coping strategies.
Limitations of the current research
Although significant progress has been made in ASD research, a number of key limitations remain. First, the etiology of ASD is extremely complex, involving genetic and environmental factors and their interactions, making it extremely challenging to identify specific etiologies and develop targeted treatment strategies. Second, the heterogeneity of ASD is reflected in the extreme variability of symptoms among patients, which makes it difficult to develop uniform diagnostic criteria and treatment approaches. In addition, most studies have focused on children, and adult patients with ASD have been relatively understudied, which limits the understanding of the full lifespan of ASD. In terms of research methodology, most current ASD research relies on small, short-term studies, which may affect the broad applicability of results and the assessment of long-term effectiveness. In addition, although advances in technology have provided new tools for ASD diagnosis and intervention, the popularization and application of these technologies still face economic and resource constraints. Finally, ASD research is unequal across the globe, with far more research conducted in resource-rich countries and regions than in resource-limited areas. This imbalance limits a comprehensive understanding of ASD in different cultural and social contexts. Therefore, to overcome these limitations, more interdisciplinary, cross-cultural, and long-term research, as well as global collaborations, are needed to deepen the understanding of ASD and improve the quality of life of individuals with ASD.
Perspectives on future research
The outlook for future prevention and treatment of ASD points in a more individualized, integrated, and technology-driven direction. With a deeper understanding of the genetic and environmental factors of ASD, it is expected that more targeted interventions and therapeutic strategies will be developed that will be based on an individual's specific genetic background and pathologic characteristics. The application of precision medicine is expected to improve treatment outcomes, reduce unwanted side effects, and optimize resource allocation. Meanwhile, technological advances, particularly artificial intelligence, machine learning, and virtual reality, are expected to revolutionize the way ASDs are diagnosed, monitored, and treated. These technologies are capable of delivering customized learning and treatment programs that enhance the acceptability and effectiveness of interventions. In addition, interdisciplinary research will be strengthened, and social policies and public health strategies will focus more on early screening and intervention, as well as increasing public awareness and understanding of ASD. Most importantly, the future of ASD prevention and treatment will place greater emphasis on the needs of patients and families, promote social integration and employment of patients, and improve their quality of life. As society's awareness of diversity and inclusion increases, individuals with ASD will receive more support and respect and enjoy fuller opportunities for social participation.
Author information
Authors and affiliations.
Department of Rehabilitation, The Second Affiliated Hospital of Shandong First Medical University, Taian, Shandong, China
Lei Qin, Wenjing Ning & Mengmeng Cui
Department of Intensive Care Medicine, Feicheng People’s Hospital, Taian, Shandong, China
Haijiao Wang
Department of Central Laboratory, The Affiliated Taian City Central Hospital of Qingdao University, Taian, China
You can also search for this author in PubMed Google Scholar
Contributions
LQ, HW and WN wrote the draft of the manuscript. MC and QW revised this manuscript. All the listed authors have made a substantial, direct, and intellectual contribution to the work, and approved its publication.
Corresponding authors
Correspondence to Mengmeng Cui or Qian Wang .
Ethics declarations
Ethical approval and consent to participate.
Not applicable.
Competing interests
The authors declare there are no competing interests.
Additional information
Publisher's note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
Qin, L., Wang, H., Ning, W. et al. New advances in the diagnosis and treatment of autism spectrum disorders. Eur J Med Res 29 , 322 (2024). https://doi.org/10.1186/s40001-024-01916-2
Download citation
Received : 17 April 2024
Accepted : 01 June 2024
Published : 10 June 2024
DOI : https://doi.org/10.1186/s40001-024-01916-2
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Autism spectrum disorder (ASD)
- Diagnostic methods
- Treatment strategies
- Precision medicine
- Emerging biotechnology
European Journal of Medical Research
ISSN: 2047-783X
- General enquiries: [email protected]
- About Autism
- Is It Autism?
- Starting Intervention
- Prenatal Factors
- Autism Assessment Tools
- Diagnostic Checklist
- Autism Treatment Evaluation Checklist (ATEC)
- Understanding and Treating Self-Injurious Behavior Tool
- Autism Support
- Expert Webinars
- Newly Diagnosed
- Studies Seeking Participants
- ARI-Funded Research Studies 2023
- ARI Think Tanks
- Participate in Studies
- ARI-Funded Research By Year
- Mission Statement
- Board of Directors
- Scientific Advisory Board
- National Autism History Museum Hours
- ARI's Latest Accomplishments
- Annual Reports
- Financials - Audit Reports/990s
- Donate Cryptocurrency
- Donate Stock/Mutual Funds
In 1964, ARI’s founder, Dr. Bernard Rimland, published his seminal book,
Infantile Autism
The Syndrome & It’s Implications for a Neural Theory of Behavior
His work exposed illogical assumptions about the underlying causes of autism & shifted autism research toward the biomedical track. Sixty years later, Rimland’s legacy continues via cross-sector, collaborative autism investigation, education & care.
In 1964, Dr. Bernard Rimland published his seminal book,
The Syndrome & Its Implications for a Neural Theory of Behavior
His groundbreaking work laid the foundation for contemporary autism research & care.
ARI donors support research that has practical application in the evolution of autism understanding and the lives of autistic people. Last fall, ARI awarded more than $400,000 in grants to fund research on evidence-based therapeutic interventions and underlying biological mechanisms.
We work to advance the biological understanding of autism. Whether you’re an autistic individual, parent, professional, or researcher, we’re here to connect you with information you need.
Understanding Autism
Is it autism.
Learn early signs and prevalence of autism—and other ARI resources for understanding developmental disorders.
Symptoms of Autism
Learn more about the physical and behavioral symptoms associated with autism spectrum disorder.
Screening & Assessment
Explore information, research and tools available for support with autism screening and assessment needs.
Explore resources, research and tools for best care and treatment practices to help individuals with autism.
Education & Support
For autistic individuals, for parents & care providers, for clinicians & therapists, for researchers, help us support autism research and education, recent & upcoming webinars.

Disordered Eating and Autism – Obesity
autismAdmin 2024-06-05T14:39:19-05:00 October 23rd, 2024 |

Caregiver Strategies for Building Infant Social Interaction
autismAdmin 2024-06-24T15:39:22-05:00 October 9th, 2024 |
Emerging Findings: Pediatric Acute Neuropsychiatric Syndrome
autismAdmin 2024-06-17T15:37:46-05:00 October 2nd, 2024 |

Wellbeing Wins: Integrating Positive Psychology into the Autism Community
autismAdmin 2024-08-16T11:41:39-05:00 September 25th, 2024 |
Get News & Updates from the Autism Research Institute
- * First Last
- Phone This field is for validation purposes and should be left unchanged.
Autism News & Editorials

ARI’s Latest Annual Report and Impact
autismAdmin 2024-08-27T12:54:07-05:00 August 27th, 2024 |

The Low-Hanging Fruit: Exploring Monogenic Syndromes with Elevated Rates of Autism
autismAdmin 2024-08-07T10:37:37-05:00 July 15th, 2024 |

Gender, Sexuality, and Autism
autismAdmin 2024-08-07T10:38:10-05:00 July 12th, 2024 |
Autism and Trauma
autismAdmin 2024-08-07T10:39:44-05:00 July 8th, 2024 |
Privacy Overview
- See us on facebook
- See us on instagram
- See us on twitter
Research Studies
Currently Recruiting or Active Research Studies
Please download the document below for our current recruiting studies organized by age range.
Study Title
Study description, spark (simons powering autism research) study.
Available in English and Spanish.
If you or your child has a professional diagnosis of autism, Stanford University invites you to learn more about SPARK, a new online research study sponsored by the Simons Foundation Autism Research Initiative. The mission of SPARK is clear: speed up research and advance understanding of autism by creating the nation’s largest autism study. Joining SPARK is simple – register online and provide a DNA sample via a saliva collection kit in the comfort of your own home. Together, we can help spark a better future for all individuals and families affected by autism.
Register by contacting us at [email protected] or online at www.sparkforautism.org/stanford .
SPARK está trabajando para fomentar la investigación y mejorar nuestra comprensión del autismo. Stanford y más de 30 de las principales escuelas de medicina y centros de investigación del autismo del país forman parte de este esfuerzo.
- Participar en SPARK es gratis y se puede hacer completamente desde casa.
- Muchas de las encuestas de SPARK aportan informes personalizados.
- Los participantes serán notificados en caso de haber otras oportunidades de investigación.
- Los individuos con autismo podrán recibir códigos de regalo de Amazon por un valor de hasta 50 dólares (uno por familia) después de la recepción de sus muestras de saliva.
Para inscribirse en SPARK: https://sparkforautism.org/Stanford/ES
La inscripción suele llevar unos 20 minutos y puede empezar y parar si lo necesita. Una vez que se registre y complete unos cuestionarios en línea, le enviaremos un kit para recolectar saliva a su domicilio. Para obtener más información, envíe un correo electrónico a [email protected]
Language Treatment Trial for Children with Autism
Researchers at Stanford University are currently recruiting children with autism spectrum disorder to identify MRI-based markers of response to treatment with Pivotal Response Treatment (PRT) targeting language abilities. Children with autism spectrum disorder between the ages of 2 and 4 years 11 months are invited to participate. This study involves up to a 5 month time commitment. The participant must be willing to complete cognitive and behavioral assessments (such as IQ and language testing) and be able to either sleep (young children) or lie still in the scanner during an MRI. After a successful MRI, the participant will be randomized into the PRT trial or DTG (Delayed Treatment Group). PRT will consist of 16 weekly, 60-90 minute sessions of parent training in PRT over a 16 week time period. DTG will consist of your child’s treatments as usual in the community and measurements and questionnaires will need to be filled out on three study visits over the course of the 16 weeks. After completion of the DTG, the participant will be offered PRT parent training sessions similar to the PRT group. There is no cost to participate in the study. If you would like to participate or if you have any questions please call (650) 736-1235 or email: [email protected] to discuss the study in more detail.
2 and 4 years,11 months
Targeting the Neurobiology of Restricted and Repetitive Behaviors in Children with Autism Using N-acetylcysteine Randomized Control Trial
We are recruiting children autism to participate in a study examining the treatment effects of an over-the-counter dietary supplement on the brain.
Eligibility: Children with autism spectrum disorder who -
· are aged between 3 and 12 years old
· exhibit restricted and repetitive behaviors
· will drink N-acetyl cysteine dissolved in water
· will undergo brain scanning (asleep or awake) with magnetic resonance imaging (MRI)
· will undergo brain scanning with electroencephalography (EEG)
The study will take place over 3 to 6 visits (some remotely over Zoom) and the approximate time required is about 10 to 12 hours. Individuals that are able to complete both of the MRI/EEG sessions will be compensated $50.
You can find more information about our NAC studies at https://redcap.link/NACforAutism .
If you have any questions please call 650-736-1235 or email: [email protected] .
3 to 12 years
Autism Center of Excellence Sleep Study
Dear Parents,
We are excited to tell you about a new research study for children. We are looking to partner with parents who have children that are between the ages of 4 and 17 years old, with and without an Autism Spectrum Disorder (ASD) diagnosis.
What is involved?
- In-person cognitive and behavioral assessments
- Day-time Electroencephalogram (EEG)
- In-home, 2 night sleep monitoring session
- Collection of saliva to measure cortisol and melatonin levels
- Wearing a watch device that tracks sleep and daily activity
What will I receive if I participate?
- Research sleep report and behavioral testing summary upon request
- $50 for each in-person visit to Stanford and $100 for the 2 night in-home sleep assessment
Treatment extension study:
- If your child has ASD, sleep difficulties, and ages 8-17, they may also qualify for sleep medication trials
Interested in participating or want to learn more? Click Here!
If you would like to reach out to our team directly with any questions, please contact our team below!
Email: [email protected]
650-498-7215
4 to 17 years
Pregnenolone Randomized Controlled Trial
Neurosteroid Pregnenolone Treatment for Irritability in Adolescents with Autism
Medication treatments for core symptoms of autism spectrum disorder (ASD) continue to be unmet medical needs. The only medications approved by the U.S. Food and Drug Administration (FDA) for the treatment of individuals with ASD are effective in treating irritability and associated aggressive behaviors, but these medications can also cause severe long-term side effects such as diabetes and involuntary motor movements. Therefore, effective medications with more tolerable side effect profiles are highly desirable. This profile is consistent with pregnenolone (PREG). PREG belongs to a new class of hormones known as neurosteroids, which have been shown to be effective in treating various psychiatric conditions including bipolar depression and schizophrenia. As compared to currently FDA-approved medications, our preliminary data suggested that PREG may represent a potentially effective and well-tolerated agent for treating irritability in individuals with ASD. In addition, our experience suggests that PREG might be helpful in improving selected core symptoms such as social deficits and sensory abnormalities of ASD. This study provides the opportunity to further explore the usefulness of PREG in the treatment of irritability and some core symptoms of ASD. We are performing a 12-week randomized double-blind controlled pilot trial to examine the effectiveness of orally administered PREG in reducing irritability and associated behaviors in adolescents with ASD. In this study, we also aim to examine the usefulness of biomarkers (blood levels of neurosteroids, eyetracking and brain wave recording) in predicting treatment response and assessing biologic changes with PREG treatment.
Link to study in Stanford's Clinical Trials Directory
14 to 25 years
Trial of Center-Based vs. In-Home Pivotal Response Treatment (PRT) in Autism (PRT-HvC)
Do you have a child (2-5 years old) with autism and want an intensive center-based or in-home intervention?
Stanford University researchers are recruiting children with autism and their parents to participate in a study examining the effectiveness of a center-based vs. in-home Pivotal Response Treatment (PRT) program in targeting social communication abilities in young children with autism.
Participants must:
- Be diagnosed with Autism Spectrum Disorder
- Be between the ages of 2 years and 5 years 11 months
- Be able to attend 3-hour research treatment sessions 4 days per week and participate in parent training
Based on behavioral screening assessments, children who are eligible will be randomly assigned to either center-based intervention, in-home intervention, or treatment as usual. Those assigned to the treatment-as-usual group will receive treatment after the 16–week period is completed.
Call 650-736-1235 or email [email protected] to learn more.
https://clinicaltrials.gov/ct2/show/NCT04899544
2 to 5 years
Improving Access to Pivotal Response Treatment (PRT) via Telehealth Parent Training
There is an urgent need for improved access to effective autism treatments. With advances in technology, distance learning models have particular promise for families who cannot access evidence-based parent training locally or may be on long wait-lists for behavioral treatments. Pivotal Response Treatment (PRT) is an established treatment for autism spectrum disorder (ASD); however, a telehealth PRT model has not yet been evaluated in a controlled trial. This study will examine the effects of training parents in PRT via secure video conferencing and investigate 1) whether parents can learn via telehealth to deliver PRT in the home setting (PRT-T) and 2) whether their children will show greater improvement in functional communication skills compared to children in a waitlist control group. Participants will include 40 children age 2 to 5 years with ASD and significant language delay. Eligible children will be randomly assigned to either PRT-T or waiting list. Weekly 60-minute parent training sessions will be delivered for 12 weeks via secure video conferencing software by a PRT-trained study therapist. Link: https://clinicaltrials.gov/ct2/show/NCT04042337
Note: Participants must live at least 200 miles away from Stanford University (i.e., this study is geared towards out-of-state families or families living at a distance)
A Center Based Randomized Controlled Trial of Pivotal Response Treatment for Preschoolers With Autism
Researchers at Stanford University are currently recruiting children with autism and their parents to participate in a study examining the effectiveness of a center-based Pivotal Response Treatment (PRT) program in targeting social communication abilities in young children with autism. We are currently recruiting children diagnosed with ASD and social communication deficits, aged 2:0 to 3:11 years. Children who are eligible based on behavioral screening assessments will be randomly assigned to either an immediate treatment (PRT) group or a delayed treatment group (DTG). If randomized into the PRT group, the 12-week treatment will consist of a combination of one weekly 60-minute individual parent training session and 12 weekly hours (approximately 3 hours per day for 4 days per week) with your child in a center-based group preschool environment at Stanford University. If randomized into the delayed treatment group, the children will wait 12 weeks to receive the PRT treatment and continue any treatment they are receiving as usual in the community. The cost of clinic-based services varies based on individual family health insurance plans.
For more information, please call (650) 736-1235 or email [email protected] to discuss the study in more detail.
2 and 3 years,11 months
Natural History Study of Individuals with Autism and Germline Heterozygous PTEN Mutations
The goal of this study is to gain a better understanding of PTEN mutation syndromes to identify early markers and ultimately effective interventions for autism spectrum disorder. Individuals 18 months or older are eligible to participate if they have been diagnosed with PTEN hamartoma tumor syndrome. The study involves five visits over a two year period. Three of the visits occur on-site at a study location. The other two visits occur as phone calls. The on-site visits include a blood draw, physical/neurological exams and behavioral testing.
Study Webpage
18 months and older
Active Studies, not Recruiting
An open-label pilot study of esomeprazole in children with autism.
Researchers at Stanford University are currently examining the effectiveness of esomeprazole in improving social communication deficits in children with Autism Spectrum Disorder (ASD). Esomeprazole is currently FDA-approved for children ages 1 and up for gastroesophageal reflux disease (GERD) and has been identified as a potential treatment for improving social communication in children with ASD. Children with ASD ages 2 through 6 years are invited to participate. The child must be willing to take esomeprazole orally for at least 8 weeks, complete diagnostic and behavioral assessments, and be free of serious medical problems. There is also an optional research blood draw. The study will require visits to Stanford University and the parent/caregiver will be required to complete questionnaires for each visit.
For more information, please go to https://is.gd/ASDstudy , call (650) 736-1235, or email [email protected] .
2 to 6 years
Vasopressin Treatment Trial for Children with Autism
The purpose of this clinical trial is to investigate the effectiveness of vasopressin nasal spray for treating symptoms associated with autism. Vasopressin is a hormone that is produced naturally within the body and has been implicated in regulating social behaviors. It has been proposed that administration of the hormone may also help improve social functioning in individuals with autism.
Link to study at clinicaltrials.gov
6 to 17 years
Autism spectrum disorder

Autism spectrum disorder (ASD) refers any one of a group of disorders with an onset typically occurring during the preschool years and characterized by difficulties with social communication and social interactionalong with restricted and repetitive patterns in behaviors, interests, and activities.
Autism, Asperger’s syndrome, and childhood disintegrative disorder are no longer considered distinct diagnoses, and medical or genetic disorders that may be associated with ASD, such as Rett’s syndrome, are identified only as specifiers of the disorder.
Adapted from the APA Dictionary of Psychology
Resources from APA

Knowing me, knowing you: Self defining memories in adolescents with and without an autism spectrum disorder
Do autistic adolescents and non-autistic adolescents recall self-defining and everyday memories in the same way?

Amy Pearson, PhD
Pearson is an autistic researcher who uses creative research strategies to understand friendship, bullying, and other aspects of autism

“Autism research is in crisis”: A mixed method study of researcher’s constructions of autistic people and autism research
Learn how the involvement of autistic individuals in research might transform the way autism is understood and discussed in the scientific world

Diagnosis as a new beginning not an end: A participatory photovoice study on navigating an autism diagnosis in adulthood
Uncover the unique stories of women seeking autism diagnosis in adulthood, captured through the lens of their own cameras
More resources about ASD
What APA is doing

Intellectual and Developmental Disabilities/Autism Spectrum Disorder
APA’s Division 33 is dedicated to advancing psychological research, professional education, and clinical services that increase quality of life in individuals with intellectual and developmental disabilities or autism spectrum disorder across the life course.
Autism Spectrum Disorder
Autism Spectrum Disorder in Children and Adolescents
Innovative Investigations of Language in Autism Spectrum Disorder
Behavioral Interventions in Schools, 2nd Ed.
Autism and Your Teen
Magination Press children’s books

Autism, The Invisible Cord

How Are You, Verity?

All My Stripes

Russell's World

Asperger's Rules!
Journal special issues
Autism and Other Child Developmental Disorders
- Skip to main content
- Skip to main navigation
- Awards & Honors
- News by topic
- News archives
- E-Newsletter
- Tuesday Newsday
- UCSC Magazine
- Administrative Messages
Home / 2024 / August / Researchers to investigate genetic roots of autism, look for new treatments
Researchers to investigate genetic roots of autism, look for new treatments
A $12.3 million award will support research out of UC Santa Cruz, UC San Francisco, and UC Berkeley
August 30, 2024
By Emily Cerf

A new award from the California Institute for Regenerative Medicine (CIRM) will support a team of UC Santa Cruz researchers in exploring the genetic underpinnings of autism spectrum disorder (ASD) and investigating possible treatments, in collaboration with teams at UC San Francisco and UC Berkeley. ASD affects one in 22 children in California, but there is a wide range of variability in how it presents. Many genetic variants have been linked to autism, but research has not clearly defined how and why these variations affect people differently and result in varying severity of autism. The SSPsyGene consortium, an effort to study genes linked to neuropsychiatric conditions involving UCSC researchers, recently prioritized 120 gene variants associated with ASD. This work will form the basis of the new project, as the researchers will focus on the gene pathways that most commonly lead to ASD. They will investigate the biological processes that cause ASD using cell culture models of brain development derived from pluripotent stem cells. They will use this information to develop laboratory tests that can be used to investigate targets for treatment. The researchers will use brain organoids, miniature models of brain tissue grown in the lab, to narrow down the most clinically relevant observable signs of ASD in their models. The Braingeneers group have become leaders in automating the cultivation and measuring the properties of brain organoids as part of their Live Cell Technology Center . This project will be the first time they use their expertise to study neuropsychiatric conditions. “The Braingeeners group has been working since 2018, and a big part of that has been developing methodologies and platforms for more robust generation and analysis of brain organoids,” said Sofie Salama, Professor of Molecular, Cellular and Developmental Biology who will be an investigator on this project. “This is a really exciting opportunity where the rubber is hitting the road — we can test how these platforms we've developed allow us to study how organoid phenotypes can shed light on the variants that can lead to human diseases.” CIRM has awarded $12.3 million in total funding for this project through its pilot ReMIND (Research using Multidisciplinary, Innovative Approaches in Neuro Diseases) Program. The project will be led by UCSF Assistant Professor of Neurology Alex Pollen. $4.1 million of this funding will go to UC Santa Cruz, where research will be spearheaded by scientists in the Braingeneers group, including Salama, Research Scientist Mohammed Mostajo-Radji, Associate Professor of Electrical and Computer Engineering Mircea Teodorescu, and Distinguished Professor of Biomolecular Engineering David Haussler.
“We are incredibly excited to combine the scalable technologies developed by our Braingeneers group and our Center for Live Cell Genomics with our experience and collaborations within the neuroscience community to address a critical question: how do genetic perturbations in brain development lead to circuit-level phenotypes in autism?” Mostajo-Radji said. “We are deeply grateful to CIRM and the voters of California who supported Proposition 14 in 2020, making this project possible. We are thrilled to take on this challenge alongside our colleagues at UCSF and UC Berkeley.”
“While we understand through our other funded projects that organoids can develop functional properties resembling those of a developing brain, the exact genetic mechanisms of how autism spectrum disorder (ASD) affects developing brains remain unclear,” Teodorescu said. “To fully grasp these mechanisms, in this project we will conduct a large-scale, automated experimental study. This will generate a vast amount of data, requiring advanced AI-powered data analysis."
The team aims to understand how ASD presents differently across various populations, and what genetic factors might protect certain populations against ASD, by studying these genetic variants in cells from people with diverse ancestral backgrounds. At the end of this project, they will produce a system to classify different types of ASD based on genetic information. At UC Berkeley, researchers include Associate Professor of Molecular and Cell Biology Helen Bateup; Professor of Chemical and Biomolecular Engineering, Bioengineering, and Neuroscience David Schaffer. At UCSF, researchers include Pollen, Associate Professor of Biochemistry and Biophysics Martin Kampmann, Professor of Neurology Saul Kato, and Professor of Neurology and Pediatrics Elliott Sherr. The successful collaborative grant writing was the result of the efforts of Lise Barbé, the newly hired grants coordinator at QB3 , where investigator Schaffer is the Executive Director.
University News
- University News Home
- Monthly Newsletter
Other News & Events
- Campus Calendars

- UCSC Chancellor
- Press Releases
- Contacts for Reporters
- Send us an email
- Report an accessibility barrier
- Land Acknowledgment
- Accreditation
Last modified: August 30, 2024 162.248.224.4
- Patient Care & Health Information
- Diseases & Conditions
- Autism spectrum disorder
Autism spectrum disorder is a condition related to brain development that impacts how a person perceives and socializes with others, causing problems in social interaction and communication. The disorder also includes limited and repetitive patterns of behavior. The term "spectrum" in autism spectrum disorder refers to the wide range of symptoms and severity.
Autism spectrum disorder includes conditions that were previously considered separate — autism, Asperger's syndrome, childhood disintegrative disorder and an unspecified form of pervasive developmental disorder. Some people still use the term "Asperger's syndrome," which is generally thought to be at the mild end of autism spectrum disorder.
Autism spectrum disorder begins in early childhood and eventually causes problems functioning in society — socially, in school and at work, for example. Often children show symptoms of autism within the first year. A small number of children appear to develop normally in the first year, and then go through a period of regression between 18 and 24 months of age when they develop autism symptoms.
While there is no cure for autism spectrum disorder, intensive, early treatment can make a big difference in the lives of many children.
Products & Services
- Children’s Book: My Life Beyond Autism
Some children show signs of autism spectrum disorder in early infancy, such as reduced eye contact, lack of response to their name or indifference to caregivers. Other children may develop normally for the first few months or years of life, but then suddenly become withdrawn or aggressive or lose language skills they've already acquired. Signs usually are seen by age 2 years.
Each child with autism spectrum disorder is likely to have a unique pattern of behavior and level of severity — from low functioning to high functioning.
Some children with autism spectrum disorder have difficulty learning, and some have signs of lower than normal intelligence. Other children with the disorder have normal to high intelligence — they learn quickly, yet have trouble communicating and applying what they know in everyday life and adjusting to social situations.
Because of the unique mixture of symptoms in each child, severity can sometimes be difficult to determine. It's generally based on the level of impairments and how they impact the ability to function.
Below are some common signs shown by people who have autism spectrum disorder.
Social communication and interaction
A child or adult with autism spectrum disorder may have problems with social interaction and communication skills, including any of these signs:
- Fails to respond to his or her name or appears not to hear you at times
- Resists cuddling and holding, and seems to prefer playing alone, retreating into his or her own world
- Has poor eye contact and lacks facial expression
- Doesn't speak or has delayed speech, or loses previous ability to say words or sentences
- Can't start a conversation or keep one going, or only starts one to make requests or label items
- Speaks with an abnormal tone or rhythm and may use a singsong voice or robot-like speech
- Repeats words or phrases verbatim, but doesn't understand how to use them
- Doesn't appear to understand simple questions or directions
- Doesn't express emotions or feelings and appears unaware of others' feelings
- Doesn't point at or bring objects to share interest
- Inappropriately approaches a social interaction by being passive, aggressive or disruptive
- Has difficulty recognizing nonverbal cues, such as interpreting other people's facial expressions, body postures or tone of voice
Patterns of behavior
A child or adult with autism spectrum disorder may have limited, repetitive patterns of behavior, interests or activities, including any of these signs:
- Performs repetitive movements, such as rocking, spinning or hand flapping
- Performs activities that could cause self-harm, such as biting or head-banging
- Develops specific routines or rituals and becomes disturbed at the slightest change
- Has problems with coordination or has odd movement patterns, such as clumsiness or walking on toes, and has odd, stiff or exaggerated body language
- Is fascinated by details of an object, such as the spinning wheels of a toy car, but doesn't understand the overall purpose or function of the object
- Is unusually sensitive to light, sound or touch, yet may be indifferent to pain or temperature
- Doesn't engage in imitative or make-believe play
- Fixates on an object or activity with abnormal intensity or focus
- Has specific food preferences, such as eating only a few foods, or refusing foods with a certain texture
As they mature, some children with autism spectrum disorder become more engaged with others and show fewer disturbances in behavior. Some, usually those with the least severe problems, eventually may lead normal or near-normal lives. Others, however, continue to have difficulty with language or social skills, and the teen years can bring worse behavioral and emotional problems.
When to see a doctor
Babies develop at their own pace, and many don't follow exact timelines found in some parenting books. But children with autism spectrum disorder usually show some signs of delayed development before age 2 years.
If you're concerned about your child's development or you suspect that your child may have autism spectrum disorder, discuss your concerns with your doctor. The symptoms associated with the disorder can also be linked with other developmental disorders.
Signs of autism spectrum disorder often appear early in development when there are obvious delays in language skills and social interactions. Your doctor may recommend developmental tests to identify if your child has delays in cognitive, language and social skills, if your child:
- Doesn't respond with a smile or happy expression by 6 months
- Doesn't mimic sounds or facial expressions by 9 months
- Doesn't babble or coo by 12 months
- Doesn't gesture — such as point or wave — by 14 months
- Doesn't say single words by 16 months
- Doesn't play "make-believe" or pretend by 18 months
- Doesn't say two-word phrases by 24 months
- Loses language skills or social skills at any age
There is a problem with information submitted for this request. Review/update the information highlighted below and resubmit the form.
From Mayo Clinic to your inbox
Sign up for free and stay up to date on research advancements, health tips, current health topics, and expertise on managing health. Click here for an email preview.
Error Email field is required
Error Include a valid email address
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Thank you for subscribing!
You'll soon start receiving the latest Mayo Clinic health information you requested in your inbox.
Sorry something went wrong with your subscription
Please, try again in a couple of minutes
Autism spectrum disorder has no single known cause. Given the complexity of the disorder, and the fact that symptoms and severity vary, there are probably many causes. Both genetics and environment may play a role.
- Genetics. Several different genes appear to be involved in autism spectrum disorder. For some children, autism spectrum disorder can be associated with a genetic disorder, such as Rett syndrome or fragile X syndrome. For other children, genetic changes (mutations) may increase the risk of autism spectrum disorder. Still other genes may affect brain development or the way that brain cells communicate, or they may determine the severity of symptoms. Some genetic mutations seem to be inherited, while others occur spontaneously.
- Environmental factors. Researchers are currently exploring whether factors such as viral infections, medications or complications during pregnancy, or air pollutants play a role in triggering autism spectrum disorder.
No link between vaccines and autism spectrum disorder
One of the greatest controversies in autism spectrum disorder centers on whether a link exists between the disorder and childhood vaccines. Despite extensive research, no reliable study has shown a link between autism spectrum disorder and any vaccines. In fact, the original study that ignited the debate years ago has been retracted due to poor design and questionable research methods.
Avoiding childhood vaccinations can place your child and others in danger of catching and spreading serious diseases, including whooping cough (pertussis), measles or mumps.
Risk factors
The number of children diagnosed with autism spectrum disorder is rising. It's not clear whether this is due to better detection and reporting or a real increase in the number of cases, or both.
Autism spectrum disorder affects children of all races and nationalities, but certain factors increase a child's risk. These may include:
- Your child's sex. Boys are about four times more likely to develop autism spectrum disorder than girls are.
- Family history. Families who have one child with autism spectrum disorder have an increased risk of having another child with the disorder. It's also not uncommon for parents or relatives of a child with autism spectrum disorder to have minor problems with social or communication skills themselves or to engage in certain behaviors typical of the disorder.
- Other disorders. Children with certain medical conditions have a higher than normal risk of autism spectrum disorder or autism-like symptoms. Examples include fragile X syndrome, an inherited disorder that causes intellectual problems; tuberous sclerosis, a condition in which benign tumors develop in the brain; and Rett syndrome, a genetic condition occurring almost exclusively in girls, which causes slowing of head growth, intellectual disability and loss of purposeful hand use.
- Extremely preterm babies. Babies born before 26 weeks of gestation may have a greater risk of autism spectrum disorder.
- Parents' ages. There may be a connection between children born to older parents and autism spectrum disorder, but more research is necessary to establish this link.
Complications
Problems with social interactions, communication and behavior can lead to:
- Problems in school and with successful learning
- Employment problems
- Inability to live independently
- Social isolation
- Stress within the family
- Victimization and being bullied
More Information
- Autism spectrum disorder and digestive symptoms
There's no way to prevent autism spectrum disorder, but there are treatment options. Early diagnosis and intervention is most helpful and can improve behavior, skills and language development. However, intervention is helpful at any age. Though children usually don't outgrow autism spectrum disorder symptoms, they may learn to function well.
- Autism spectrum disorder (ASD). Centers for Disease Control and Prevention. https://www.cdc.gov/ncbddd/autism/facts.html. Accessed April 4, 2017.
- Uno Y, et al. Early exposure to the combined measles-mumps-rubella vaccine and thimerosal-containing vaccines and risk of autism spectrum disorder. Vaccine. 2015;33:2511.
- Taylor LE, et al. Vaccines are not associated with autism: An evidence-based meta-analysis of case-control and cohort studies. Vaccine. 2014;32:3623.
- Weissman L, et al. Autism spectrum disorder in children and adolescents: Overview of management. https://www.uptodate.com/home. Accessed April 4, 2017.
- Autism spectrum disorder. In: Diagnostic and Statistical Manual of Mental Disorders DSM-5. 5th ed. Arlington, Va.: American Psychiatric Association; 2013. http://dsm.psychiatryonline.org. Accessed April 4, 2017.
- Weissman L, et al. Autism spectrum disorder in children and adolescents: Complementary and alternative therapies. https://www.uptodate.com/home. Accessed April 4, 2017.
- Augustyn M. Autism spectrum disorder: Terminology, epidemiology, and pathogenesis. https://www.uptodate.com/home. Accessed April 4, 2017.
- Bridgemohan C. Autism spectrum disorder: Surveillance and screening in primary care. https://www.uptodate.com/home. Accessed April 4, 2017.
- Levy SE, et al. Complementary and alternative medicine treatments for children with autism spectrum disorder. Child and Adolescent Psychiatric Clinics of North America. 2015;24:117.
- Brondino N, et al. Complementary and alternative therapies for autism spectrum disorder. Evidence-Based Complementary and Alternative Medicine. http://dx.doi.org/10.1155/2015/258589. Accessed April 4, 2017.
- Volkmar F, et al. Practice parameter for the assessment and treatment of children and adolescents with autism spectrum disorder. Journal of the American Academy of Child and Adolescent Psychiatry. 2014;53:237.
- Autism spectrum disorder (ASD). Eunice Kennedy Shriver National Institute of Child Health and Human Development. https://www.nichd.nih.gov/health/topics/autism/Pages/default.aspx. Accessed April 4, 2017.
- American Academy of Pediatrics policy statement: Sensory integration therapies for children with developmental and behavioral disorders. Pediatrics. 2012;129:1186.
- James S, et al. Chelation for autism spectrum disorder (ASD). Cochrane Database of Systematic Reviews. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD010766.pub2/abstract;jsessionid=9467860F2028507DFC5B69615F622F78.f04t02. Accessed April 4, 2017.
- Van Schalkwyk GI, et al. Autism spectrum disorders: Challenges and opportunities for transition to adulthood. Child and Adolescent Psychiatric Clinics of North America. 2017;26:329.
- Autism. Natural Medicines. https://naturalmedicines.therapeuticresearch.com. Accessed April 4, 2017.
- Autism: Beware of potentially dangerous therapies and products. U.S. Food and Drug Administration. https://www.fda.gov/ForConsumers/ConsumerUpdates/ucm394757.htm?source=govdelivery&utm_medium=email&utm_source=govdelivery. Accessed May 19, 2017.
- Drutz JE. Autism spectrum disorder and chronic disease: No evidence for vaccines or thimerosal as a contributing factor. https://www.uptodate.com/home. Accessed May 19, 2017.
- Weissman L, et al. Autism spectrum disorder in children and adolescents: Behavioral and educational interventions. https://www.uptodate.com/home. Accessed May 19, 2017.
- Huebner AR (expert opinion). Mayo Clinic, Rochester, Minn. June 7, 2017.
Associated Procedures
- Cognitive behavioral therapy
News from Mayo Clinic
- Demystifying my diagnosis of autism July 19, 2024, 02:00 p.m. CDT
- Understanding autism: The path to diagnosis, awareness and support April 28, 2024, 11:00 a.m. CDT
- 10 significant studies from Mayo Clinic's Center for Individualized Medicine in 2023 Dec. 30, 2023, 12:00 p.m. CDT
- Mayo Clinic 'mini-brain' study reveals possible key link to autism spectrum disorder Aug. 10, 2023, 04:00 p.m. CDT
- Symptoms & causes
- Diagnosis & treatment
- Doctors & departments
Mayo Clinic does not endorse companies or products. Advertising revenue supports our not-for-profit mission.
- Opportunities
Mayo Clinic Press
Check out these best-sellers and special offers on books and newsletters from Mayo Clinic Press .
- Mayo Clinic on Incontinence - Mayo Clinic Press Mayo Clinic on Incontinence
- The Essential Diabetes Book - Mayo Clinic Press The Essential Diabetes Book
- Mayo Clinic on Hearing and Balance - Mayo Clinic Press Mayo Clinic on Hearing and Balance
- FREE Mayo Clinic Diet Assessment - Mayo Clinic Press FREE Mayo Clinic Diet Assessment
- Mayo Clinic Health Letter - FREE book - Mayo Clinic Press Mayo Clinic Health Letter - FREE book
5X Challenge
Thanks to generous benefactors, your gift today can have 5X the impact to advance AI innovation at Mayo Clinic.
- Introduction
- Conclusions
- Article Information
Dispensations of folic acid and/or multivitamin vitamin supplements, folic acid supplements, and multivitamin supplements before childbirth.
The solid boxes represent the estimated relative risk adjusted for the study covariates, and the lines represent the corresponding 95% CI. For each exposure, the reference group was children whose mothers had no exposure in each corresponding interval.
eAppendix. Methods
eTable 1. Descriptive Characteristics of Autism Spectrum Disorder (ASD) Cases and Controls
eTable 2. Descriptive Characteristics of Autism Spectrum Disorder (ASD) Cases and Controls: Exposures in Sensitivity Analyses
eTable 3. Unadjusted Relative Risk (RR) Estimates and 95% Confidence Intervals From Sensitivity Analysis
eFigure 1. Schoenfeld Residual Plots to Assess Proportional Hazards for the Primary Exposures to Folic Acid and/or Multivitamin Before and During Pregnancy
eFigure 2. Schoenfeld Residual Plots to Assess Proportional Hazards for the Primary Exposures to Folic Acid Before and During Pregnancy
eFigure 3. Schoenfeld Residual Plots to Assess Proportional Hazards for the Primary Exposures to Multivitamin Supplement Before and During Pregnancy
eReferences
See More About
Select your interests.
Customize your JAMA Network experience by selecting one or more topics from the list below.
- Academic Medicine
- Acid Base, Electrolytes, Fluids
- Allergy and Clinical Immunology
- American Indian or Alaska Natives
- Anesthesiology
- Anticoagulation
- Art and Images in Psychiatry
- Artificial Intelligence
- Assisted Reproduction
- Bleeding and Transfusion
- Caring for the Critically Ill Patient
- Challenges in Clinical Electrocardiography
- Climate and Health
- Climate Change
- Clinical Challenge
- Clinical Decision Support
- Clinical Implications of Basic Neuroscience
- Clinical Pharmacy and Pharmacology
- Complementary and Alternative Medicine
- Consensus Statements
- Coronavirus (COVID-19)
- Critical Care Medicine
- Cultural Competency
- Dental Medicine
- Dermatology
- Diabetes and Endocrinology
- Diagnostic Test Interpretation
- Drug Development
- Electronic Health Records
- Emergency Medicine
- End of Life, Hospice, Palliative Care
- Environmental Health
- Equity, Diversity, and Inclusion
- Facial Plastic Surgery
- Gastroenterology and Hepatology
- Genetics and Genomics
- Genomics and Precision Health
- Global Health
- Guide to Statistics and Methods
- Hair Disorders
- Health Care Delivery Models
- Health Care Economics, Insurance, Payment
- Health Care Quality
- Health Care Reform
- Health Care Safety
- Health Care Workforce
- Health Disparities
- Health Inequities
- Health Policy
- Health Systems Science
- History of Medicine
- Hypertension
- Images in Neurology
- Implementation Science
- Infectious Diseases
- Innovations in Health Care Delivery
- JAMA Infographic
- Law and Medicine
- Leading Change
- Less is More
- LGBTQIA Medicine
- Lifestyle Behaviors
- Medical Coding
- Medical Devices and Equipment
- Medical Education
- Medical Education and Training
- Medical Journals and Publishing
- Mobile Health and Telemedicine
- Narrative Medicine
- Neuroscience and Psychiatry
- Notable Notes
- Nutrition, Obesity, Exercise
- Obstetrics and Gynecology
- Occupational Health
- Ophthalmology
- Orthopedics
- Otolaryngology
- Pain Medicine
- Palliative Care
- Pathology and Laboratory Medicine
- Patient Care
- Patient Information
- Performance Improvement
- Performance Measures
- Perioperative Care and Consultation
- Pharmacoeconomics
- Pharmacoepidemiology
- Pharmacogenetics
- Pharmacy and Clinical Pharmacology
- Physical Medicine and Rehabilitation
- Physical Therapy
- Physician Leadership
- Population Health
- Primary Care
- Professional Well-being
- Professionalism
- Psychiatry and Behavioral Health
- Public Health
- Pulmonary Medicine
- Regulatory Agencies
- Reproductive Health
- Research, Methods, Statistics
- Resuscitation
- Rheumatology
- Risk Management
- Scientific Discovery and the Future of Medicine
- Shared Decision Making and Communication
- Sleep Medicine
- Sports Medicine
- Stem Cell Transplantation
- Substance Use and Addiction Medicine
- Surgical Innovation
- Surgical Pearls
- Teachable Moment
- Technology and Finance
- The Art of JAMA
- The Arts and Medicine
- The Rational Clinical Examination
- Tobacco and e-Cigarettes
- Translational Medicine
- Trauma and Injury
- Treatment Adherence
- Ultrasonography
- Users' Guide to the Medical Literature
- Vaccination
- Venous Thromboembolism
- Veterans Health
- Women's Health
- Workflow and Process
- Wound Care, Infection, Healing
Others Also Liked
- Download PDF
- X Facebook More LinkedIn
Levine SZ , Kodesh A , Viktorin A, et al. Association of Maternal Use of Folic Acid and Multivitamin Supplements in the Periods Before and During Pregnancy With the Risk of Autism Spectrum Disorder in Offspring. JAMA Psychiatry. 2018;75(2):176–184. doi:10.1001/jamapsychiatry.2017.4050
Manage citations:
© 2024
- Permissions
Association of Maternal Use of Folic Acid and Multivitamin Supplements in the Periods Before and During Pregnancy With the Risk of Autism Spectrum Disorder in Offspring
- 1 Department of Community Mental Health, University of Haifa, Haifa, Israel
- 2 Department of Mental Health, Meuhedet Health Services, Tel Aviv, Israel
- 3 The Seaver Autism Center for Research and Treatment, Icahn School of Medicine at Mount Sinai, New York, New York
- 4 Department of Psychiatry, Icahn School of Medicine at Mount Sinai, New York, New York
- 5 Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden
- 6 Department of Psychiatry, Dalhousie University, Halifax, Nova Scotia, Canada
Question Does maternal folic acid and/or multivitamin supplement use before and/or during pregnancy increase the risk of autism spectrum disorder in offspring?
Findings In this case-control cohort study of 45 300 offspring, statistically significant associations between maternal vitamin supplement use before and/or during pregnancy and reduced risk of autism spectrum disorder in offspring were observed.
Meaning A reduced risk of autism spectrum disorder in children born to women who used the specified vitamin supplements before and during pregnancy has important public health implications; possible mechanisms include epigenetic modifications.
Importance The association of maternal use of folic acid and multivitamin supplements before and during pregnancy with the risk of autism spectrum disorder (ASD) in offspring is unclear.
Objective To examine the associations between the use of maternal folic acid and multivitamin supplements before and during pregnancy and the risk of ASD in offspring.
Design, Setting, and Participants A case-control cohort study of 45 300 Israeli children born between January 1, 2003, and December 31, 2007, were followed up from birth to January 26, 2015, for the risk of ASD. The cases were all children diagnosed with ASD and the controls were a random sample of 33% of all live-born children.
Exposures Maternal vitamin supplements were classified for folic acid (vitamin B 9 ), multivitamin supplements (Anatomical Therapeutic Chemical A11 codes vitamins A, B, C, and D), and any combination thereof exposed in the intervals before and during pregnancy.
Main Outcomes and Measures The association between maternal vitamin supplementation and the risk of ASD in offspring was quantified with relative risks (RRs) and their 95% CIs fitting Cox proportional hazards regression models adjusted for confounders. Sensitivity analyses were performed to test the robustness of the results.
Results Of the 45 300 children in the study (22 090 girls and 23 210 boys; mean [SD] age, 10.0 [1.4] years at the end of follow-up), 572 (1.3%) received a diagnosis of ASD. Maternal exposure to folic acid and/or multivitamin supplements before pregnancy was statistically significantly associated with a lower likelihood of ASD in the offspring compared with no exposure before pregnancy (RR, 0.39; 95% CI, 0.30-0.50; P < .001). Maternal exposure to folic acid and/or multivitamin supplements during pregnancy was statistically significantly associated with a lower likelihood of ASD in offspring compared with no exposure during pregnancy (RR, 0.27; 95% CI, 0.22-0.33; P < .001). Corresponding RRs were estimated for maternal exposure to folic acid before pregnancy (RR, 0.56; 95% CI, 0.42-0.74; P = .001), maternal exposure to folic acid during pregnancy (RR, 0.32; 95% CI, 0.26-0.41; P < .001), maternal exposure to multivitamin supplements before pregnancy (RR, 0.36; 95% CI, 0.24-0.52; P < .001), and maternal exposure to multivitamin supplements during pregnancy (RR, 0.35; 95% CI, 0.28-0.44; P < .001). The results generally remained statistically significant across sensitivity analyses.
Conclusions and Relevance Maternal exposure to folic acid and multivitamin supplements before and during pregnancy is associated with a reduced risk of ASD in the offspring compared with the offspring of mothers without such exposure.
Maternal vitamin deficiency during pregnancy is inconsistently associated with cognitive functioning in offspring. 1 However, maternal vitamin D deficiency may have specific associations with the risk of autism spectrum disorder (ASD) and intellectual disability (ID) in offspring. 2 Furthermore, maternal vitamin deficiency has also been linked with increased neural tube defects, 3 the incidence of which can be reduced by folic acid (FA) supplementation. 4 - 7 Hence, FA and multivitamin supplements are routinely recommended to pregnant women. 8
Epidemiologic studies report inconsistent associations between maternal supplementation with multivitamins or FA before and during pregnancy and the risk of ASD in offspring. Case-control studies in California identified a reduced risk of ASD in offspring with FA exposure 12 weeks before and 4 weeks into pregnancy 9 , 10 ; this risk was moderated by genetic variants involved in folate use. In population-based Norwegian studies, FA supplementation from 4 weeks before and 8 weeks into pregnancy was associated with reduced risks of ASD 11 and linguistic delay, 12 a key feature of ASD. 13 However, in studies from Denmark of the same exposure interval, maternal FA 14 , 15 and multivitamin 14 supplement use did not significantly reduce the risk of ASD in offspring. In the Stockholm Youth Cohort, multivitamin (but not FA) use reported at approximately 10 weeks into pregnancy was associated with a reduced risk of ASD with ID but not ASD without ID. 16 Our study aims to examine the association between maternal supplementation with FA and multivitamins before and/or during pregnancy and the risk of ASD in offspring.
A case-cohort study was established by linking health care registers from the Meuhedet health care organization that covers 35% of Israelis until the age of 15 years (eAppendix in the Supplement ). 17 Linked health care registers included the Family Relations Register, the Diagnostic Classification Register (records health care dates of diagnosis and codes in accordance with the International Classification of Diseases, Eighth Revision , and the International Classification of Diseases, Ninth Revision ), and the Prescription Register (records all prescribed and dispensed medications based on the Anatomical Therapeutic Chemical [ATC] Classification System).
We identified all children with ASD and a randomly selected one-third of all children born live between January 1, 2003, and December 31, 2007. The cohort was followed up from birth to January 26, 2015. All children had complete birth date, sex, and parental information. The study was approved by the University of Haifa Institutional Review Board and the Helsinki Ethics Committee of the Meuhedet. Each body that approved the study granted a waiver of informed consent because the study data were deidentified (eAppendix in the Supplement ).
Children with a clinical impression of probable ASD undergo evaluation by a panel of experts consisting of social workers, a psychologist, and either a trained psychiatrist, developmental behavioral pediatrician, or child neurologist. The final ASD diagnosis is determined by a board-recognized developmental behavioral pediatrician. Since 1995, diagnoses of ASD are stored in a database maintained by Meuhedet as a distinct subset of the Diagnostic Classification Register. We defined ASD using the International Classification of Diseases, Ninth Revision code 299.0, 299.1, or 299.8. Intellectual disability is diagnosed in a similar manner as ASD, except that the evaluation also includes psychometric cognitive testing (diagnostic codes are in the eAppendix in the Supplement ).
Information was obtained about sex, birth year, socioeconomic status (high vs low), 17 a maternal and paternal psychiatric diagnosis by childbirth (present or absent), maternal and paternal age at childbirth, and parity. 18 Parental psychiatric history was ascertained from a recorded diagnosis of at least 1 episode of a psychiatric disorder (eAppendix in the Supplement ).
The Meuhedet Prescription Register holds information on drugs dispensed by a majority of pharmacies nationwide since 1996, including drug names, prescription and dispensation dates, number of pills dispensed, and ATC codes. Using the ATC codes of dispensed drugs, we extracted information on dispensed FA and multivitamin supplements (eAppendix in the Supplement ). In Israel, food is not fortified with FA, but FA supplementation is recommended before and during pregnancy. 19
Using the ATC codes, vitamin supplements were classified as FA and/or multivitamin supplements, an FA supplement, and a multivitamin supplement. For each of the 3 vitamin supplement classifications, the redeemed dispensations were categorized into the following 2 time intervals: before pregnancy (540-271 days before childbirth) and during pregnancy (270 days before childbirth up to the date of childbirth).
For each dispensation, assuming 1 pill per day, we defined an exposure period as the date the pills were dispensed until the date the pills would be finished. If an exposure period occurred entirely during a defined time interval, we defined the woman as being exposed during that time interval.
Relative risks (RRs) of ASD and the associated 2-sided 95% CIs were estimated by the hazard ratios from Cox proportional hazards regression models. All models were fitted using age as the underlying time scale. For each exposure, a crude model was fitted without adjusting for any other covariate than the exposure. Each model was also adjusted with all the aforementioned covariates. Because we used a case-cohort study design, all models were estimated using sampling weights to correct for the sampling of controls. 20 As a consequence, if not adjusted for properly, the SEs may be underestimated, resulting in CIs that are too narrow; to correct for this, we used robust SEs. 21 The use of robust SEs also adjusted for the potential within-maternal correlations due to multiple births from the same mother. Each child was followed up from birth until the first diagnosis of ASD, death, or end of follow-up in 2015, whichever came first. The RRs of ASD among children whose mothers were exposed to FA and/or multivitamin supplements before and/or during pregnancy were compared with the reference group of children whose mothers had no exposure in each corresponding interval. Folic acid and/or multivitamin exposure, FA exposure, and multivitamin exposure were analyzed separately. P < .05 (2-sided) was considered statistically significant. All analyses were performed in R, version 3.4.1, 22 using the survival library. 23
The robustness of the primary results was tested in sensitivity analyses. First, we examined maternal vitamin supplementation before but not during pregnancy, during but not before pregnancy, and before and during pregnancy, and compared the group in each time interval with the reference group without maternal vitamin supplementation in each of the aforementioned intervals.
Second, we examined maternal vitamin supplementation with exposure before pregnancy compared with exposure during pregnancy. Third, we examined the exposure interval of 4 weeks before pregnancy to 8 weeks into pregnancy, compared with the reference group of children with no exposure in this interval for direct comparison with prior studies that have examined this exposure interval. 11 , 14 , 15 Fourth, we examined maternal vitamin supplementation 2 years before pregnancy, during pregnancy, and 2 years before and during pregnancy, compared with the reference group without vitamin supplementation in each of the aforementioned intervals. We examined the 2 years before pregnancy because vitamin use in this time interval has not been studied previously, to our knowledge, and is a negative control group. 24
Several potential sources of confounding factors were examined. First, we repeated the primary analysis among singleton births because associations between multiple births with vitamin exposure before conception 25 and assisted reproductive technologies 26 have been reported. Second, we repeated the primary analysis for male and female offspring separately. 27 Third, to investigate the role of maternal vitamin deficiency, we repeated the primary analysis for the offspring of women with and without a diagnosis of vitamin deficiency separately (eAppendix in the Supplement ). 2 , 28 Fourth, we repeated the primary analysis for offspring with both parents diagnosed with a psychiatric disorder and then for offspring with neither parent diagnosed with a psychiatric disorder. Fifth, we refitted the primary analysis confined to mothers with low socioeconomic status because socioeconomic status has been shown to be associated with risk of ASD. 17 Sixth, we refitted the primary analysis for the outcome diagnosis of ASD with and then without ID. 16 Finally, the proportional hazards assumption for the Cox proportional hazards regression models was examined using Schoenfeld residuals. 23
Children born before 2003 were not included in the analysis owing to a lack of reliable information on maternal vitamin dispensation before 2002. We included children born from 2003 onward to ascertain maternal vitamin use up to 270 days before birth. Of 45 300 children born to 26 702 mothers, 572 (1.3%) received a diagnosis of ASD. The raw dispensation rate indicated that most dispensations occurred around the first trimester ( Figure 1 ). There were 11 917 children (26.3%) born to mothers exposed to FA and/or multivitamin supplements before pregnancy and 21 884 children (48.3%) born to mothers exposed to FA and/or multivitamin supplements during pregnancy (eTable 1 in the Supplement ).
The crude RR of ASD in children of mothers exposed to FA and/or multivitamin supplements before pregnancy compared with children of unexposed mothers in the same interval was estimated at 0.41 (95% CI, 0.32-0.53) and at 0.39 (95% CI, 0.30-0.50) after covariate adjustment ( Figure 2 ). The crude RR of ASD in children of mothers exposed during pregnancy to FA and/or multivitamin supplements compared with children of unexposed mothers in the same interval was estimated at 0.27 (95% CI, 0.22-0.34) and at 0.27 (95% CI, 0.22-0.33) after covariate adjustment ( Figure 2 ).
The crude RR of ASD in children of mothers exposed before pregnancy to FA compared with children of unexposed mothers in the same interval was estimated at 0.62 (95% CI, 0.47-0.83) and at 0.56 (95% CI, 0.42-0.74) after covariate adjustment ( Figure 2 ). The crude RR of ASD in children of mothers exposed during pregnancy to FA compared with children of unexposed mothers in the same interval was estimated at 0.34 (95% CI, 0.27-0.43) and at 0.32 (95% CI, 0.26-0.41) after covariate adjustment ( Figure 2 ).
The crude RR of ASD in children of mothers exposed before pregnancy to multivitamin supplements compared with children of unexposed mothers in the same interval was estimated at 0.34 (95% CI, 0.23-0.49) and at 0.36 (95% CI, 0.24-0.52) after covariate adjustment ( Figure 2 ). The crude RR of ASD in children of mothers exposed during pregnancy to multivitamin supplements compared with children of unexposed mothers in the same interval was estimated at 0.36 (95% CI, 0.29-0.45) and at 0.35 (95% CI, 0.28-0.44) after covariate adjustment ( Figure 2 ).
Sensitivity analysis showed that exposure during compared with before pregnancy showed statistically insignificant risk reductions for FA and/or multivitamin exposure and FA exposure, but showed an insignificant increase in risk for multivitamin exposure ( Table , model 2). Maternal exposure to FA and/or multivitamin supplements from 4 weeks before to 8 weeks into pregnancy was associated with a statistically significant reduction in the risk of ASD in offspring compared with offspring of mothers with no exposure in that time interval ( Table , model 3). Across the vitamin supplement classifications examined, maternal exposure during the 2 years before pregnancy was associated with a significant reduction in the risk of ASD in offspring compared with the reference group never exposed, not exposed during the 2-year period before pregnancy, or not exposed during pregnancy (model 4 in the Table ; eTables 2 and 3 in the Supplement ).
Sensitivity analyses of possible sources of confounding replicated the statistical significance in the primary analysis ( Table ), with some exceptions. Among female offspring, maternal exposure to multivitamin supplementation before pregnancy (crude RR [eTable 3 in the Supplement ] and adjusted RR [ Table ]) and FA supplementation before pregnancy (crude RR [eTable 3 in the Supplement , model 7]) had a null association with the risk of ASD in offspring. Among offspring to both parents with a psychiatric condition, maternal exposure to FA before pregnancy had a null association with the risk of ASD in offspring ( Table , model 9). Among children of mothers with a vitamin deficiency, across the classifications of vitamin supplements examined, maternal exposure before pregnancy had a null association with the risk of ASD in offspring ( Table , model 11). Across the vitamin supplement classifications examined, maternal exposure before pregnancy was not statistically significantly associated with the risk of a comorbid diagnosis of ASD with ID in offspring ( Table , model 13). Inspection of the Schoenfeld residuals did not suggest any violation of the proportional hazards assumption for the primary exposures (eFigures 1-3 in the Supplement ).
This study of 45 300 children revealed a decreased risk of ASD in children born to mothers who used FA and/or multivitamin supplements before and/or during pregnancy compared with those who had not. Sensitivity analysis examining the risk in different intervals, controlling for different sources of confounding, and checking analytic assumptions underlying the statistical analysis did not generally attenuate the observed risk reduction. The association between the use of multivitamin supplements and the risk of ASD was similar in male and female offspring. However, the analysis for female offspring had low power due to the small sample size. Also, among offspring whose parents had a psychiatric condition, FA supplementation before pregnancy did not significantly reduce the risk of ASD. This finding may reflect noncompliance, higher rates of vitamin deficiency, or poor diet among persons with psychiatric conditions. 29 - 31 Across the vitamin supplement classes examined, maternal exposure before pregnancy did not reduce the risk of ASD with ID in offspring, possibly owing to the combination of rare outcome and rare exposure.
We examined whether the reduced RR of ASD was due to a vitamin deficiency. Folate deficiency before pregnancy has been associated with adverse childhood outcomes 32 and ASD traits. 33 , 34 The reduction in the risk of ASD in offspring after maternal exposure to FA and multivitamin supplements remained after adjusting for the presence of vitamin deficiency in the mother. However, among offspring of women with a vitamin deficiency who were already receiving supplementation before pregnancy, the risk of ASD was not reduced ( Table ), a result that rules out the possibility that the association is solely due to confounding. Future studies of the underlying biological mechanisms could help us understand the potential modifiable mechanisms in the possible causes of ASD.
Maternal FA and/or multivitamin supplement exposure before and during pregnancy reduced the risk of ASD in offspring. Our results are consistent with those from a Norwegian birth cohort study showing that maternal FA use from 4 weeks before and 8 weeks into pregnancy is associated with a reduced risk of ASD in offspring. 11 This interval is considered relevant to the development of the central nervous system, includes neural tube closure, and is implicated in the development of basic brain structures. These results were, however, not replicated in Danish studies on maternal use of FA and multivitamin supplements. 14 , 15 Unique to our study, to our knowledge, is the ability to examine the association between multivitamin exposure and ASD for an extended period preceding pregnancy. Maternal exposure to FA and multivitamin supplements 2 years before pregnancy was associated with a reduced risk of ASD in offspring ( Table , model 4). The risk of ASD associated with maternal vitamin exposure was similar before and during pregnancy ( Table , model 2). Our study could not determine whether this result is due to the vitamin or to unmeasured confounding by other conditions, such as preterm birth, or lifestyle factors. 35 Future research is warranted to examine the association between vitamin exposure before pregnancy and outcomes in offspring further.
The present results require cautious interpretation given several limitations. The effect of confounding was notable, and we cannot rule out remaining residual confounding. Furthermore, our study had a limited sample size and lacked the ability to conduct a sibling control analysis. 36 The underlying indication for the supplement dispensation is unknown. We cannot rule out the possibility that the observed risk reduction is due to other causes associated with the dispensation. However, most dispensations appeared to occur around pregnancy ( Figure 1 ).
Misclassifications of exposure may have occurred and biased the estimated risk reduction. Some mothers may have used over-the-counter supplements that were not prescribed by the health care professional (ie, use of the supplements was not recorded). This form of misclassification is in the direction of false negatives. False-negative classification of exposure may narrow the difference between the exposed and unexposed groups, resulting in a more conservative comparison than one without false-negative misclassification. This suggests that if women classified as false negative were accurately identified, the results would be more pronounced than they are.
Although registry data avoid recall biases associated with survey-based methods, 12 , 15 , 16 they still may be subject to bias, such as false-positive misclassification due to noncompliance. To address this limitation, the analysis consisted of continuous exposure over time. A continuous rather than a single dispensation pattern may reflect a conservative estimate of ongoing vitamin supplement use.
The rates of vitamin supplementation in our study largely resemble those found in prior registry-based research in Norway. 37 The prevalence of mutually exclusive FA and/or multivitamin supplements (derived from eTable 2: model 1 in the Supplement ) was 26 668 (58.8%) overall (vs 44.4% in the study in Norway), was 7133 (15.8%) before and during pregnancy (vs 15.9% in the study in Norway), was 14 751 (32.6%) during pregnancy only (vs 27.3% in the study in Norway), and was 4784 (10.6%) before pregnancy only (vs 1.3% in the study in Norway). 37 Differences may be attributable in part to government guidelines in Norway for FA supplement use for the first 12 weeks of pregnancy.
The extent to which dispensed vitamins are consumed is unknown, and ATC codes cannot distinguish between multivitamin preparations with and multivitamin preparations without FA. 38 Also, we lack information about the mothers’ whole-blood folate levels, which, to our knowledge, 17 is unavailable for women of reproductive age in Israel. Research has shown that second-trimester prenatal vitamin use and maternal whole-blood folate levels are not associated with a proxy of autism-like behaviors. 34 The lack of association between whole-blood folate levels and autistic behaviors may reflect the timing of biomarker measures relative to developmental periods, confounding, or other moderators. Although our exposure rates resembled those in prior studies, future research should account for whole-blood folate levels during pregnancy.
The combination of rare outcome and rare exposure (eTable 2 in the Supplement ) precluded defining adequately powered exposures by mutually exclusive time intervals across all analyses. This may be expected in observational studies like ours. Still, mutually exclusive exposure by time interval was included in the sensitivity analysis ( Table , model 1).
Another study limitation was our lack of information on gestational age, decreasing the accuracy of exposure classifications. The use of birth date to ascertain exposure increases the possibility that preterm births were misclassified. 39 Hence, future studies are warranted to replicate these findings.
Finally, causality cannot be inferred from observational epidemiologic studies such as this one. However, observational epidemiologic studies are more pragmatic and ethical than randomized clinical trials to examine the pregnancy period. 40
Maternal exposure to FA and multivitamin supplements before and during pregnancy is associated with a reduced risk of ASD in offspring compared with offspring of mothers without such exposure. Reduced risk of ASD in offspring is a consideration for public health policy that may be realized by extended use of FA and multivitamin supplements during pregnancy.
Accepted for Publication: November 4, 2017.
Corresponding Author: Stephen Z. Levine, PhD, Department of Community Mental Health, University of Haifa, Haifa, 31905, Israel ( [email protected] ).
Published Online: January 3, 2018. doi:10.1001/jamapsychiatry.2017.4050
Author Contributions: Drs Levine and Sandin had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Study concept and design: Levine, Viktorin, Uher, Reichenberg, Sandin.
Acquisition, analysis, or interpretation of data: Levine, Kodesh, Viktorin, Smith, Reichenberg, Sandin.
Drafting of the manuscript: Levine, Kodesh, Sandin.
Critical revision of the manuscript for important intellectual content: Levine, Viktorin, Smith, Uher, Reichenberg, Sandin.
Statistical analysis: Levine, Viktorin, Uher, Sandin.
Obtained funding: Reichenberg.
Administrative, technical, or material support: Levine, Kodesh, Viktorin, Smith, Reichenberg.
Study supervision: Levine, Reichenberg, Sandin.
Conflict of Interest Disclosures: In unrelated work Dr Levine reported receiving research support from Shire Pharmaceuticals. Arad Kodesh reported being an employee of Meuhedet Health Services. No other disclosures were reported.
Funding/Support: This study was supported by grants from the National Institutes of Health; grant HD073978 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institute of Environmental Health Sciences, and National Institute of Neurological Disorders and Stroke; grant MH097849 from the National Institute of Mental Health; by the Beatrice and Samuel A. Seaver Foundation (Dr Sandin is a Seaver Fellow); by the Fredrik and Ingrid Thuring Foundation; and by the Swedish Society of Medicine.
Role of the Funder/Sponsor: The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
- Register for email alerts with links to free full-text articles
- Access PDFs of free articles
- Manage your interests
- Save searches and receive search alerts
Information
- Author Services
Initiatives
You are accessing a machine-readable page. In order to be human-readable, please install an RSS reader.
All articles published by MDPI are made immediately available worldwide under an open access license. No special permission is required to reuse all or part of the article published by MDPI, including figures and tables. For articles published under an open access Creative Common CC BY license, any part of the article may be reused without permission provided that the original article is clearly cited. For more information, please refer to https://www.mdpi.com/openaccess .
Feature papers represent the most advanced research with significant potential for high impact in the field. A Feature Paper should be a substantial original Article that involves several techniques or approaches, provides an outlook for future research directions and describes possible research applications.
Feature papers are submitted upon individual invitation or recommendation by the scientific editors and must receive positive feedback from the reviewers.
Editor’s Choice articles are based on recommendations by the scientific editors of MDPI journals from around the world. Editors select a small number of articles recently published in the journal that they believe will be particularly interesting to readers, or important in the respective research area. The aim is to provide a snapshot of some of the most exciting work published in the various research areas of the journal.
Original Submission Date Received: .
- Active Journals
- Find a Journal
- Proceedings Series
- For Authors
- For Reviewers
- For Editors
- For Librarians
- For Publishers
- For Societies
- For Conference Organizers
- Open Access Policy
- Institutional Open Access Program
- Special Issues Guidelines
- Editorial Process
- Research and Publication Ethics
- Article Processing Charges
- Testimonials
- Preprints.org
- SciProfiles
- Encyclopedia
Article Menu

- Subscribe SciFeed
- Recommended Articles
- Google Scholar
- on Google Scholar
- Table of Contents
Find support for a specific problem in the support section of our website.
Please let us know what you think of our products and services.
Visit our dedicated information section to learn more about MDPI.
JSmol Viewer
The impact of parental involvement on the educational development of students with autism spectrum disorder.

1. Introduction
2. methodology, 2.1. design, 2.2. sample, 2.3. data collection instrument.
- Having published scientific articles on the inclusion of students with educational needs in the education system.
- Being trained in the educational needs of students.
- Having actively participated in research projects related to attention to diversity.
- Having taught in subjects related to attention to diversity.
2.4. Data Collection Procedure
2.5. data analysis process, 3.1. participation in school meetings and activities.
“Personally, I often attend meetings convened by the school at least once every two weeks, as I am interested in knowing about updates and new proposals suggested both by other parents and by the school’s own teachers”. (INTERVIEW 04)
“Sometimes, it is not possible for me to attend the meetings that the school organises to discuss problems that arise or simply to find out about our child’s academic performance, mainly because my work prevents me from doing so. My work schedule changes a lot, and I try to organise it with my husband, but sometimes it is not possible”. (INTERVIEW 11)
As these results are strikingly similar to those of people with and without tertiary education, an analysis was carried out to see whether the breakdown of participation in school activities is associated with educational level, which may in turn influence flexibility in working hours, etc.
“Although I recognise the importance of all the activities organised by the school, I tend to be more involved in tutorials, as decisions are made that directly affect my child’s education and well-being”. (INTERVIEW 15)
“Family participation in the school council remains low, due to the fact that some families are unaware of its functioning and importance”. (INTERVIEW 18)
3.2. Support for Homework at Home
“I am quite active in that. I think it is an essential part of my role as a parent to help my son with his homework, especially because he has ASD. Whenever there are school activities at home, I make sure I am available to support him”. (INTERVIEW 07)
“I really wish I could do more. I work full time and often have to bring work home, which limits the time I can spend helping with homework. I understand the importance of this support, especially because my daughter has ASD and needs more personalised attention”. (INTERVIEW 31)
As in the previous category, it was found to be necessary to analyse whether parents’ educational level is associated with homework support.
“We use a lot of visual aids because I have noticed that they capture their attention and really help them understand the concepts better. We also set up a regular schedule which seems to help him feel more confident and we eliminate distractions such as mobiles”. (INTERVIEW 21)
“We introduced technology tools that he used at home into the classroom as well, and we saw a noticeable improvement in his concentration and participation. I think this alignment between home and school really helped create a more effective and comfortable learning environment for him”. (INTERVIEW 01)
3.3. Communication and Collaboration
“For me, email is direct and efficient. I can write down my questions or concerns and send them when I have time during the day. It also allows me to have a written record of all communications, which is useful for tracking progress and issues discussed”. (INTERVIEW 31)
“We have been members of the Seville Autism Association for ten years and we have found a lot of support in the meetings we have attended”. (INTERVIEW 22)
“We take our daughter to the Early Attention Centre where she receives therapy and they have given us many tools to work with our daughter at home”. (INTERVIEW 02)
3.4. Challenges and Suggestions
“Communication between school and families is crucial and often insufficient. We need to ensure that there is an open and effective line of communication so that parents feel part of the educational process”. (INTERVIEW 09)
“A big problem is the lack of resources in the school; there are simply not enough trained staff and materials adapted for it. This has led me to look for external solutions such as finding specialised educational materials that we can use at home”. (INTERVIEW 39)
“I consider it essential to invest more money in educational materials adapted for students with ASD. Nowadays there are insufficient resources in a school”. (INTERVIEW 02)
“There is a need for greater awareness of the particularities of a pupil with ASD in the classroom. Therefore, the creation of training and awareness plans would be a way to help these students”. (INTERVIEW 18)
4. Discussion
5. conclusions, 6. limitations, 7. future directions, author contributions, institutional review board statement, informed consent statement, data availability statement, conflicts of interest.
| Q | Questions |
|---|---|
| 1 | Demographic questions: gender, age, ownership of your child’s centre. |
| 2 | How often do you attend school meetings or activities at school? |
| 3 | How do you support your child with homework at home? |
| 4 | What strategies do you use to maintain or increase your child’s motivation to study? |
| 5 | How is the communication between you and the school regarding your child’s academic progress and special needs? |
| 6 | Are you part of any support groups for parents of children with ASD? |
| 7 | What are the main challenges you have faced in your child’s education? |
| 8 | How have your own experience and expectations influenced your involvement in your child’s education? |
| 9 | What improvements would you suggest to better support students with ASD and their families? |
| 10 | Finally, is there anything else you would like to share? |
- Gómez Zepeda, G.; Petreñas, C.; Sabando, D.; Puigdellívol, I. El papel del Maestro de Apoyo y Atención a la Diversidad (MAAD) desde una perspectiva comunitaria: Promoviendo el éxito educativo y la inclusión educativa para todos. Enseñanza Form. Profr. 2017 , 64 , 127–138. [ Google Scholar ]
- Escobar Delgado, G.R.; Tarazona Meza, A.K.; Romero Chávez, S.A.; Alcívar Murillo, G.S. Demandas de las Personas con Discapacidad y Potenciación de Estrategias Resilientes. Rev. Int. Investig. Gestión Informática Cienc. Soc. 2018 , 5 , 45–54. [ Google Scholar ]
- Málaga, I.; Blanco Lago, R.; Hedrera-Fernández, A.; Álvarez-Álvarez, N.; Oreña-Ansonera, V.A.; Baeza-Velasco, M. Prevalencia de los trastornos del espectro autista en niños en Estados Unidos, Europa y España: Coincidencias y discrepancias. Medicina 2019 , 79 (Suppl. S1), 4–9. [ Google Scholar ] [ PubMed ]
- White, S.W.; Mazefsky, C.A.; Dichter, G.S.; Chiu, P.H.; Richey, J.A.; Ollendick, T.H. Social-cognitive, physiological, and neural mechanisms underlying emotion regulation impairments: Understanding anxiety in autism spectrum disorder. Int. J. Dev. Neurosci. 2014 , 39 , 22–36. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Belaić, Z.G. Parental Involvement in Their Children’s Education. Ziv. I Škola 2021 , 67 , 95–114. [ Google Scholar ] [ CrossRef ]
- Fan, X.; Chen, M. Parental Involvement and Students’ Academic Achievement: A Meta-Analysis. Educ. Psychol. Rev. 2001 , 13 , 1–22. [ Google Scholar ] [ CrossRef ]
- Ludlow, A.; Skelly, C.; Rohleder, P. Challenges faced by parents of children diagnosed with autism spectrum disorder. J. Health Psychol. 2012 , 17 , 702–711. [ Google Scholar ] [ CrossRef ]
- Campilla, J.; Guzman, J.; Santiago, C.; Rigor, J.; Frando, M. Challenges and Coping Strategies of Parents in the Education of their Children with Autism. E-DAWA Int. Multidiscip. Res. J. 2023 , 3 , 2. [ Google Scholar ] [ CrossRef ]
- Omar, T.; Ahmed, W.; Basiouny, N. Challenges and adjustments of mothers having children with autism. Alex. J. Pediatr. 2017 , 30 , 120–129. [ Google Scholar ] [ CrossRef ]
- Laili, N.; Abdullah, W.; Toran, H.; Amin, A.; Alias, R. Challenges and Support for Parents of Children with Autism Spectrum Disorder at Work. Int. J. Acad. Res. Bus. Soc. Sci. 2021 , 11 , 655–669. [ Google Scholar ] [ CrossRef ]
- Gona, J.; Newton, C.; Rimba, K.; Mapenzi, R.; Kihara, M.; Vijver, F.; Abubakar, A. Challenges and coping strategies of parents of children with autism on the Kenyan coast. Rural Remote Health 2016 , 16 , 3517. [ Google Scholar ] [ CrossRef ]
- Zablotsky, B.; Boswell, K.; Smith, C. An evaluation of school involvement and satisfaction of parents of children with autism spectrum disorders. Am. J. Intellect. Dev. Disabil. 2012 , 117 4 , 316–330. [ Google Scholar ] [ CrossRef ]
- Đorđević, M.; Glumbić, N.; Memisevic, H.; Brojčin, B.; Krstov, A. Parent-teacher interactions, family stress, well-being, and parental depression as contributing factors to parental involvement mechanisms in education of children with autism. Int. J. Dev. Disabil. 2021 , 68 , 838–849. [ Google Scholar ] [ CrossRef ]
- Álvarez-Gayou, J.L. Cómo Hacer Investigación Cualitativa. Fundamentos y Metodología ; Paidós: Barcelona, Spain, 2003. [ Google Scholar ]
- Fernández Batanero, J.M.; Tadeu, P.; Cabero, J. ICT and disability. Design, construction and validation of a diagnostic tool. J. Soc. Stud. Educ. Res. 2018 , 9 , 332–350. [ Google Scholar ] [ CrossRef ]
- Cruz Ramirez, M.; Martínez Cepena, M. Origin and development of an index of expert competence: The k coefficient. Rev. Latinoam. Metodol. Investig. Soc. 2020 , 19 , 40–56. [ Google Scholar ]
- WMA. World medical association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013 , 310 , 2191–2194. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Hill, N.; Taylor, L. Parental School Involvement and Children’s Academic Achievement. Curr. Dir. Psychol. Sci. 2004 , 13 , 161–164. [ Google Scholar ] [ CrossRef ]
- Schultz, T.; Able, H.; Sreckovic, M.; White, T. Parent-Teacher Collaboration: Teacher Perceptions of What Is Needed to Support Students with ASD in the Inclusive Classroom. Educ. Train. Autism Dev. Disabil. 2016 , 51 , 344–354. [ Google Scholar ]
- Yan, T.; Hou, Y.; Deng, M. Direct, Indirect, and Buffering Effect of Social Support on Parental Involvement Among Chinese Parents of Children with Autism Spectrum Disorders. J. Autism Dev. Disord. 2021 , 52 , 2911–2923. [ Google Scholar ] [ CrossRef ]
- Knight, V.F.; Mckissick, B.R.; Saunders, A.F. A Review of Technology-Based Interventions to Teach Academic Skills to Students with Autism Spectrum Disorder. J. Autism Dev. Disord. 2013 , 43 , 2628–2648. [ Google Scholar ] [ CrossRef ]
- Matson, J.L.; Boisjoli, J.A. Restraint procedures and challenging behaviours in intellectual disability: An analysis of causative factors. J. Appl. Res. Intellect. Disabil. 2009 , 22 , 111–117. [ Google Scholar ] [ CrossRef ]
- Grynszpan, O.; Weiss, P.L.; Perez-Diaz, F.; Gal, E. Innovative technology-based interventions for autism spectrum disorders: A meta-analysis. Autism 2014 , 18 , 346–361. [ Google Scholar ] [ CrossRef ] [ PubMed ]
- Morrier, M.J.; Hess, K.L.; Heflin, L.J. Teacher training for implementation of teaching strategies for students with autism spectrum disorders. Teach. Educ. Spec. Educ. 2011 , 34 , 119–132. [ Google Scholar ] [ CrossRef ]
- Stoner, J.B.; Angell, M.E.; House, J.J.; Bock, S.J. Individualized education programs for students with autism: Perceptions of parents and teachers. Focus Autism Other Dev. Disabil. 2005 , 20 , 24–33. [ Google Scholar ]
- Robertson, K.; Chamberlain, B.; Kasari, C. General education teachers’ relationships with included students with autism. J. Autism Dev. Disord. 2010 , 33 , 123–130. [ Google Scholar ] [ CrossRef ]
- Phelps, K.W.; Hodgson, J.L.; McCammon, S.L.; Lamson, A.L. Caring for an individual with autism spectrum disorder: A qualitative analysis. J. Intellect. Dev. Disabil. 2009 , 34 , 27–35. [ Google Scholar ] [ CrossRef ]
- Azad, G.F.; Mandell, D.S. Parent involvement in ASD intervention: An overview of the literature. J. Autism Dev. Disord. 2016 , 46 , 3573–3586. [ Google Scholar ]
- Barnard, W. Parent involvement in elementary school and educational attainment. Child. Youth Serv. Rev. 2004 , 26 , 39–62. [ Google Scholar ] [ CrossRef ]
- Montenegro Rueda, M.; Fernandez Batanero, J.M. Adaptation and validation of an instrument for assessing the digital competence of special education teachers. Eur. J. Spec. Needs Educ. 2023 , 39 , 367–382. [ Google Scholar ] [ CrossRef ]
Click here to enlarge figure
| Category | Subcategory | Values | |
|---|---|---|---|
| Male | N | 20 | |
| % | 47.6% | ||
| Female | N | 22 | |
| % | 52.3% | ||
| | Public | N | 17 |
| % | 40.4% | ||
| Private-Concerted | N | 14 | |
| % | 33.3% | ||
| Private | N | 11 | |
| % | 26.1% | ||
| Between 30 and 40 | N | 13 | |
| % | 30.9% | ||
| Between 40 and 50 | N | 23 | |
| % | 54.76% | ||
| More than 60 | N | 6 | |
| % | 14.34% | ||
| No higher education | N | 13 | |
| % | 30.95% | ||
| Higher education | N | 29 | |
| % | 69.05% | ||
| Categories | Subcategories | Description |
|---|---|---|
| Frequency | Frequency with which parents attend school meetings and activities. | |
| Type of activities | Types of school meetings and activities attended by parents. | |
| Frequency | How often do you help with your child’s chores at home? | |
| Support strategies and resources used at home | Specific strategies used to maintain or increase children’s motivation to study. | |
| Channels of communication | Means by which communication takes place (e-mail, meetings, reports, etc.). | |
| Participation in support groups | Participation in support groups or associations for parents of children with ASD. | |
| Main challenges | Specific challenges parents have faced in the education of their children. | |
| Strategies or suggestions for overcoming challenges | Strategies and solutions that parents have implemented or suggest implementing to address these challenges. |
| Overall Results of the Study | Breakdown of Participation | ||
|---|---|---|---|
| Attendance | 71.43% (n = 30) | No tertiary education | 11.9% (n = 5) |
| With higher education | 59.52% (n = 25) | ||
| Non-attendance | 28.57% (n = 12) | No tertiary education | 19.05% (n = 8) |
| With higher education | 9.52% (n = 4) | ||
| Overall Results of the Study | Breakdown of Participation | ||
|---|---|---|---|
| Attendance | 85.71% (n = 36) | No tertiary education | 19.05% (n = 8) |
| With higher education | 66.67% (n = 28) | ||
| Non-attendance | 14.29% (n = 6) | No tertiary education | 11.9% (n = 5) |
| With higher education | 2.38% (n = 1) | ||
| The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
Share and Cite
Fernández Cerero, J.; Montenegro Rueda, M.; López Meneses, E. The Impact of Parental Involvement on the Educational Development of Students with Autism Spectrum Disorder. Children 2024 , 11 , 1062. https://doi.org/10.3390/children11091062
Fernández Cerero J, Montenegro Rueda M, López Meneses E. The Impact of Parental Involvement on the Educational Development of Students with Autism Spectrum Disorder. Children . 2024; 11(9):1062. https://doi.org/10.3390/children11091062
Fernández Cerero, José, Marta Montenegro Rueda, and Eloy López Meneses. 2024. "The Impact of Parental Involvement on the Educational Development of Students with Autism Spectrum Disorder" Children 11, no. 9: 1062. https://doi.org/10.3390/children11091062
Article Metrics
Article access statistics, further information, mdpi initiatives, follow mdpi.
Subscribe to receive issue release notifications and newsletters from MDPI journals
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Review Article
- Published: 29 August 2024
Executive function deficits in attention-deficit/hyperactivity disorder and autism spectrum disorder
- Michael J. Kofler ORCID: orcid.org/0000-0002-8604-3647 1 ,
- Elia F. Soto ORCID: orcid.org/0000-0002-6672-287X 2 ,
- Leah J. Singh ORCID: orcid.org/0000-0003-0242-2859 1 ,
- Sherelle L. Harmon ORCID: orcid.org/0000-0002-7727-6908 1 ,
- Emma M. Jaisle ORCID: orcid.org/0000-0003-4882-7501 3 ,
- Jessica N. Smith ORCID: orcid.org/0000-0002-3559-4895 3 ,
- Kathleen E. Feeney ORCID: orcid.org/0000-0002-8442-7866 3 &
- Erica D. Musser 4
Nature Reviews Psychology ( 2024 ) Cite this article
3 Altmetric
Metrics details
- Autism spectrum disorders
- Signs and symptoms
Executive function deficits have been reported in both autism spectrum disorder (ASD) and attention-deficit/hyperactivity disorder (ADHD). However, little is known regarding which, if any, of these impairments are shared in children with ADHD and those with ASD. In this Review, we provide an overview of the current literature with a critical eye toward diagnostic, measurement and third-variable considerations that should be leveraged to provide more definitive answers. We conclude that the field’s understanding of executive function profiles in ASD and ADHD is highly limited because most research on each of these disorders has failed to account for the possible co-occurrence and the presence of symptoms of the other disorder. A vast majority of studies have relied on traditional neuropsychological tests and informant-rated executive function scales that have poor specificity and construct validity, and most studies have been unable to account for the well-documented between-person heterogeneity within and across disorders. At present, the most parsimonious conclusion is that children with ADHD and/or ASD tend to perform moderately worse than neurotypical children on a broad range of neuropsychological tests. However, the extent to which these difficulties are unique to one of these disorders or shared, or are attributable to impairments in specific executive functions, remains largely unknown. We end with focused recommendations for future research.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$59.00 per year
only $4.92 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
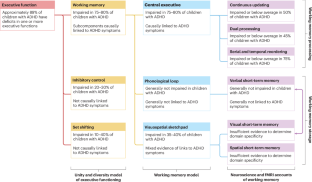
Similar content being viewed by others

Attention-deficit/hyperactivity disorder

Symptoms of autism in Williams syndrome: a transdiagnostic approach

Attention-deficit hyperactivity disorder traits are a more important predictor of internalising problems than autistic traits
American Psychiatric Association Diagnostic and Statistical Manual of Mental Disorders 5th edn (American Psychiatric Association, 2022).
Polanczyk, G., de Lima, M. S., Horta, B. L., Biederman, J. & Rohde, L. A. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am. J. Psychiat. 164 , 942–948 (2007).
Article PubMed Google Scholar
Polanczyk, G. V., Willcutt, E. G., Salum, G. A., Kieling, C. & Rohde, L. A. ADHD prevalence estimates across three decades: an updated systematic review and meta-regression analysis. Int. J. Epidemiol. 43 , 434–442 (2014).
Article PubMed PubMed Central Google Scholar
Boyle, C. A. et al. Trends in the prevalence of developmental disabilities in US children, 1997–2008. Pediatrics 127 , 1034–1042 (2011).
Kogan, M. D. et al. Prevalence of parent-reported diagnosis of autism spectrum disorder among children in the US, 2007. Pediatrics 124 , 1395–1403 (2009).
Federico, A. et al. Predictors of autism spectrum disorder and ADHD: results from the national survey of children’s health. Disabil. Health J. 17 , 101512 (2023).
Aduen, P. A. et al. Social problems in ADHD: is it a skills acquisition or performance problem? J. Psychopathol. Behav. Assess. 40 , 440–451 (2018).
Kofler, M. J. et al. Neurocognitive and behavioral predictors of social problems in ADHD: a Bayesian framework. Neuropsychology 32 , 344–355 (2018).
Ros, R. & Graziano, P. A. Social functioning in children with or at risk for attention deficit/hyperactivity disorder: a meta-analytic review. J. Clin. Child. Adolesc. Psychol. 47 , 213–235 (2018).
Pedreño, C., Pousa, E., Navarro, J., Pàmias, M. & Obiols, J. Exploring the components of advanced theory of mind in autism spectrum disorder. J. Autism Dev. Disord. 47 , 2401–2409 (2017).
Grzadzinski, R., Dick, C., Lord, C. & Bishop, S. Parent-reported and clinician-observed autism spectrum disorder (ASD) symptoms in children with attention deficit/hyperactivity disorder (ADHD): implications for practice under DSM-5. Molec. Autism 7 , 7 (2016).
Article Google Scholar
Locke, J., Shih, W., Kretzmann, M. & Kasari, C. Examining playground engagement between elementary school children with and without autism spectrum disorder. Autism 20 , 653–662 (2016).
Gates, J. A., McNair, M. L., Richards, J. K. & Lerner, M. D. Social knowledge & performance in autism: a critical review & recommendations. Clin. Child. Fam. Psychol. Rev. 26 , 665–689 (2023).
Demetriou, E. A., DeMayo, M. M. & Guastella, A. J. Executive function in autism spectrum disorder: history, theoretical models, empirical findings, and potential as an endophenotype. Front. Psychiat. 10 , 753 (2019).
Kofler, M. J. et al. Reaction time variability in ADHD: a meta-analytic review of 319 studies. Clin. Psychol. Rev. 33 , 795–811 (2013).
Nigg, J. T. Annual research review: on the relations among self-regulation, self-control, executive functioning, effortful control, cognitive control, impulsivity, risk-taking, and inhibition for developmental psychopathology. J. Child. Psychol. Psychiat. 58 , 361–383 (2017).
Barrasso-Catanzaro, C. & Eslinger, P. J. Neurobiological bases of executive function and social-emotional development: typical and atypical brain changes. Fam. Relat. 65 , 108–119 (2016).
Diamond, A. Activities and programs that improve children’s executive functions. Curr. Dir. Psychol. Sci. 21 , 335–341 (2012).
Miyake, A. et al. The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: a latent variable analysis. Cogn. Psychol. 41 , 49–100 (2000).
Diamond, A. Executive functions. Annu. Rev. Psychol. 64 , 135–168 (2013).
Baddeley, A. Working memory: theories, models, and controversies. Annu. Rev. Psychol. 63 , 1–29 (2012).
Wiemers, E. A. & Redick, T. S. Working memory capacity and intra-individual variability of proactive control. Acta Psychol. 182 , 21–31 (2018).
Raiker, J. S., Rapport, M. D., Kofler, M. J. & Sarver, D. E. Objectively-measured impulsivity and attention-deficit/hyperactivity disorder (ADHD): testing competing predictions from the working memory and behavioral inhibition models of ADHD. J. Abnorm. Child. Psychol. 40 , 699–713 (2012).
Patros, C. H. et al. Visuospatial working memory underlies choice-impulsivity in boys with attention-deficit/hyperactivity disorder. Res. Dev. Disabil. 38 , 134–144 (2015).
Singh, L. J., Gaye, F., Cole, A. M., Chan, E. S. & Kofler, M. J. Central executive training for ADHD: effects on academic achievement, productivity, and success in the classroom. Neuropsychology 36 , 330–345 (2022).
Demaray, M. K. & Jenkins, L. N. Relations among academic enablers and academic achievement in children with and without high levels of parent-rated symptoms of inattention, impulsivity, and hyperactivity. Psychol. Sch. 48 , 573–586 (2011).
Barkley, R. A. Behavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHD. Psychol. Bull. 121 , 65–94 (1997).
Pennington, B. F. & Ozonoff, S. Executive functions and developmental psychopathology. J. Child. Psychol. Psychiat. 37 , 51–87 (1996).
Rapport, M. D., Chung, K.-M., Shore, G. & Isaacs, P. A conceptual model of child psychopathology: implications for understanding attention deficit hyperactivity disorder and treatment efficacy. J. Clin. Child. Adolesc. Psychol. 30 , 48–58 (2001).
Kofler, M. J., Raiker, J. S., Sarver, D. E., Wells, E. L. & Soto, E. F. Is hyperactivity ubiquitous in ADHD or dependent on environmental demands? Evidence from meta-analysis. Clin. Psychol. Rev. 46 , 12–24 (2016).
Kofler, M. J. et al. Working memory deficits and social problems in children with ADHD. J. Abnorm. Child. Psychol. 39 , 805–817 (2011).
Groves, N. B. et al. Executive functioning and emotion regulation in children with and without ADHD. Res. Child. Adolesc. Psychopathol. 50 , 721–735 (2021).
Kofler, M. J., Rapport, M. D., Bolden, J., Sarver, D. E. & Raiker, J. S. ADHD and working memory: the impact of central executive deficits and exceeding storage/rehearsal capacity on observed inattentive behavior. J. Abnorm. Child. Psychol. 38 , 149–161 (2010).
Hill, E. L. Evaluating the theory of executive dysfunction in autism. Dev. Rev. 24 , 189–233 (2004).
Leung, R. C., Vogan, V. M., Powell, T. L., Anagnostou, E. & Taylor, M. J. The role of executive functions in social impairment in autism spectrum disorder. Child. Neuropsychol. 22 , 336–344 (2016).
Mostert-Kerckhoffs, M. A., Staal, W. G., Houben, R. H. & de Jonge, M. V. Stop and change: inhibition and flexibility skills are related to repetitive behavior in children and young adults with autism spectrum disorders. J. Autism Dev. Disord. 45 , 3148–3158 (2015).
Ozonoff, S. in Learning and Cognition in Autism: Current Issues in Autism (eds Schopler, E. & Mesibov, G. B.) 199–219 (Springer, 1995).
Karr, J. E. et al. The unity and diversity of executive functions: a systematic review and re-analysis of latent variable studies. Psychol. Bull. 144 , 1147–1185 (2018).
Miyake, A. & Friedman, N. P. The nature and organization of individual differences in executive functions: four general conclusions. Curr. Dir. Psychol. Sci. 21 , 8–14 (2012).
Wiebe, S. A. et al. The structure of executive function in 3-year-olds. J. Exp. Child. Psychol. 108 , 436–452 (2011).
Zelazo, P. D., Craik, F. I. & Booth, L. Executive function across the life span. Acta Psychol. 115 , 167–183 (2004).
Lerner, M. D. & Lonigan, C. J. Executive function among preschool children: unitary versus distinct abilities. J. Psychopathol. Behav. Assess. 36 , 626–639 (2014).
St Clair-Thompson, H. L. & Gathercole, S. E. Executive functions and achievements in school: shifting, updating, inhibition, and working memory. Q. J. Exp. Psychol. 59 , 745–759 (2006).
Kofler, M. J. et al. Working memory and organizational skills problems in ADHD. J. Child. Psychol. Psychiat. 59 , 57–67 (2018).
Jaroslawska, A. J., Gathercole, S. E., Logie, M. R. & Holmes, J. Following instructions in a virtual school: does working memory play a role? Mem. Cogn. 44 , 580–589 (2016).
Engle, R. W. & Kane, M. J. in The Psychology of Learning and Motivation: Advances in Research and Theory Vol. 44 (ed. Ross, B. H.) 145–199 (Elsevier Science, 2004).
Chacko, A., Kofler, M. & Jarrett, M. Improving outcomes for youth with ADHD: a conceptual framework for combined neurocognitive and skill-based treatment approaches. Clin. Child. Fam. Psychol. Rev. 17 , 368–384 (2014).
Antshel, K. M. & Russo, N. Autism spectrum disorders and ADHD: overlapping phenomenology, diagnostic issues, and treatment considerations. Curr. Psychiat. Rep. 21 , 34 (2019).
Townes, P. et al. Do ASD and ADHD have distinct executive function deficits? A systematic review and meta-analysis of direct comparison studies. J. Atten. Disord. 27 , 1571–1582 (2023).
Sullivan, G. M. & Feinn, R. Using effect size — or why the P value is not enough. J. Grad. Med. Educ. 4 , 279–282 (2012).
Kofler, M. J. et al. Executive functioning heterogeneity in pediatric ADHD. J. Abnorm. Child. Psychol. 47 , 273–286 (2019).
Pievsky, M. A. & McGrath, R. E. The neurocognitive profile of attention-deficit/hyperactivity disorder: a review of meta-analyses. Arch. Clin. Neuropsychol. 33 , 143–157 (2018).
Kasper, L. J., Alderson, R. M. & Hudec, K. L. Moderators of working memory deficits in children with attention-deficit/hyperactivity disorder (ADHD): a meta-analytic review. Clin. Psychol. Rev. 32 , 605–617 (2012).
Fosco, W. D., Kofler, M. J., Groves, N. B., Chan, E. S. & Raiker, J. S. Which ‘working’components of working memory aren’t working in youth with ADHD? J. Abnorm. Child. Psychol. 48 , 647–660 (2020).
Wager, T. D. & Smith, E. E. Neuroimaging studies of working memory. Cogn. Affect. Behav. Neurosci. 3 , 255–274 (2003).
Kofler, M. J. et al. Working memory and short-term memory deficits in ADHD: a bifactor modeling approach. Neuropsychology 34 , 686–698 (2020).
Pauli-Pott, U. & Becker, K. Neuropsychological basic deficits in preschoolers at risk for ADHD: a meta-analysis. Clin. Psychol. Rev. 31 , 626–637 (2011).
Schoemaker, K., Mulder, H., Deković, M. & Matthys, W. Executive functions in preschool children with externalizing behavior problems: a meta-analysis. J. Abnorm. Child. Psychol. 41 , 457–471 (2013).
Demetriou, E. A. et al. Autism spectrum disorders: a meta-analysis of executive function. Mol. Psychiat. 23 , 1198–1204 (2018).
Habib, A., Harris, L., Pollick, F. & Melville, C. A meta-analysis of working memory in individuals with autism spectrum disorders. PLoS ONE 14 , e0216198 (2019).
Wang, Y. et al. A meta-analysis of working memory impairments in autism spectrum disorders. Neuropsychol. Rev. 27 , 46–61 (2017).
Edmunds, S. R., Colman, C., Vidal, P. & Faja, S. Brief report: examining the links between language processes and working memory impairments in toddlers and preschoolers with ASD. J. Autism Dev. Disord. 52 , 1872–1880 (2022).
Lai, C. L. E. et al. Meta-analysis of neuropsychological measures of executive functioning in children and adolescents with high-functioning autism spectrum disorder. Autism Res. 10 , 911–939 (2017).
Yerys, B. E. et al. Set-shifting in children with autism spectrum disorders: reversal shifting deficits on the Intradimensional/Extradimensional Shift Test correlate with repetitive behaviors. Autism 13 , 523–538 (2009).
Yerys, B. E. et al. Attention deficit/hyperactivity disorder symptoms moderate cognition and behavior in children with autism spectrum disorders. Autism Res. 2 , 322–333 (2009).
Karalunas, S. L. et al. Overlapping and distinct cognitive impairments in attention-deficit/hyperactivity and autism spectrum disorder without intellectual disability. J. Abnorm. Child. Psychol. 46 , 1705–1716 (2018).
Craig, F. et al. A review of executive function deficits in autism spectrum disorder and attention-deficit/hyperactivity disorder. Neuropsychiat. Dis. Treat . 12 , 1191–1202 (2016).
Google Scholar
Neely, R. J., Green, J. L., Sciberras, E., Hazell, P. & Anderson, V. Relationship between executive functioning and symptoms of attention-deficit/hyperactivity disorder and autism spectrum disorder in 6–8 year old children. J. Autism Dev. Disord. 46 , 3270–3280 (2016).
Sinzig, J., Morsch, D., Bruning, N., Schmidt, M. H. & Lehmkuhl, G. Inhibition, flexibility, working memory and planning in autism spectrum disorders with and without comorbid ADHD-symptoms. Child. Adolesc. Psychiat. Ment. Health 2 , 1–4 (2008).
Benallie, K. J., McClain, M. B., Bakner, K. E., Roanhorse, T. & Ha, J. Executive functioning in children with ASD + ADHD and ASD + ID: a systematic review. Res. Autism Spectr. Disord. 86 , 101807 (2021).
Carroll, A. G. Comparing Executive Functioning Impairments Across Clinical Groups: Autism Spectrum Disorder, Attention-Deficit/Hyperactivity Disorder, and Their Comorbid Occurrence in Children PhD thesis https://www.proquest.com/dissertations-theses/comparing-executive-functioning-impairments/docview/2594697995/se-2?accountid=15728 (Indiana Univ. Pennsylvania, 2022).
Alderson, R. M., Rapport, M. D., Sarver, D. E. & Kofler, M. J. ADHD and behavioral inhibition: a re-examination of the stop-signal task. J. Abnorm. Child. Psychol. 36 , 989–998 (2008).
Alderson, R. M., Rapport, M. D. & Kofler, M. J. Attention-deficit/hyperactivity disorder and behavioral inhibition: a meta-analytic review of the stop-signal paradigm. J. Abnorm. Child. Psychol. 35 , 745–758 (2007).
Wright, L., Lipszyc, J., Dupuis, A., Thayapararajah, S. W. & Schachar, R. Response inhibition and psychopathology: a meta-analysis of go/no-go task performance. J. Abnorm. Psychol. 123 , 429–439 (2014).
Lipszyc, J. & Schachar, R. Inhibitory control and psychopathology: a meta-analysis of studies using the stop signal task. J. Int. Neuropsychol. Soc. 16 , 1064–1076 (2010).
Lansbergen, M. M., Kenemans, J. L. & van Engeland, H. Stroop interference and attention-deficit/hyperactivity disorder: a review and meta-analysis. Neuropsychology 21 , 251–262 (2007).
Mullane, J. C., Corkum, P. V., Klein, R. M. & McLaughlin, E. Interference control in children with and without ADHD: a systematic review of Flanker and Simon task performance. Child. Neuropsychol. 15 , 321–342 (2009).
Geurts, H. M., van den Bergh, S. F. W. M. & Ruzzano, L. Prepotent response inhibition and interference control in autism spectrum disorders: two meta-analyses. Autism Res. 7 , 407–420 (2014).
Tonizzi, I., Giofrè, D. & Usai, M. C. Inhibitory control in autism spectrum disorders: meta-analyses on indirect and direct measures. J. Autism Dev. Disord. 52 , 4949–4965 (2022).
Irwin, L. N., Kofler, M. J., Soto, E. F. & Groves, N. B. Do children with attention-deficit/hyperactivity disorder (ADHD) have set shifting deficits? Neuropsychology 33 , 470–481 (2019).
Irwin, L. N., Groves, N. B., Soto, E. F. & Kofler, M. J. Is there a functional relation between set shifting and hyperactivity in children with attention-deficit/hyperactivity disorder (ADHD)? J. Int. Neuropsychol. Soc. 26 , 1019–1027 (2020).
Irwin Harper, L. N., Groves, N. B., Marsh, C. L., Cole, A. M. & Kofler, M. J. Does training working memory or inhibitory control produce far-transfer improvements in set shifting for children with ADHD? A randomized controlled trial. Child. Neuropsychol. 29 , 825–845 (2023).
Reed, P. Behavioural flexibility of children with autism spectrum disorder on a card-sorting task with varying task difficulty. Heliyon 4 , e00842 (2018).
Miller, H. L., Ragozzino, M. E., Cook, E. H., Sweeney, J. A. & Mosconi, M. W. Cognitive set shifting deficits and their relationship to repetitive behaviors in autism spectrum disorder. J. Autism Dev. Disord. 45 , 805–815 (2015).
Chen, S.-F. et al. Deficits in executive functions among youths with autism spectrum disorders: an age-stratified analysis. Psychol. Med. 46 , 1625–1638 (2016).
Boshomane, T. T., Pillay, B. J. & Meyer, A. Mental flexibility (set-shifting) deficits in children with ADHD: a replication and extension study. J. Psychol. Afr. 31 , 344–349 (2021).
Fair, D. A., Bathula, D., Nikolas, M. A. & Nigg, J. T. Distinct neuropsychological subgroups in typically developing youth inform heterogeneity in children with ADHD. Proc. Natl Acad. Sci. USA 109 , 6769–6774 (2012).
Dajani, D. R., Llabre, M. M., Nebel, M. B., Mostofsky, S. H. & Uddin, L. Q. Heterogeneity of executive functions among comorbid neurodevelopmental disorders. Sci. Rep. 6 , 36566 (2016).
Karalunas, S. L. et al. Heterogeneity in development of aspects of working memory predicts longitudinal attention deficit hyperactivity disorder symptom change. J. Abnorm. Psychol. 126 , 774–792 (2017).
Irwin, L. N. et al. Activities of daily living and working memory in pediatric attention-deficit/hyperactivity disorder (ADHD). Child. Neuropsychol. 27 , 468–490 (2021).
Korkman, M., Kirk, U. & Kemp, S. NEPSY II: Clinical and Interpretive Manual (Harcourt Assessment, PsychCorp, 2007).
Wechsler, D. Wechsler Intelligence Scale for Children 5th edn (WISC-V) ( Pearson, 2014).
Andersson, A. et al. Research review: the strength of the genetic overlap between ADHD and other psychiatric symptoms — a systematic review and meta-analysis. J. Child. Psychol. Psychiat. 61 , 1173–1183 (2020).
Yerys, B. E. et al. Evaluation of the ADHD rating scale in youth with autism. J. Autism Dev. Disord. 47 , 90–100 (2017).
Zhou, X., Reynolds, C., Zhu, J. & Kamphaus, R. W. Differentiating autism from ADHD in children and adolescents using BASC-3. J. Pediatr. Neuropsychol. 6 , 61–65 (2020).
Rosen, T. E., Mazefsky, C. A., Vasa, R. A. & Lerner, M. D. Co-occurring psychiatric conditions in autism spectrum disorder. Int. Rev. Psychiat. 30 , 40–61 (2018).
Mazefsky, C. A. et al. ASD, a psychiatric disorder, or both? Psychiatric diagnoses in adolescents with high-functioning ASD. J. Clin. Child. Adolesc. Psychol. 41 , 516–523 (2012).
Miodovnik, A., Harstad, E., Sideridis, G. & Huntington, N. Timing of the diagnosis of attention-deficit/hyperactivity disorder and autism spectrum disorder. Pediatrics 136 , e830–e837 (2015).
Katusic, M. Z., Myers, S. M., Weaver, A. L. & Voigt, R. G. IQ in autism spectrum disorder: a population-based birth cohort study. Pediatrics 148 , e2020049899 (2021).
Witwer, A. N. & Lecavalier, L. Validity of comorbid psychiatric disorders in youngsters with autism spectrum disorders. J. Dev. Phys. Disabil. 22 , 367–380 (2010).
Musser, E. D. et al. Shared familial transmission of autism spectrum and attention-deficit/hyperactivity disorders. J. Child. Psychol. Psychiat. 55 , 819–827 (2014).
Lerner, M. D. et al. Verbal ability and psychiatric symptoms in clinically referred inpatient and outpatient youth with ASD. J. Autism Dev. Disord. 48 , 3689–3701 (2018).
Engle, R. W., Tuholski, S. W., Laughlin, J. E. & Conway, A. R. Working memory, short-term memory, and general fluid intelligence: a latent-variable approach. J. Exp. Psychol. Gen. 128 , 309–331 (1999).
Giofrè, D., Mammarella, I. C. & Cornoldi, C. The structure of working memory and how it relates to intelligence in children. Intelligence 41 , 396–406 (2013).
Tourva, A., Spanoudis, G. & Demetriou, A. Cognitive correlates of developing intelligence: the contribution of working memory, processing speed and attention. Intelligence 54 , 136–146 (2016).
Lilienfeld, S. O. & Landfield, K. in P sychopathology: History, Diagnosis, and Empirical Foundations (eds Craighead, W. E., Miklowitz, D. J. & Craighead, L. W.) 1–33 (John Wiley & Sons, 2008).
Brown, T. A. & Barlow, D. H. A proposal for a dimensional classification system based on the shared features of the DSM-IV anxiety and mood disorders: implications for assessment and treatment. Psychol. Assess. 21 , 256–271 (2009).
Cuthbert, B. N. & Insel, T. R. Toward the future of psychiatric diagnosis: the seven pillars of RDoC. BMC Med. 11 , 126 (2013).
Sokolova, E. et al. A causal and mediation analysis of the comorbidity between attention deficit hyperactivity disorder (ADHD) and autism spectrum disorder (ASD). J. Autism Dev. Disord. 47 , 1595–1604 (2017).
Krakowski, A. D. et al. Characterizing the ASD–ADHD phenotype: measurement structure and invariance in a clinical sample. J. Child. Psychol. Psychiat. 63 , 1534–1543 (2022).
Anning, K. L., Langley, K., Hobson, C. & Van Goozen, S. H. M. Dimensional associations between executive function processes and symptoms of ADHD, ASD, oppositional defiance and anxiety in young school-referred children. Cortex 167 , 132–147 (2023).
Snyder, H. R., Miyake, A. & Hankin, B. L. Advancing understanding of executive function impairments and psychopathology: bridging the gap between clinical and cognitive approaches. Front. Psychol. 6 , 328 (2015).
Semrud-Clikeman, M. & Ellison, P. A. T. Child Neuropsychology (Springer, 2009).
Sattler, J. Assessment of Children: Cognitive Foundations and Applications and Resource Guide to Accompany Assessment of Children: Cognitive Foundations and Applications (Sattler, 2018).
Benson, N. F. et al. Test use and assessment practices of school psychologists in the United States: findings from the 2017 national survey. J. Sch. Psychol. 72 , 29–48 (2019).
Delis, D. C., Kaplan, E. & Kramer, J. H. Delis–Kaplan Executive Function System Assessment D-KEFS Database 10.1037/t15082-000 (APA PsycTests, 2001).
Woodcock, R. W., McGrew, K. S. & Mather, N. Woodcock–Johnson III Tests of Cognitive Abilities (Riverside Publishing, 2001).
Sonuga-Barke, E. J., Sergeant, J. A., Nigg, J. & Willcutt, E. Executive dysfunction and delay aversion in attention deficit hyperactivity disorder: nosologic and diagnostic implications. Child. Adolesc. Psychiat. Clin. N. Am. 17 , 367–384 (2008).
Canivez, G. L., Dombrowski, S. C. & Watkins, M. W. Factor structure of the WISC-V in four standardization age groups: exploratory and hierarchical factor analyses with the 16 primary and secondary subtests. Psychol. Sch. 55 , 741–769 (2018).
Floyd, R. G., Bergeron, R., Hamilton, G. & Parra, G. R. How do executive functions fit with the Cattell–Horn–Carroll model? Some evidence from a joint factor analysis of the Delis–Kaplan executive function system and the Woodcock–Johnson III tests of cognitive abilities. Psychol. Sch. 47 , 721–738 (2010).
Singh, L. J., Floyd, R. G., Reynolds, M. R., Pike, N. A. & Huenergarde, M. C. What does the developmental Neuropsychological Assessment–II (NEPSY-II) measure in children ages 7 to 12? A structural and psychometric analysis. Child Neuropsychol . https://doi.org/10.1080/09297049.2024.2357376 (2024).
Abad, F. J., Sorrel, M. A., Román, F. J. & Colom, R. The relationships between WAIS-IV factor index scores and educational level: a bifactor model approach. Psychol. Assess. 28 , 987 (2016).
Canivez, G. L. et al. Construct validity of the WISC-V in clinical cases: exploratory and confirmatory factor analyses of the 10 primary subtests. Assessment 27 , 274–296 (2020).
Canivez, G. L., Watkins, M. W. & Dombrowski, S. C. Factor structure of the Wechsler Intelligence Scale for Children — Fifth edition: exploratory factor analyses with the 16 primary and secondary subtests. Psychol. Assess. 28 , 975–986 (2016).
Dombrowski, S. C., Canivez, G. L. & Watkins, M. W. Factor structure of the 10 WISC-V primary subtests across four standardization age groups. Contemp. Sch. Psychol. 22 , 90–104 (2018).
Dombrowski, S. C., Canivez, G. L., Watkins, M. W. & Beaujean, A. A. Exploratory bifactor analysis of the Wechsler Intelligence Scale for Children — Fifth edition with the 16 primary and secondary subtests. Intelligence 53 , 194–201 (2015).
Gignac, G. E. & Watkins, M. W. Bifactor modeling and the estimation of model-based reliability in the WAIS-IV. Multivar. Behav. Res. 48 , 639–662 (2013).
Kranzler, J. H., Benson, N. & Floyd, R. G. Using estimated factor scores from a bifactor analysis to examine the unique effects of the latent variables measured by the WAIS-IV on academic achievement. Psychol. Assess. 27 , 1402–1416 (2015).
Watkins, M. W. et al. Long-term stability of Wechsler Intelligence Scale for Children — 5th edition scores in a clinical sample. Appl. Neuropsychol. Child. 11 , 422–428 (2022).
Wells, E. L., Kofler, M. J., Soto, E. F., Schaefer, H. S. & Sarver, D. E. Assessing working memory in children with ADHD: minor administration and scoring changes may improve digit span backward’s construct validity. Res. Dev. Disabil. 72 , 166–178 (2018).
Conway, A. R. et al. Working memory span tasks: a methodological review and user’s guide. Psychon. Bull. Rev. 12 , 769–786 (2005).
Soto, E. F. et al. Executive functioning rating scales: ecologically valid or construct invalid? Neuropsychology 34 , 605–619 (2020).
Rapport, M. D., Orban, S. A., Kofler, M. J. & Friedman, L. M. Do programs designed to train working memory, other executive functions, and attention benefit children with ADHD? A meta-analytic review of cognitive, academic, and behavioral outcomes. Clin. Psychol. Rev. 33 , 1237–1252 (2013).
Redick, T. S. & Lindsey, D. R. Complex span and n -back measures of working memory: a meta-analysis. Psychon. Bull. Rev. 20 , 1102–1113 (2013).
Isquith, P. K., Roth, R. M. & Gioia, G. Contribution of rating scales to the assessment of executive functions. Appl. Neuropsychol. Child. 2 , 125–132 (2013).
Toplak, M. E., West, R. F. & Stanovich, K. E. Practitioner review: do performance-based measures and ratings of executive function assess the same construct? J. Child. Psychol. Psychiat. 54 , 131–143 (2013).
Miranda, A., Colomer, C., Mercader, J., Fernández, M. I. & Presentación, M. J. Performance-based tests versus behavioral ratings in the assessment of executive functioning in preschoolers: associations with ADHD symptoms and reading achievement. Front. Psychol. 6 , 545 (2015).
Nordvall, O., Jonsson, B. & Neely, A. S. Self-reported and performance-based measures of executive functions in interned youth. Psychol. Crime. Law 23 , 240–253 (2017).
Spiegel, J. A., Lonigan, C. J. & Phillips, B. M. Factor structure and utility of the behavior rating inventory of executive function — preschool version. Psychol. Assess. 29 , 172–185 (2017).
Friedman, N. P. & Miyake, A. Unity and diversity of executive functions: individual differences as a window on cognitive structure. Cortex 86 , 186–204 (2017).
Biederman, J. et al. Impact of executive function deficits and attention-deficit/hyperactivity disorder (ADHD) on academic outcomes in children. J. Consult. Clin. Psychol. 72 , 757–766 (2004).
Coghill, D. R., Seth, S. & Matthews, K. A comprehensive assessment of memory, delay aversion, timing, inhibition, decision making and variability in attention deficit hyperactivity disorder: advancing beyond the three-pathway models. Psychol. Med. 44 , 1989–2001 (2014).
Nigg, J. T., Willcutt, E. G., Doyle, A. E. & Sonuga-Barke, E. J. S. Causal heterogeneity in attention-deficit/hyperactivity disorder: do we need neuropsychologically impaired subtypes? Biol. Psychiat. 57 , 1224–1230 (2005).
Willcutt, E. G., Doyle, A. E., Nigg, J. T., Faraone, S. V. & Pennington, B. F. Validity of the executive function theory of attention-deficit/hyperactivity disorder: a meta-analytic review. Biol. Psychiat. 57 , 1336–1346 (2005).
Solanto, M. V. et al. The ecological validity of delay aversion and response inhibition as measures of impulsivity in AD/HD: a supplement to the NIMH multimodal treatment study of AD/HD. J. Abnorm. Child. Psychol. 29 , 215–228 (2001).
Sonuga-Barke, E., Bitsakou, P. & Thompson, M. Beyond the dual pathway model: evidence for the dissociation of timing, inhibitory, and delay-related impairments in attention-deficit/hyperactivity disorder. J. Am. Acad. Child. Adolesc. Psychiat. 49 , 345–355 (2010).
Willoughby, M. T. & Blair, C. B. Measuring executive function in early childhood: a case for formative measurement. Psychol. Assess. 28 , 319 (2016).
Redick, T. S. et al. Measuring working memory capacity with automated complex span tasks. Eur. J. Psychol. Assess. 28 , 164–171 (2012).
Nee, D. E. et al. A meta-analysis of executive components of working memory. Cereb. Cortex 23 , 264–282 (2013).
Kofler, M. J. et al. Rethinking hyperactivity in pediatric ADHD: preliminary evidence for a reconceptualization of hyperactivity/impulsivity from the perspective of informant perceptual processes. Psychol. Assess. 32 , 752–767 (2020).
Hwang-Gu, S.-L. et al. Symptoms of ADHD affect intrasubject variability in youths with autism spectrum disorder: an ex-Gaussian analysis. J. Clin. Child. Adolesc. Psychol. 48 , 455–468 (2019).
Fosco, W. D. et al. Inhibitory control and information processing in ADHD: comparing the dual task and performance adjustment hypotheses. J. Abnorm. Child. Psychol. 47 , 961–974 (2019).
Kofler, M. J. et al. Working memory and intraindividual variability as neurocognitive indicators in ADHD: examining competing model predictions. Neuropsychology 28 , 459–471 (2014).
Rapport, M. D. et al. Working memory deficits in boys with attention-deficit/hyperactivity disorder (ADHD): the contribution of central executive and subsystem processes. J. Abnorm. Child. Psychol. 36 , 825–837 (2008).
Kofler, M. J. et al. A randomized controlled trial of central executive training (CET) versus inhibitory control training (ICT) for ADHD. J. Consult. Clin. Psychol. 88 , 738–756 (2020).
Chan, E. S. M., Gaye, F., Cole, A. M., Singh, L. J. & Kofler, M. J. Central executive training for ADHD: impact on organizational skills at home and school. A randomized controlled trial. Neuropsychology 37 , 859–871 (2023).
Kofler, M. J., Sarver, D. E. & Wells, E. L. Working memory and increased activity level (hyperactivity) in ADHD: experimental evidence for a functional relation. J. Atten. Disord. 24 , 1330–1344 (2020).
Rapport, M. D. et al. Hyperactivity in boys with attention-deficit/hyperactivity disorder (ADHD): a ubiquitous core symptom or manifestation of working memory deficits? J. Abnorm. Child. Psychol. 37 , 521–534 (2009).
Schachar, R. J. et al. Autism spectrum disorder and attention-deficit/hyperactivity disorder: shared or unique neurocognitive profiles? Res. Child. Adolesc. Psychopathol. 51 , 17–31 (2023).
Alderson, R. M., Rapport, M. D., Hudec, K. L., Sarver, D. E. & Kofler, M. J. Competing core processes in attention-deficit/hyperactivity disorder (ADHD): do working memory deficiencies underlie behavioral inhibition deficits? J. Abnorm. Child. Psychol. 38 , 497–507 (2010).
Alderson, R. M. et al. Working memory and behavioral inhibition in boys with ADHD: an experimental examination of competing models. Child. Neuropsychol. 23 , 255–272 (2017).
Kofler, M. J. et al. Working memory and information processing in ADHD: evidence for directionality of effects. Neuropsychology 34 , 127–143 (2020).
Goschke, T. Dysfunctions of decision-making and cognitive control as transdiagnostic mechanisms of mental disorders: advances, gaps, and needs in current research. Int. J. Methods Psychiat. Res. 23 , 41–57 (2014).
Bennett, C. L., Petros, T. V., Johnson, M. & Ferraro, F. R. Individual differences in the influence of time of day on executive functions. Am. J. Psychol. 121 , 349–361 (2008).
Lara, T., Madrid, J. A. & Correa, Á. The vigilance decrement in executive function is attenuated when individual chronotypes perform at their optimal time of day. PLoS ONE 9 , e88820 (2014).
Constantino, J. N. & Todd, R. D. Autistic traits in the general population: a twin study. Arch. Gen. Psychiat. 60 , 524–530 (2003).
Robinson, E. B. et al. Evidence that autistic traits show the same etiology in the general population and at the quantitative extremes (5%, 2.5%, and 1%). Arch. Gen. Psychiatry 68 , 1113–1121 (2011).
McLennan, J. D. Understanding attention deficit hyperactivity disorder as a continuum. Can. Fam. Physician 62 , 979–982 (2016).
PubMed PubMed Central Google Scholar
Yang, Y. et al. Child executive function and future externalizing and internalizing problems: a meta-analysis of prospective longitudinal studies. Clin. Psychol. Rev. 97 , 102194 (2022).
Dennis, M. et al. Why IQ is not a covariate in cognitive studies of neurodevelopmental disorders. J. Int. Neuropsychol. Soc. 15 , 331–343 (2009).
Howard, S. J. et al. Challenging socioeconomic status: a cross-cultural comparison of early executive function. Dev. Sci. 23 , e12854 (2020).
Alloway, T. P., Alloway, R. G. & Wootan, S. Home sweet home: does where you live matter to working memory and other cognitive skills? J. Exp. Child. Psychol. 124 , 124–131 (2014).
Bitsko, R. H. et al. Mental health surveillance among children — United States, 2013–2019. MMWR Suppl. 71 , 1–42 (2022).
Maenner, M. J. et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years — autism and developmental disabilities monitoring network, 11 sites, United States, 2020. MMWR Surveill. Summ. 72 , 1–14 (2023).
Lai, M.-C., Lombardo, M. V., Auyeung, B., Chakrabarti, B. & Baron-Cohen, S. Sex/gender differences and autism: setting the scene for future research. J. Am. Acad. Child. Adolesc. Psychiat. 54 , 11–24 (2015).
Millenet, S. et al. Sex-specific trajectories of ADHD symptoms from adolescence to young adulthood. Eur. Child. Adolesc. Psychiat. 27 , 1067–1075 (2018).
Cockcroft, K. Are working memory models WEIRD? Testing models of working memory in a non-WEIRD sample. Neuropsychology 36 , 456–467 (2022).
Cheon, B. K., Melani, I. & Hong, Y. How USA-centric is psychology? An archival study of implicit assumptions of generalizability of findings to human nature based on origins of study samples. Soc. Psychol. Personal. Sci. 11 , 928–937 (2020).
Webber-Ritchey, K. J. et al. Recruitment strategies to optimize participation by diverse populations. Nurs. Sci. Q. 34 , 235–243 (2021).
Rowley, S. J. & Camacho, T. C. Increasing diversity in cognitive developmental research: issues and solutions. J. Cogn. Dev. 16 , 683–692 (2015).
Buchanan, N. T., Perez, M., Prinstein, M. J. & Thurston, I. B. Upending racism in psychological science: strategies to change how science is conducted, reported, reviewed, and disseminated. Am. Psychol. 76 , 1097–1112 (2021).
Werner, K. M., Inzlicht, M. & Ford, B. Q. Whither inhibition? Curr. Dir. Psychol. Sci. 31 , 333–339 (2022).
Kofler, M. J. et al. Working memory and inhibitory control deficits in children with ADHD: an experimental evaluation of competing model predictions. Front. Psychiat. 15 , 1277583 (2024).
Howlett, C. A., Miles, S., Berryman, C., Phillipou, A. & Moseley, G. L. Conflation between self-report and neurocognitive assessments of cognitive flexibility: a critical review of the Jingle Fallacy. Aust. J. Psychol. 75 , 2174684 (2023).
Abikoff, H. et al. Remediating organizational functioning in children with ADHD: immediate and long-term effects from a randomized controlled trial. J. Consult. Clin. Psychol. 81 , 113–128 (2013).
Verbruggen, F., Chambers, C. D. & Logan, G. D. Fictitious inhibitory differences: how skewness and slowing distort the estimation of stopping latencies. Psychol. Sci. 24 , 352–362 (2013).
Duncan, A., Tamm, L., Birnschein, A. M. & Becker, S. P. Clinical correlates of sluggish cognitive tempo in adolescents with autism spectrum disorder. Autism 23 , 1354–1362 (2019).
McFayden, T. et al. Sluggish cognitive tempo in autism spectrum disorder, ADHD, and their comorbidity: implications for impairment. J. Clin. Child. Adolesc. Psychol. 51 , 195–202 (2022).
Becker, S. P. et al. The internal, external, and diagnostic validity of sluggish cognitive tempo: a meta-analysis and critical review. J. Am. Acad. Child. Adolesc. Psychiat. 55 , 163–178 (2016).
Becker, S. P. & Barkley, R. A. Sluggish cognitive tempo. In Oxford Textbook of Attention Deficit Hyperactivity Disorder (eds Banaschewski, T., Coghill, D. & Zuddas, A.) Ch. 15, 147–153 (Oxford Univ. Press, 2018).
McBurnett, K. et al. Structure and validity of sluggish cognitive tempo using an expanded item pool in children with attention-deficit/hyperactivity disorder. J. Abnorm. Child. Psychol. 42 , 37–48 (2014).
Kofler, M. J. et al. What cognitive processes are “sluggish” in sluggish cognitive tempo? J. Consult. Clin. Psychol. 87 , 1030 (2019).
Mayes, S. D., Calhoun, S. L. & Waschbusch, D. A. Relationship between sluggish cognitive tempo and sleep, psychological, somatic, and cognitive problems and impairment in children with autism and children with ADHD. Clin. Child. Psychol. Psychiat. 26 , 518–530 (2021).
Reinvall, O. et al. Sluggish cognitive tempo in children and adolescents with higher functioning autism spectrum disorders: social impairments and internalizing symptoms. Scand. J. Psychol. 58 , 389–399 (2017).
Mueller, A. K. et al. Sluggish cognitive tempo and its neurocognitive, social and emotive correlates: a systematic review of the current literature. J. Mol. Psychiat. 2 , 5 (2014).
Tamm, L. et al. Neurocognition in children with cognitive disengagement syndrome: accurate but slow. Child. Neuropsychol. 30 , 221–240 (2024).
Stark, R. & Mandl, H. Bridging the gap between basic and applied research by an integrative research approach. Educ. Res. Eval. 13 , 249–261 (2007).
Munro, C. L. & Savel, R. H. Narrowing the 17-year research to practice gap. Am. J. Crit. Care 25 , 194–196 (2016).
Mallonee, S., Fowler, C. & Istre, G. R. Bridging the gap between research and practice: a continuing challenge. Inj. Prev. 12 , 357–359 (2006).
American Educational Research Association (AERA), American Psychological Association (APA) & National Council on Measurement in Education. Standards for Educational and Psychological Testing (AERA, 2014).
Kane, M. J. & Engle, R. W. Working-memory capacity and the control of attention: the contributions of goal neglect, response competition, and task set to Stroop interference. J. Exp. Psychol. Gen. 132 , 47–70 (2003).
Hicks, K. L., Foster, J. L. & Engle, R. W. Measuring working memory capacity on the web with the online working memory lab (the OWL). J. Appl. Res. Mem. Cogn. 5 , 478–489 (2016).
Normand, S. & Tannock, R. Screening for working memory deficits in the classroom: the psychometric properties of the working memory rating scale in a longitudinal school-based study. J. Atten. Disord. 18 , 294–304 (2014).
Download references
Author information
Authors and affiliations.
Department of Psychology, Florida State University, Tallahassee, FL, USA
Michael J. Kofler, Leah J. Singh & Sherelle L. Harmon
Department of Psychology, Louisiana State University, Baton Rouge, LA, USA
Elia F. Soto
Department of Psychology, Florida International University, Miami, FL, USA
Emma M. Jaisle, Jessica N. Smith & Kathleen E. Feeney
Department of Psychology, Barnard College, Columbia University, New York, NY, USA
Erica D. Musser
You can also search for this author in PubMed Google Scholar
Contributions
All authors researched data for the article and contributed substantially to the discussion of the content. M.J.K., E.F.S., L.J.S., S.L.H, E.M.J., J.N.S., K.E.F. and E.D.M. wrote the article and reviewed and/or edited the manuscript before submission.
Corresponding author
Correspondence to Michael J. Kofler .
Ethics declarations
Competing interests.
The authors declare no competing interests.
Peer review
Peer review information.
Nature Reviews Psychology thanks Alisha Pollastri, Russel Schachar and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary information, rights and permissions.
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Cite this article.
Kofler, M.J., Soto, E.F., Singh, L.J. et al. Executive function deficits in attention-deficit/hyperactivity disorder and autism spectrum disorder. Nat Rev Psychol (2024). https://doi.org/10.1038/s44159-024-00350-9
Download citation
Accepted : 23 July 2024
Published : 29 August 2024
DOI : https://doi.org/10.1038/s44159-024-00350-9
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing newsletter — what matters in science, free to your inbox daily.


An official website of the United States government
The .gov means it’s official. Federal government websites often end in .gov or .mil. Before sharing sensitive information, make sure you’re on a federal government site.
The site is secure. The https:// ensures that you are connecting to the official website and that any information you provide is encrypted and transmitted securely.
- Publications
- Account settings
Preview improvements coming to the PMC website in October 2024. Learn More or Try it out now .
- Advanced Search
- Journal List
- Springer Nature - PMC COVID-19 Collection
Beyond Friendship: The Spectrum of Social Participation of Autistic Adults
Dara v. chan.
1 Division of Clinical Rehabilitation and Mental Health Counseling, Department of Allied Health, The University of North Carolina at Chapel Hill and The University of North Carolina TEACCH Autism Program, Chapel Hill, USA
3 Campus Box 7250, Chapel Hill, NC 27599 USA
Julie D. Doran
Osly d. galobardi.
2 Essential Counseling and Therapeutic Services, PLLC, Chapel Hill, NC USA
Difficulties with social interactions and communication that characterize autism persist in adulthood. While social participation in adulthood is often marked by social isolation and limited close friendships, this qualitative study describes the range of social participation activities and community contacts, from acquaintances to close relationships, that contributed to connection from the perspective of 40 autistic adults. Qualitative data from interviews around social and community involvement were analyzed and revealed five main contexts where social participation occurred: vocational contexts, neighborhoods, common interest groups, support services and inclusive environments, and online networks and apps. Implications for practice to support a range of social participation include engaging in newer social networking avenues, as well as traditional paths through employment and support services.
Introduction
The diagnosis of individuals with autism spectrum disorder (ASD) has risen dramatically, from 1 in 150 8-year-olds in 2002 to 1 in 54 in 2016 (Center for Disease Control, 2020 ). While prevalence rates are most closely monitored in children, ASD is a lifelong disorder characterized by social and communication impairments as well as repeated and restricted patterns of behavior (American Psychiatric Association [APA], 2013 ). While other symptoms of autism often plateau or improve in adulthood, characteristic social interaction difficulties persist and are potential contributors to lower rates of normative adult outcomes reported in the literature that involve social participation, friendships, or close relationships (Tobin et al., 2014 ).
Social Relationships in Childhood and Adolescence
Social participation includes the size and quality of social networks (Wong & Solomon, 2002 ), while friendship is defined as emotional relationships people form with another characterized by mutual affection, companionship, and reciprocal support and interaction (Freeman & Kasari, 1998 ; Parker & Gottman, 1989, as cited in Bauminger et al., 2008 ). Yet the importance of the size or number of social contacts related to well-being may vary through different life stages or the lifespan. Parker and Asher’s ( 1993 ) research with neurotypical children, meaning those who are typically developing, highlighted the importance of the need for only one close friend in childhood for better well-being. In this study, less loneliness was associated with having at least one close friend, even among children who were not accepted in their classroom. Loneliness denotes a negative emotional state from the subjective appraisal that the quality or amount of social interaction desired does not match one’s actual social experience (Elmose, 2020 ; Peplau & Perlman, 1982 ). This is different from solitude, which may be preferred and important (Elmose, 2020 ; Mazurek, 2014 ; Peplau & Perlman, 1982 ). In the literature, loneliness also differs from social isolation, which in contrast to the subjective appraisal of one’s social relationship status, objectively examines one’s amount of social contact (Mazurek, 2014 ).
There is some support for the similar importance of having a close friend as potential protection against feelings of loneliness in autistic children. Autistic children identified quality friendships in a small circle of supportive friends as an important measure of their well-being, and the preference to have a few close friends who can be trusted (Lam et al., 2020 ). Similarly, Rotheram-Fuller et al. ( 2010 ) identified autistic children who had at least one reciprocal friendship, defined in the research as two children both nominating one another as friends (Kasari et al., 2011 ), also had greater peer acceptance. While these close friendships may have important implications, they are less frequent. A study of parent reports of friendships indicated 34% of autistic children had at least one good friend, compared to 71% of children with other disabilities and 93% of neurotypical children without disabilities (Rowley et al., 2012 ). Having one close friend may offer some protection against loneliness, although reciprocal friendships may be less common among autistic children compared to neurotypical children.
Social and communication impairments are often tied to difficulties with developing these reciprocal friendships in childhood. In the regular classroom, autistic children may experience the social structure of inclusion, but often still appear on the fringe of social activities, with higher rates of loneliness and poorer friendship quality than their neurotypical classmates (Kasari et al., 2011 ; Locke et al., 2010 ). For example, in a study examining playground observations as well as self, teacher, and classmate reports, Kasari et al. ( 2011 ) found autistic children were more likely to be socially isolated, meaning not a part of any social group in the classroom, or identified as only having peripheral social status compared to their neurotypical peers.
Other findings using measures of friendship quality, which evaluates the degree of companionship, help, security, and closeness between an identified friend, are often lower for autistic children and adolescents (Kasari et al., 2011 ; Locke et al., 2010 ). Friendship quality, however, is not commensurate with friendship satisfaction, as satisfaction with friendship may be fulfilled through a few friends or from friends outside the school setting (Petrina et al., 2017 ). Calder et al. ( 2012 ) noted autistic children were generally satisfied with their level of friendship. Petrina et al. ( 2017 ) also found rates of friendship satisfaction were similar for autistic and non-autistic elementary school children, with the level of perceived friendship reciprocated by named neurotypical peer friends in the study. These named friend pairs were often connected through common interests in childhood which carried into adolescence. Available survey data from Orsmond et al. ( 2004 ) on peer relationships in autistic adolescents found 20.9% had at least one friendship with shared activities, but only 8.1% had one close reciprocal friendship, and almost half had no peer relationships at all.
Social Relationships in Adulthood
When examining the quality of social networks in adulthood, including peer relationships and friendships, systematic reviews of the available research report adults across the spectrum have poorer social relationships than both neurotypically developing peers and those with intellectual disabilities, learning disabilities, and speech language disorders (Gotham et al., 2015 ; Kirby et al., 2016 ; Levy & Perry, 2011 ; Orsmond et al., 2013 ; Roux et al., 2013 ). Unlike childhood, where autistic children are more likely to initiate engagement with neurotypical peers in the classroom rather than with other children with disabilities (Bauminger et al., 2003 ), in adulthood there is some support for a preference for relationships with others on the spectrum (Milton & Sims, 2016 ; Morrison et al., 2020 ). For example, Morrison et al. ( 2020 ) conducted a study in which they paired autistic and neurotypical adults for a 5-minute social interaction. Researchers found that autistic adults preferred to interact with other autistic adults and were more likely to reveal more about themselves to them compared to neurotypical participants (Morrison et al., 2020 ). Sedgewick et al. ( 2019 ) compared ratings of close relationships between 532 autistic and 417 non-autistic adults and found no significant differences when rating their relationship with a long-term partner or spouse, indicating that autistic adults may feel the same level of closeness to a marriage or long-term partner as neurotypical adults (Sedgewick et al., 2019 ). Similarly, in survey research with 108 autistic adults, 60% reported having a close or best friend, which was significantly related to less loneliness (Mazurek, 2014 ). Furthermore, in a qualitative study of 15 adults and nine caretakers of autistic adults, some participants described having a limited number of close friendships as important for aging well (Hwang et al., 2017 ), which may indicate satisfaction with a few close relationships.
In the neurotypical population, however, particularly with aging in adulthood, the benefits of social participation shift away from the importance of having one close friend. A number of researchers have identified having a broad network of social contacts in adulthood as a key contributor to factors supporting healthy aging, including mental health (Achat et al., 1998 ; Michael et al., 1999 ; Uchino et al., 2001 ). In older adulthood, larger social networks are related to better global cognition (Kelly et al., 2017 ), while perceived social connectedness is significantly related to self-reported health status (Ashida, 2008 ). Much less is known about the impact of the size or extent of social networks in autistic adults. In the Mazurek ( 2014 ) survey study, number of friends was an important predictor of better self-esteem and less depression and anxiety, suggesting quality and quantity matters. However, social participation outcomes have previously been measured by assessing the number of friendships, frequency of contact or activities with friends, or even a dichotomous measure of the presence or absence of social activity within a defined period, such as the past month or past year. These measures may not accurately capture social participation, or the perceived size and quality of social contacts (Myers et al., 2015 ; Orsmond et al., 2013 ; Steinhausen et al., 2016 ; Tint et al., 2016 ). For example, in a qualitative study of 38 autistic adults examining factors influencing quality of life, McConachie et al. ( 2020 ) found that some participants described difficulty with engaging in social interactions, while others described a lack of desire for friendships altogether, representing a range of social participation preferences.
With differences between autistic and neurotypical individuals in mind, the neurodiversity perspective challenges the use of normative outcomes as the benchmark for success in adulthood. A neurodiverse framework acknowledges the difficulties the autism community faces, while also presenting the commonalities that characterize autistic individuals as strengths and differences rather than inherent deficits (Baron-Cohen, 2017 ). Social, environmental, or attitudinal barriers, however, can magnify the extent to which these differences interfere with the individual being able to engage in typical participation outcomes. Similarly, as opposed to a medical model focused on deficits, viewing autism as an identity and culture replaces typically held beliefs about social impairments and difficulties with the concept that individuals on the spectrum possess social skills, but they may be different than those of neurotypical individuals (Herrick & Datti, 2020 ).
With this perspective in mind, friendships and social participation may look different for individuals on the spectrum. For example, autistic adults may plan their social interactions to include less face-to-face contact to meet their social needs without being overwhelmed (Elmose, 2020 ). Attending concerts, movies, or sporting events may be preferred activities because these activities are more scripted and require less verbal communication. In other cases, individuals may appear to others to be on the periphery of social interactions and not involved, but still themselves consider the activity as social and participating with others (Bagatell, 2010 ). Additionally, online social networking platforms may serve as an important facilitator of friendship development for autistic individuals (Brownlow et al., 2015 ). These online friendships may appear to be of lower quality when assessed using a neurotypical model of friendship, but autistic individuals may engage in meaningful and important relationships through the online setting (Brownlow et al., 2015 ). Furthermore, Mazurek ( 2013 ) found autistic adults who used social networking platforms were more likely to report having a close friend compared to those who did not use online social networking.
Range of Social Participation
For all individuals, there are different levels of social participation and engagement. Social connections can range from casual encounters, such as greeting a neighbor or stranger, to having acquaintances with those who are familiar but not known well, to close friendships and relationships where individuals feel known and accepted (Wood et al., 2015 ). While past research has primarily focused on close friendships and relationships, a better understanding of the range of social participation experiences is needed to determine potential benefits in adulthood. Research on healthy aging in adulthood stresses the importance of making social connections and forming these connections in a variety of ways that are personally meaningful (Ashida, 2008 ; Michael et al., 1999 ; Uchino et al., 2001 ). Within the autism community, there is a call to research the strengths and unique perspectives of individuals to add validity and depth to the outcomes measured (Henniger & Taylor, 2012 ; Howlin & Taylor, 2015 ). Research on the individual subjective experience of social participation of autistic adults will meet this gap (Tint et al., 2016 ).
Purpose of the Study
There is little qualitative research on the breadth of social interactions and experiences among autistic adults, and how these different types of engagements are perceived by autistic adults. Beyond the normative ways of thinking about friendships, more information is needed regarding which social connections adults with autism are engaging in that are meaningful, and how they are making connections they feel are important to them. Understanding where meaningful social participation occurs, and the contexts that frame or promote these interactions, are important for developing client-centered services and client-identified goals (McCollum et al., 2016 ). Seeking input from the autistic individual on meaningful social activities and connections both empowers the individual to provide information as an expert on the experience and can facilitate a deeper understanding of which activities and interactions are significant (McCollum et al., 2016 ; Tobin et al., 2014 ). The purpose of this study is to describe the range of social participation experiences of autistic adults to better understand, from the individual’s perspective, where and how these meaningful social contacts occur.
This study draws on data collected as part of a larger mixed methods project aimed at understanding the community participation of autistic adults. The qualitative data describing social interactions and community connections in the larger study are the focus of this analysis.
Participants
Participants were recruited through an autism research registry affiliated with a university in the southeastern United States. This registry maintains a list of individuals with autism who have indicated interest in participating in autism research, and contacts individuals on the registry based on the study’s inclusion criteria. The registry contacted potential participants for the current study who could communicate (verbally or nonverbally) in English and had an intelligence quotient (IQ) of 70 or above on record with the registry. IQ was confirmed through psychological reports previously submitted to the registry or through a previous diagnosis of Asperger’s Disorder. Recruitment invitations were sent from the registry via mail and email in groups of 30 by geographic catchment area, with approximately a 20% response rate. Interested participants could respond to the registry or the principal investigator. Research team members contacted interested individuals to confirm their ability to complete two 60-minute interviews and that a typical week of community participation could be captured during the study week.
Data were collected primarily using semi-structured interviews to assess the importance of community activities, feelings of belonging, and social connectedness from the individual’s perspective. Over the 2-year study period (2019–2021), the majority of interviews ( n = 29) were completed in person with the research team traveling to the participant’s community area prior to the beginning of the COVID-19 pandemic. Data collection after March 2020 ( n = 11) was completed via Zoom and required that participants have reliable internet access. These interviews included additional questions regarding how participants’ social and community participation changed since the onset of COVID-19.
Each interview was conducted after the participant finished a week-long data tracking process recording community activities through participants carrying a GPS tracking device and completing a daily travel diary. No intervention was included in the larger study. The interviews focused on the activities that occurred during the week, facilitators and barriers to participation, the importance of different locations visited in the community, and feelings of belonging and social support in the community. Primary study questions such as “Where do you typically see your friends?” “Are there any activities you wish you were more involved with?” “Do you feel a part of your community?” and “Who is your biggest form of social support?” often prompted discussion related to social participation. Prior to the current study, pilot testing of each project component and the interview guide was completed with 12 autistic adults which resulted in some modifications to the questions and response style of the measures used in the larger study.
The university Institutional Review Board approved all aspects of the study. Written consent was received from participants or their guardians, including consent to record the interviews. Participants with consenting guardians ( n = 5) verbally assented to participation. One participant was minimally verbal but was able to respond through confirming his family member’s responses to questions. The tracking data of community activities was used to triangulate the report of social activities if they occurred during the tracking week. After study participation, a summary of interview data including general themes of the interview and question responses was sent to each participant. Participants were asked to confirm that the information was accurate or provide changes as necessary as a form of member checking.
All authors were involved with the data collection, interviews, and analysis process. Interviews were transcribed verbatim and coded using open coding methods by the principal investigator and two master’s level research assistants (RA) on the project. All members of the research team are clinical rehabilitation and mental health counselors with experience working with autistic individuals through research, service provision, and/or as an immediate family member.
Interview data were analyzed using a multi-step approach. First, interviewers recorded detailed notes on the semi-structured interview guide during or immediately following the study visit to capture participant responses to key questions. When approximately half of the sample had completed the study, the research team met to reflect on common threads noted throughout the data collection process from these notes. Potential codes and emerging themes were identified in this process, with a particular emphasis on ten case studies. This initial conventional content analysis (Hsieh & Shannon, 2005 ) of the ten cases highlighted social networking facilitated activities, vocational related opportunities, and the importance of personal and formalized supports. A matrix was constructed that included participant demographic information, emerging codes and potential themes, and illustrative quotes (Averill, 2002 ; Hamilton & Maietta, 2017 ).
This initial analysis of ten case studies served as the foundation for further analysis. Transcripts were then independently reviewed by two team members using line by line coding for the presence of the initial representative codes or emergence of new codes and themes. The study team met regularly to review findings and compare coding results, with high agreement in coding. Sharing findings from the coding process often confirmed and expanded some of the previously identified experiences from the ten cases but also noted differences in the level of engagement or meaning of interactions and preferences across the spectrum of participation, prompting a return to the review of the data. After data collection was nearly complete, the matrix and key quotes were revisited, and the team applied a neurodiversity framework to analyze the quotes. Using a neurodiversity approach resulted in a refined focus on the range and meaning of social participation reported across participants, reframing differences in social participation as such rather than emphasizing differences as deficits. For example, during the first round of data analysis, relying exclusively on online social connections was coded as a barrier to social participation. When the team applied the neurodiversity framework, however, quotes regarding online social connections were re-coded as an important way individuals were maintaining social contacts with friends living in other geographic areas.
Forty adults participated in the study. Participant demographics are described in Table Table1. 1 . Participant age had similar dispersion and averages for males ( n = 27, M = 37.89 years, SD = 11.84) and females ( n = 13, M = 37.69, SD = 8.57). At the time of study participation, 55% ( n = 22) were employed in some capacity (full-time or part-time), 45% ( n = 18) lived independently or with a spouse or partner, and 67.5% ( n = 27) drove independently. Most participants ( n = 36, 90%) lived in urban areas, as classified by the Rural-Urban Commuting Area Codes ( https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes.aspx ).
Demographics of the sample of autistic adults ( n = 40)
| Demographics | |
|---|---|
| Age | |
| Mean (SD) | 37.89 years (10.77) |
| Range | 24–62 years |
| Male | 27 (67.5%) |
| Race | |
| White | 33 (82.5%) |
| Black/African American | 4 (10%) |
| Multiracial | 3 (7.5%) |
| Waisman activities of daily living scale score | |
| Mean (SD) | 30.75 (4.99) |
| Range | 10–34 |
| Highest level of education | |
| High School | 3 (7.5%) |
| Some college | 10 (25%) |
| Graduated 2-year college | 4 (10%) |
| Some vocational school | 3 (7.5%) |
| Graduated vocation school | 2 (5%) |
| Some 4-year college | 5 (12%) |
| Graduated 4-year college | 7 (17.5%) |
| Advanced degree | 6 (15%) |
| Employment status | |
| Never employed | 6 (15%) |
| Currently employed | 22 (55%) |
| Previously employed, currently unemployed | 11 (27.5%) |
| Living situation | |
| With parent, relative, caregiver, or guardian | 21 (52.5%) |
| Independent | 8 (20%) |
| With spouse or roommate | 10 (25%) |
| Group home | 1 (2.5%) |
| Psychiatric diagnosis (ever diagnosed) | |
| Anxiety | 18 (45%) |
| Depression | 20 (50%) |
| Other psychiatric diagnosis | 9 (22.5%) |
| Parent highest level of education | |
| High school | 3 (7.5%) |
| Graduated vocation school | 4 (10%) |
| Some college | 4 (10%) |
| Graduated 4-year college | 13 (32.5%) |
| Advanced degree | 16 (40%) |
a The Waisman activities of daily living scale (Maenner et al. 2013 ) was administered in the context of the larger study to assess independence in completing daily living skills
Social Participation
Participants described social participation in a variety of contexts clustered around five main themes: (1) Vocational contexts, (2) Neighborhoods, (3) Common interest groups, (4) Support services and inclusive environments, and (5) Online networks and apps. A short description and example of each theme is included in Table Table2. 2 . In all contexts, participants reported experiences that ranged across the spectrum of social participation that included casual encounters, engaging with known acquaintances, or engaging with close friendships or relationships. However, the results are purposefully structured by location and not level of engagement to show that social participation occurred at different levels in each context fostering a sense of belonging, which differed from person to person. Therefore, the goal was primarily to let the data tell the story, through the participants’ own words, and in response to specific interview questions. It is of note participants used some of these contexts to practice social interactions that they then applied to other settings or at other levels of engagement. Quotes were edited slightly for clarity and pseudonyms were assigned to each participant to protect confidentiality.
Overview of social participation themes
| Theme | Description | Example |
|---|---|---|
| 1) Vocational contexts | Employment, educational or volunteer experiences | “It’s work. It’s my practice ground. Social interaction practice.” |
| 2) Neighborhoods | Interaction with neighbors | “I guess I am part of a neighborhood community. I wouldn’t be if I didn’t walk the dog. But you meet a lot of people.” |
| 3) Common interest groups | Activities involving shared interests | “[Improv is] great for social skills. Oh my gosh, it’s so good for social skills.” |
| 4) Support services and inclusive environments | Disability support services | “I was diagnosed with autism at [autism organization]. And then they had an adult support group there, too, monthly and I would go there. Originally, I would go there by myself, and there would be a few other guys with autism that I got friendly with there too.” |
| 5) Online networks and apps | Internet-based platforms | “I think that’s [online communities] just as significant really. It’s still, you know, a community. It’s still a group of people that you share interests and ideas with.” |
Vocational Contexts
Some participants described vocational activities of employment, volunteering, and pursuing education as an avenue for social participation. Participants described work as a place to interact positively with others. For some it offered a sense of belonging, for others, it served as an important avenue for practicing social interactions. For example, Tyler reported his place of work was most important to him because, “It’s work. It’s my practice ground. Social interaction practice.” Similarly, Warren discussed how, prior to his diagnosis of autism, he worked as a grocery store clerk to practice interacting with others, stating,
So, for a while, I got a job, in order to put myself in a spot where I’d have to interact with more people. I got a job at a grocery store for about two months in addition to my other job. That was just so I could learn to interact better with people.
Another participant described the importance of his volunteer activities as an usher as a means to interact positively with others:
Well, I mean, when I usher, I interact with a lot of people. So, it's just getting—talking to people I don’t know. And I mean I have, um, people that are season ticket holders, so they come back every year. So, it’s nice just to see.
Additionally, one participant described his attendance at graduate school as offering a context to practice social skills and foster in-person social connection:
And so, once I went to grad school, I realized I’m far away from home…and I can’t just survive just being online anymore. I don’t ... have like my family for support—things like that. So, I literally just made like a concerted effort to study social skills by myself, as well as get as many experiences as possible to, uh, get to the point where I am today.
From these efforts, Brian developed a network of friends he remains in contact with, “I have like a group of friends from back in grad school I text with, all the time.”
Jack reported volunteering was among one of his favorite activities and commented on the importance of community built there, stating, "I like attending the different meetings for the groups, like the consumer family group for Lions. I just joined a group in a human rights committee at [psychiatric hospital]." Work also provided a sense of belonging and community for some participants. For example, when Bob was asked where he felt he belonged the most, he replied, “Work. It’s where I feel most confident.” When asked where he belonged the most, Joshua, who worked at a service organization for autistic individuals, stated, "Probably [autism organization], because I have been working there for—for a long time and I'm friends with pretty much everyone there.”
Even participants who did not work or participate in organizations directly serving those on the autism spectrum were able to find neurodiverse communities that offered social connection. For example, Brian participated in a neurodiversity group at his place of work and even created an international “autistic task force” within his business. He noted, “I'm active in the neurodiversity business resource group. So that’s been helpful.” Overall, employment, volunteer, and educational settings provided a means for shared common interests, interaction practice, and familiarity with others at different levels of social participation that increased feelings of belonging and connection to a group, and in some cases fostered meaningful social connections that endured.
Neighborhoods
Neighborhoods were identified as an environment promoting meaningful social engagement and personal security. Participants described visiting with friends and acquaintances within their local neighborhood communities as well as neighbors providing a sense of safety. For example, when asked where she usually saw her friends, Julia commented, “I think it's basically around the neighborhood and everything since we live like really close to each other and everything.” Daniel commented on how his neighbor promoted feelings of safety, stating, “There's a real involved next-door neighbor who would never let anything happen,” and indicated this security enabled him to be more independent.
Participants also specifically described pets as promoting social interaction within their neighborhood communities, and these interactions contributed to them feeling a part of the community. Travis stated, “I guess I am part of a neighborhood community. I wouldn’t be if I didn’t walk the dog. But you meet a lot of people.” Similarly, when asked if he felt part of his community, Nathan described how he spoke with neighbors while walking his cat in the neighborhood, stating, “I mean, I do get out occasionally. And if people see me with Cat, they’re pretty impressed and want to talk to me.”
Common Interest Groups
Activities involving a common interest offered opportunities for social engagement for many participants. For example, attending church fellowship provided a sense of belonging and place of connection to others through shared faith. Jack described his favorite activity in the community as “...going to church and being in the choir and things. I enjoy that.” Other participants felt a sense of belonging within their church, Bible studies, or faith-based communities. When asked where she felt she belonged the most, Hannah stated, “Oh, Kingdom Hall is the one that I belong [to] the most.” She described how her church community was accepting and provided a context for meaningful social engagement. Another participant, Kathryn, also described a Bible study and church as where she belonged the most.
Some participants described gaming as a common interest that increased social engagement. For example, Brian reported he participated in game nights frequently: “Playing cards—like I will be gone to board games multiple times a week regularly.” Nathan also described how he ran a Dungeons and Dragons clan, an interactive game, to connect with friends. Peter described his interaction with others through online gaming platforms but wished to play in person as well: “I’ve been dabbling in Pathfinder and Dungeons and Dragons on—with my Discord friends, but I’d like to be with an actual physical group one of these days.” Melissa participated in an improvisation group frequently and described how this allowed for important social skills practice, reporting, “[Improv is] great for social skills. Oh my gosh, it’s so good for social skills.” Common interest groups were used to interact with friends and acquaintances at times and were even used to practice interacting with others in a safe environment.
Support Services and Inclusive Environments
Some participants utilized formalized support services to create meaningful social relationships and also described specific service organizations as offering a sense of acceptance and safety. Specifically, autistic adult support groups were described as a means of providing social connection and comfort. For example, when asked where he felt most comfortable, Charles responded, “I’d probably say [my] support group.” Similarly, Joe noted,
I was diagnosed with autism at [autism organization]. And then they had an adult support group there too, monthly, and I would go there. Originally, I would go there by myself, and there would be a few other guys with autism that I got friendly with there too.
Similarly, two participants commented on the importance of a specific camp for individuals on the autism spectrum. Brian noted he met one of his closest friends at this camp and Joe commented he and his closest friend had attended the camp as a social activity together. Participants commented on how organizations specifically serving individuals with autism and developmental disabilities provided a sense of belonging and safety. Jerry commented,
You know, you come to [organization for individuals with developmental disabilities], you come to [another autism organization], this is like safe. Say what you want to. Do what you want to. You're not likely to go run into any problems [there].
These examples of connections attributed through supportive agencies and inclusive spaces were often described as leading to the development of friendships, where individuals met as strangers or acquaintances but developed closer relationships because they were able to be themselves without fearing judgment.
Although based on a professional relationship, therapists, support staff, and service animals were specifically described as important forms of social support as well. Danielle stated her biggest form of social support was a support staff who worked with her group home. Tyler described how his service dog increased his social motivation and ability to connect with others when he went out into the community. He stated: “I think this [service dog] really helped me. ‘Cause I was, you know, I was in a tough situation before I moved here. Just not much to do, not much motivation. She [my service dog] definitely helped with that.” The addition of extra support or encouragement to engage in social settings was important for initiating these contacts.
Online Networks and Apps: “ That’s the way I communicate. ”
Several participants commented on online social networks promoting social interaction in a variety of ways. One way in which online platforms were used was to facilitate in-person gatherings. Brian and Melissa indicated they had arranged dates using dating apps. Participants also described using or trying Meetup, an online platform designed for people who share similar interests to meet for events in person. Tyler, Brian, and Troy reported they used Meetup frequently to meet others for social activities in the community such as beer tastings, game nights and rock-climbing events. In fact, when asked about his biggest form of social support, Troy commented that he had used Meetup to connect with individuals at his rock-climbing gym and how Meetup provided a simple means of meeting new people. He stated, “Meetup’s a, you know, pretty good way to go out to do something without really, you don’t need too many social skills to at least sign up and get there, and I guess you’re on your own after that.”
Others described using a variety of online platforms for communication purposes. Joe stated, “Now I’m on Facebook groups a lot—autism AS groups communicating with people and I get to know people and it’s just, yeah, I’m really happy.” Hannah also reported, “I do, I do write on Facebook and stuff... That’s the way I communicate.” When asked where he usually saw his friends, Michael responded, “Online. I used to use Facebook but not anymore. Now, I use one called MeWe.” When asked the same question, Catherine responded, "Usually they're internet friends, so I just talk with them online." Brian noted, “And I also have a friend on Twitter I'm pretty close to.” Participants utilized many different social networking platforms to communicate with individuals, ranging from casual encounters, acquaintances, and close personal friends.
Beyond individual relationships, a few participants discussed using social networking platforms to establish important online communities. When asked if she felt part of her community, Catherine stated, “Yeah, the online one, definitely. I can—we have discussion, and—it feels like I'm involved, and my opinions are taken. Like, they—they hear my opinions.” Similarly, Isaac described his view of online communities being of the same importance as typical communities: “I think that’s just as significant really. It’s still, you know, a community. It’s still a group of people that you share interests and ideas with.” Brian, who moved to a new town approximately one year prior, reported he used online platforms to connect with friends in other areas while waiting to build a community closer to home, “I’ve been able to get a good—good network of people—to some extent. They’re mostly online, now, ‘cause I haven’t made full close friends down here.” For some participants, social interactions online led to feelings of belonging and community, and at times prompted the building of connections across the social spectrum, from stranger, to someone familiar, to a supportive community.
The current study is consistent with findings in prior qualitative studies where many, but not all, autistic adults desire social connections (Causton-Theoharis et al., 2009 ; Muller et al., 2008 ). In the present study, autistic adults were engaging in a range of social participation experiences in a variety of contexts. Moreover, these autistic adults were using different venues to intentionally practice social skills, including in-person engagement and online connections. Reports of casual encounters with neighbors or acquaintances were meaningful and contributed to individuals feeling part of their communities. With a significant focus in the literature on loneliness, isolation, and friendship quality in autistic adults, the current study provides some initial support to think more broadly about the context of where social participation and interactions take place and the meaning ascribed. These findings may provide more context to past research by Mehling and Tasse ( 2014 ), who found that individuals with and without autism were participating in the community at similar rates but those with autism reported lower levels of friendship, implying these community interactions were not leading to increased friendships for autistic adults. In conjunction with the current findings, it is possible that autistic adults are socially participating and active in their communities, but it may not extend to the level of a close friendship. Autistic adults may still need some support in finding or developing these closer connections in the community, if desired.
The role and use of video games, online connections, and social media by autistic individuals has received increased attention in the literature, particularly related to social participation and friendship (Mazurek et al., 2013 , Milton & Sims, 2016 ; Schalkwyk et al., 2017 ; Sundberg, 2018 ). In childhood, Mazurek and Wenstrup ( 2013 ) found time spent playing video games was associated with less time socially interacting or using social media in autistic children compared to their neurotypical peers. In adolescence and adulthood, online connections, social media use, and playing online video games with others has previously been associated with higher friendship quality, more friends, and less loneliness (Kuo et al., 2013 ; Milton & Sims, 2016 ; Schalkwyk et al., 2017 ; Sundberg, 2018 ). While online connections are often perceived as less meaningful in the neurotypical view of social participation, Mazurek’s ( 2013 ) study examining social interactions and friendships reported almost half of the autistic adults in the study used electronic communication to contact close friends through email, text, chat or social media at least once a day or several times a day, whereas in-person visits or phone contacts were more likely to occur on a monthly basis. The current study contributes to the literature supporting the meaning and feelings of belonging attributed to these electronic connections, and new evidence of the progression of independently using technology to meet others in person through using Meetup groups and online dating apps. Participants in the current study did not exclusively use technology for social connections but merged the use of technology and online platforms to engage in in-person connections in the community.
The current study found evidence for the importance of connecting with other individuals on the spectrum in adulthood, whether through in-person support groups with other autistic adults, close personal friendships, seeking online communities specifically for autistic adults, or creating an autistic task force at work to support coworkers who are also on the spectrum. Past research notes autistic adults are more likely to disclose more about themselves to other autistic adults and prefer to interact with others on the spectrum, where they can speak freely about their interest (Milton & Sims, 2016 ; Morrison, 2020 ). As noted by Milton and Sims ( 2016 ), relationships with others who identify as autistic are very important, especially in fostering feelings of acceptance and safety. Consistent with our findings, online forums provide a space for these relationships. However, in-person connections at work or through autism support agencies were also identified as meaningful places of social connection with other autistic adults. It is of note that the importance of connecting with other autistic adults may represent a shift from childhood, where autistic children show a preference for interacting with neurotypical peers in a classroom setting (Bauminger et al., 2003 ). In adulthood, the current study provides preliminary support for a broader range of social participation with both autistic and neurotypical individuals.
There is also specific support for Elmose’s ( 2020 ) notion of “accessibility” as an important factor facilitating social relationships in autistic adults, where partners, spouses, school, or work helped build connections and ease interactions. For some of the current participants, shared interests in games nights, faith communities, work, volunteer, or educational settings provided important contexts encouraging connections of convenience and interaction with others. Different types of roles, such as partner, employee/volunteer, neighbor, or group member, in different contexts led to accessibility for opportunities for social participation.
Participants in the current study reported feeling safe at organizations for individuals with autism and developmental disabilities and connecting with others through online autism groups. Participants also reported using work or volunteer positions as a safe space to intentionally practice social skills with others. This connects to Elmose’s ( 2020 ) findings that autistic adults actively decode the social rules of situations or interactions with people based on past experiences, and plan ways to make social interaction easier. However, unlike some of the participants in Elmose’s ( 2020 ) study who reported seeking out activities such as going to the movies, sporting events, or concerts where there was less social interaction or the social interaction would be more predictable, the current study noted examples of participants actively seeking out social interactions, through work, volunteer positions, or joining an improvisation class, that were less predictable to practice and improve their social skills.
Finally, it is of note in the autism literature on isolation and loneliness that more attention has been given to the importance of perceived loneliness and the subjective experience of social interaction in determining the impact on well-being (Mazurek, 2014 ; McConachie et al., 2020 ). Not everyone in the current study preferred to engage in social interactions, as clearly stated by one participant who commented, “I don’t like people.” Additionally, there were several participants who responded, “I have no friends,” when asked where they typically see their friends. However, a number of participants perceived themselves as being engaged in meaningful social interactions in a variety of contexts and at various levels of social participation that contributed to feelings of belonging that may or may not require having a close friend in adulthood. This finding provides preliminary support for the formation of a sense of community and feelings of belonging. Even those who desired more social connection reported other community connections, in-person or online, with individuals at the casual encounter or acquaintance level that helped them feel connected to their sense of community.
Limitations
While the purpose of the larger study was to describe the community participation experiences of autistic adults, including social participation, data collection was not created around exploring different levels of social engagement, or differences in the quality of friendships found in different contexts, such as in person or online connections. We attempted not to impose our own lens in interpreting the findings and ascribe meanings to the range of social connections described, but rather sought to let the data speak for itself. When asked where participants saw their friends, we assumed their responses included descriptions of meaningful friendships, and at times, this question elicited direct statements of not having friends. Elsewhere, participants openly described the lack of close friendships, or acknowledged that contacts remained at an acquaintance level. However, often participants described social contacts at all levels in relation to identifying places where they felt they belonged, places that were most important to them, and as contributing to feeling part of the community.
Similarly, the current study did not begin from a neurodiversity framework to specifically focus on strengths of individuals in the context of social participation. However, when participants described different means of social engagement that seemed to be working in connecting with others for significant friendships, dating, or marriage partners, we often prompted them to share more in hopes of understanding the different contexts and/or supports that were helpful in facilitating these meaningful connections. Additional study limitations include a small sample from a limited geographic region. Furthermore, inclusion criteria of an IQ of 70 or above means the entire autism spectrum is not represented in our findings. Additionally, most data were collected before the beginning of the COVID-19 pandemic. However, some ( n = 11) were collected via Zoom interviews during the pandemic, which expanded our geographic reach but also required that participants have access to reliable internet connection, thus excluding some participants. Participants in the current study indicated if they were ever diagnosed with a mental health condition on a demographic survey. However, we did not collect information regarding current psychiatric diagnoses, which may have impacted social participation unless it was shared directly during the interview. For example, Kayla noted, “I have really bad social anxiety at times...especially for places that are unfamiliar.” Finally, we did not collect any information regarding prior participation in social skill interventions, which may have promoted social engagement.
Implications for Practice
In addition to social skills training groups, our findings suggest the need for structured opportunities for social interactions and individualized approaches to promote social participation in areas of interest. This may be part of providing comprehensive supports for autistic adults through an interdisciplinary approach including professionals such as rehabilitation counselors, recreational, and occupational therapists. While social skills training can be an effective intervention, providing structured opportunities, such as practicing social interaction in community contexts with professional support, could be another step in promoting social participation in autistic adults. Offering information about online platforms that can be used to facilitate in-person social interaction may be an avenue for fostering new social connections. Additionally, encouraging participation in natural practice spaces for social interaction at work and in common interest groups may offer potential means for social interaction. Because adults with autism may desire spaces in which they can discuss their interests (Milton & Sims, 2016 ), these natural practice grounds, especially when related to common interest, may allow adults with autism to engage with others in a way that they prefer. For example, if an individual has an interest in gaming, participating in a gaming group would allow the individual to speak freely about their interest while engaging with others.
While encouraging the use of online platforms to facilitate in-person interaction and participation in common interest groups may be potential avenues for meaningful social connection, formalized support services also offered safe spaces for our participants to engage with others with developmental disabilities, and potentially develop closer relationships. Taken a step further, support groups could offer opportunities to organize social outings or discuss ways to meet new people. Additionally, individual therapy sessions could be utilized to practice social skills and discuss contexts in which these skills could be practiced. For example, clinicians could collaborate with clients to identify where they might practice social interactions in various contexts in the community including volunteer sites, the grocery store, or in the neighborhood, with or without a pet. Therapists could challenge clients to think about how they might interact with individuals in these locations. Additionally, therapists could assist clients to plan when the social outing would occur, how to self-manage their capacity for social interaction in the community, and create an exit strategy if the activity becomes overwhelming or overstimulating.
To increase community and social engagement, our research team created “personalized mapping profiles” for each participant, depicted in Figure Figure1. 1 . These profiles included locations visited during the study week, other important locations they noted that were not visited during the study week, approximately 10 new locations the participant could visit based on identified interests during the study interviews, and information about Meetup with approximately three suggested Meetup groups. A description of each new location, a color-coded map with its location relative to the participant’s home, and the website link was included in each profile. Creating similar mapping profiles could provide a visual representation of new locations of interest in community and provide new ideas for potential contexts for social interaction.

An example slide from the personalized mapping profiles developed for participants
Participants in the current study highlighted how they had both practiced social skills and found meaningful social connections in the workplace. Employment supports independence in the community and could potentially have the added benefit of developing social connection for autistic adults. Providing employment support to this population may have the benefit of fostering natural supports and providing a safe context for social practice. Referrals to vocational rehabilitation agencies or to support agencies with expertise in supported employment for autistic adults may increase employment attainment and social participation.
Future Directions
Although social networking promoted social engagement in many cases, participants also described having the majority of one’s friends out of town or online as a barrier to social interaction. Peter explained, “I haven’t spoken with most of my non-online friends in ages.... most of the friends I do have online are either somewhere across the ocean, somewhere on the other side of the country.” Similarly, Michael indicated he would like to attend parties and go to bars with friends but was not presently participating in those activities. When asked about barriers to these activities, he explained, “A lot of my friends are out of town,” and later described most of his friends were online. Because research has shown social connection is important to healthy aging (Michael et al., 1999 ; Uchino et al., 2001 ), it is worth noting that some participants described their social interactions as primarily online. Although beyond the scope of our research, understanding whether online friendships and interactions support healthy aging and well-being in autistic adults may be beneficial, and more research is needed in this area. Future research would benefit from a more comprehensive investigation into the quality, frequency, and meaning connected to online versus in-person social interactions and friendships, and important mechanisms supporting the development of these social connections. Because the connection between loneliness and an unmet need to belong is associated with suicidal ideation in autistic adults (Camm-Crosbie et al., 2019 ; Dow et al., 2021 ; Pelton et al., 2020 ), a specific focus on the impact of online and in-person social connections on mental health is needed.
While many participants reported no barriers to participation during the study week, some participants noted additional barriers of transportation, expense, and weather, as well as lack of motivation, energy, or people to do things with as interfering with social participation. At times, as Renee noted, it was a combination of factors,
Like if I had, if I had more friends like I would probably do more; [if] people were asking me, ‘Hey you wanna go do blah blah blah?’ I probably would. But I don’t really have any like, real friends right now. And I get exhausted from having to work.
Mental health, sensory, and organizational challenges were also reported as barriers to planned or desired activities during the study week. More research is needed to further examine how different types of barriers can be addressed to support a full range of social participation in autistic adults.
The current study suggests considerations of well-being and feelings of belonging in autistic adults should not be limited to measures of the number and quality of friendships alone. Rather, as researchers and clinicians, we may need to change the questions we are asking regarding the range of types of connections with others and community contexts that collectively contribute to social participation. As autistic adults navigate social experiences, the current study found evidence of individuals using a variety of in-person and online community contexts to intentionally practice and improve their social participation skills. In addition, current findings support autistic adults used specific apps to facilitate in-person meet ups, at times merging the preference for online communication with the desire for in-person connection. These results suggest exploring new ways to tailor interventions to support the range of desired social participation preferences of autistic adults. These findings may be a first step in research on the role of the range of social connections and healthy aging or well-being in autistic adults.
Acknowledgments
The authors would like to thank Laura Klinger, Ph.D. and The University of North Carolina at Chapel Hill TEACCH Autism Program’s research team for their feedback on an early draft of this manuscript. This paper was presented at the 20th annual National Council on Rehabilitation Education Conference (NCRE), July 17, 2020. This study was made possible through funding from The National Institute of Disability, Independent Living, and Rehabilitation Research (#90SFGE0008-01-00). Assistance for this project was also provided by the UNC Intellectual and Developmental Disabilities Research Center (NICHD; P50 HD103573; PI: Joseph Piven). The data management aspects of the project described was supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number UL1TR002489. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Author Contributions
Dara Chan contributed to the study conception and design. Material preparation and data collection were performed by all authors. Dara Chan and Julie Doran completed the data analysis and contributed to the manuscript writing. Osly Galobardi aided in data collection, analysis and interpreting the results. The first draft of the manuscript was written by Dara Chan and Julie Doran. All authors read and approved the final manuscript.
Dara Chan has received primary support for this project from a Switzer Fellowship from The National Institute of Disability, Independent Living, and Rehabilitation Research (#90SFGE0008-01-00). Assistance for this project was also provided by the UNC Intellectual and Developmental Disabilities Research Center (NICHD; P50 HD103573; PI: Joseph Piven). The project described was also supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number UL1TR002489. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
- Achat H, Kawachi I, Levine S, Berkey C, Coackley E, Colditz G. Social networks, stress and health-related quality of life. Quality of Life Research. 1998; 7 (8):735–750. doi: 10.1023/A:1008837002431. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders. 5. APA; 2013. [ Google Scholar ]
- Ashida S. Differential associations of social support and social connectedness with structural features of social networks and the health status of older adults. Journal of Aging and Health. 2008; 20 (7):872–893. doi: 10.1177/0898264308324626. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Averill J. Matrix analysis as a complementary analytic strategy in qualitative inquiry. Qualitative Health Research. 2002; 12 (6):855–866. doi: 10.1177/104973230201200611. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Bagatell N. From cure to community: Transforming notions of autism. Journal of the Society for Psychological Anthropology. 2010; 38 (1):33–55. doi: 10.1111/j.1548-1352.2009.01080.x. [ CrossRef ] [ Google Scholar ]
- Baron-Cohen S. Editorial Perspective: Neurodiversity—a revolutionary concept for autism and psychiatry. Journal of Child Psychology and Psychiatry. 2017; 58 (6):744–747. doi: 10.1111/jcpp.12703. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Bauminger N, Shulman C, Agam G. Peer interaction and loneliness in high-functioning children with autism. Journal of Autism and Developmental Disorders. 2003; 33 (5):489–507. doi: 10.1023/a:1025827427901. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Bauminger N, Solomon M, Aviezer A, Heung K, Gazit L, Brown J, Rogers SJ. Children with autism and their friends: A multidimensional study of friendship in high-functioning autism spectrum disorder. Journal of Abnormal Child Psychology. 2008; 36 (2):135–150. doi: 10.1007/s10802-007-9156-x. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Brownlow C, Rosqvist H, O’Dell L. Exploring the potential for social networking among people with autism: challenging dominant ideas of ‘friendship’ Scandinavian Journal of Disability Research. 2015; 17 (2):188–193. doi: 10.1080/15017419.2013.859174. [ CrossRef ] [ Google Scholar ]
- Calder L, Hill V, Pellicano E. ‘Sometimes I want to play by myself’: Understanding what friendship means to children with autism in mainstream primary schools. Autism. 2012; 17 (3):296–316. doi: 10.1177/1362361312467866. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Camm-Crosbie L, Bradley L, Shaw R, Baron-Cohen S, Cassidy S. ‘People like me don’t get support’: Autistic adults’ experiences of support and treatment for mental health difficulties, self-injury and suicidality. Autism. 2019; 23 (6):1431–1441. doi: 10.1177/1362361318816053. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Causton-Theoharis J, Ashby C, Cosier M. Islands of loneliness: Exploring social interaction through the autobiographies of individuals with autism. Intellectual and Developmental Disabilities. 2009; 47 (2):84–96. doi: 10.1352/1934-9556-47.2.84. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Center for Disease Control and Prevention. (2020). Data & statistics on autism spectrum disorder . Retrieved April 3, 2020, from https://www.cdc.gov/ncbddd/autism/data.html
- Dow D, Morgan L, Hooker J, Michaels M, Joiner T, Woods J, Wetherby A. Anxiety, depression, and the interpersonal theory of suicide in a community sample of adults with autism spectrum disorder. Archives of Suicide Research. 2021; 25 (2):297–314. doi: 10.1080/13811118.2019.1678537. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Elmose M. Understanding loneliness and social relationships in autism: The reflections of autistic adults. Nordic Psychology. 2020; 72 (1):3–22. doi: 10.1080/19012276.2019.1625068. [ CrossRef ] [ Google Scholar ]
- Freeman SFN, Kasari C. Friendships in children with developmental disabilities. Early Education & Development. 1998; 9 (4):341–355. doi: 10.1207/s15566935eed0904_2. [ CrossRef ] [ Google Scholar ]
- Gotham K, Marvin A, Lounds Taylor J, Warren Z, Anderson C, Law P, Law J, Lipkin P. Characterizing the daily life, needs, and priorities of adults with autism spectrum disorder from interactive autism network data. Autism. 2015; 19 (7):794–804. doi: 10.1177/1362361315583818. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Hamilton A, Maietta R. Rapid turn around qualitative research. Research Talk, Inc.; 2017. [ Google Scholar ]
- Henniger NA, Taylor JL. Outcomes in adults with autism spectrum disorders: A historical perspective. Autism. 2012; 17 (1):103–116. doi: 10.1177/1362361312441266. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Herrick, S., Datti, P. (2020). Neuro-competence: A multicultural counseling competence model for autism spectrum disorder . The 20th annual National Council on Rehabilitation Education Conference, Online
- Howlin P, Taylor JL. Addressing the need for high quality research in autism in adulthood. Autism. 2015; 19 (7):771–773. doi: 10.1177/1362361315595582. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Hsieh HF, Shannon S. Three approaches to qualitative content analysis. Qualitative Health Research. 2005; 15 (9):1277–1288. doi: 10.1177/1049732305276687. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Hwang Y, Foley K, Troller J. Aging well on the autism spectrum: the perspectives of autistic adults and carers. International Psychogeriatrics. 2017; 29 (12):2033–2046. doi: 10.1017/S1041610217001521. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Kasari C, Locke J, Gulsrud A, Rotheram-Fuller E. Social networks and friendships at school: Comparing children with and without ASD. Journal of Autism and Developmental Disorders. 2011; 41 (5):533–544. doi: 10.1007/s10803-010-1076-x. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Kelly M, Duff H, Kelly S, McHugh Power J, Brennan S, Lawlor B, Loughrey D. The impact of social activities, social networks, social support and social relationships on the cognitive functioning of healthy older adults: A systematic review. Systematic Reviews. 2017 doi: 10.1186/s13643-017-0632-2. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Kirby A, Baranek G, Fox L. Longitudinal predictors of outcomes for adults with autism spectrum disorder: Systematic review. OTJR: Occupation, Participation and Health. 2016; 36 (2):55–64. doi: 10.1177/1539449216650182. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Kuo M, Orsmond G, Cohn E, Coster W. Friendship characteristics and activity patterns of adolescents with an autism spectrum disorder. Autism. 2013; 17 (4):481–500. doi: 10.1177/1362361311416380. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Lam G, Holden E, Fitzpatrick M, Raffaele Mendez L, Berman K. “Different but connected”: Participatory action research using photovoice to explore well-being in autistic young adults. Autism. 2020; 24 (5):1246–1259. doi: 10.1177/1362361319898. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Levy A, Perry A. Outcomes in adolescents and adults with autism: A review of the literature. Research in Autism Spectrum Disorders. 2011; 5 (4):1271–1282. doi: 10.1016/j.rasd.2011.01.023. [ CrossRef ] [ Google Scholar ]
- Locke J, Ishijima E, Kasari C, London N. Loneliness, friendship quality and the social networks of adolescents with high-functioning autism in an inclusive school setting. Journal of Research in Special Education Needs. 2010; 10 (2):74–81. doi: 10.1111/j.1471-3802.2010.01148.x. [ CrossRef ] [ Google Scholar ]
- Maenner MJ, Smith LE, Hong J, Makuch R, Greenberg JS, Malick MR. Evaluation of an activities of daily living scale for adolescents and adults with developmental disabilities. Disability and Health Journal. 2013; 6 (1):8–17. doi: 10.1016/j.dhjo.2012.08.005. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Mazurek M. Social media use among adults with autism spectrum disorders. Computers in Human Behavior. 2013; 29 (4):1709–1714. doi: 10.1016/j.chb.2013.02.004. [ CrossRef ] [ Google Scholar ]
- Mazurek M. Loneliness, friendship, and well-being in adults with autism spectrum disorders. Autism. 2014; 18 (3):223–232. doi: 10.1177/1362361312474121. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Mazurek M, Wenstrup C. Television, video game and social media use among children with ASD and typically developing siblings. Journal of Autism and Developmental Disorders. 2013; 43 (6):1258–1271. doi: 10.1007/s10803-012-1659-9. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- McCollum M, LaVesser P, Berg C. Participation in daily activities of young adults with high functioning autism spectrum disorder. Journal of Autism and Developmental Disorders. 2016; 46 (3):987–997. doi: 10.1007/s10803-015-2642-z. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- McConachie H, Wilson C, Mason D, Garland D, Parr J, Rattazzi A, Rodgers J, Skevington S, Uljarevic M, Magiati I. What is important in measuring quality of life? Reflections by autistic adults in four countries. Autism in Adulthood. 2020; 2 (1):4–12. doi: 10.1089/aut.2019.0008. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Mehling M, Tasse M. Empirically derived model of social outcomes and predictors for adults with ASD. Intellectual and Developmental Disabilities. 2014; 52 (4):282–295. doi: 10.1352/1934-9556-52.4.282. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Michael Y, Colditz G, Coakley E, Kawachi I. Health behaviors, social networks, and healthy aging: Cross-sectional evidence from the Nurses’ Health Study. Quality of Life Research. 1999; 8 (8):711–722. doi: 10.1023/a:1008949428041. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Milton D, Sims T. How is a sense of well-being and belonging constructed in the accounts of autistic adults? Disability & Society. 2016; 31 (4):520–534. doi: 10.1080/09687599.2016.1186529. [ CrossRef ] [ Google Scholar ]
- Morrison K, DeBrabander K, Jones D, Faso D, Ackerman R, Sasson N. Outcomes of real world social interaction for autistic adults paired with autistic compared to typically developing partners. Autism. 2020; 24 (5):1067–1080. doi: 10.1177/1362361319892701. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Muller E, Schuler A, Yates G. Social challenges and supports from the perspective of individuals with Asperger syndrome and other autism spectrum disabilities. Autism. 2008; 12 (2):173–190. doi: 10.1177/1362361307086664. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Myers E, Davis BE, Stobbe G, Bjornson K. Community and social participation among individuals with autism spectrum disorder transitioning to adulthood. Journal of Autism and Developmental Disorders. 2015; 45 (8):2373–2381. doi: 10.1007/s10803-015-2403-z. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Orsmond G, Shattuck P, Cooper B, Sterzing P, Anderson K. Social participation among young adults with an autism spectrum disorder. Journal of Autism and Developmental Disorders. 2013; 43 (11):2710–2719. doi: 10.1007/s10803-013-1833-8. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Orsmond G, Wyngaarden Krauss M, Mailick Seltzer M. Peer relationships and social and recreational activities among adolescents and adults with autism. Journal of Autism and Developmental Disorders. 2004; 34 (3):245–256. doi: 10.1023/b:jadd.0000029547.96610.df. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Parker J, Asher S. Friendship and friendship quality in middle childhood: Links with peer group acceptance and feelings of loneliness and social dissatisfaction. Developmental Psychology. 1993; 29 (4):611–621. doi: 10.1037/0012-1649.29.4.611. [ CrossRef ] [ Google Scholar ]
- Pelton M, Crawford H, Robetson A, Rodgers J, Baron-Cohen S, Cassidy S. Understanding suicide risk in autistic adults: Comparing the interpersonal theory of suicide in autistic and non-autistic samples. Journal of Autism and Developmental Disorders. 2020; 50 (10):3620–3637. doi: 10.1007/s10803-020-04393-8. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Peplau LA, Perlman D. Loneliness: A sourcebook of current theory, research and therapy. Wiley; 1982. [ Google Scholar ]
- Petrina N, Carter M, Stephenson J, Sweller N. Friendship satisfaction in children with autism spectrum disorder and nominated friends. Journal of Autism and Developmental Disorders. 2017; 47 (2):384–392. doi: 10.1007/s10803-016-2970-7. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Rotheram-Fuller E, Kasari C, Chamberlain B, Locke J. Social involvement of children with autism spectrum disorders in elementary school classrooms. Journal of Child Psychology and Psychiatry. 2010 doi: 10.1111/j.1469-7610.2010.02289.x. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Roux A, Shattuck P, Cooper B, Anderson K, Wagner M, Narendorf S. Postsecondary employment experiences among young adults with an autism spectrum disorder. Journal of American Academy of Child and Adolescent Psychiatry. 2013; 52 (9):931–939. doi: 10.1016/j.jaac.2013.05.019. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Rowley E, Chandler S, Baird G, Simonoff E, Pickles A, Loucas T, Charman T. The experience of friendship, victimization and bullying in children with an autism spectrum disorder: Associations with child characteristics and school placement. Research in Autism Spectrum Disorders. 2012; 6 (3):1126–1134. doi: 10.1016/j.rasd.2012.03.004. [ CrossRef ] [ Google Scholar ]
- Schalkwyk G, Marin C, Ortiz M, Rolison M, Qayyum Z, McPartland J, Lebowitz E, Volkmar F, Silverman W. Social media use, friendship quality, and the moderating role of anxiety in adolescents with autism spectrum disorder. Journal of Autism and Developmental Disorders. 2017; 47 (9):2805–2813. doi: 10.1007/s10803-017-3201-6. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Sedgewick F, Leppanen J, Tchanturia K. The friendship questionnaire, autism, and gender differences: A study revisited. Molecular Autism. 2019 doi: 10.1186/s13229-019-0295-z. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Steinhausen HC, Mohr Jensen C, Lauritsen MB. A systematic review and meta-analysis of the long-term overall outcome of autism spectrum disorders in adolescence and adulthood. Acta Psychiatrica Scandinavica. 2016; 133 (6):445–452. doi: 10.1111/acps.12559. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Sundberg M. Online gaming, loneliness and friendships among adolescents and adults with ASD. Computers in Human Behavior. 2018; 79 :105–110. doi: 10.1016/j.chb.2017.10.020. [ CrossRef ] [ Google Scholar ]
- Tint A, Maughan AL, Weiss JA. Community participation of youth with intellectual disability and autism spectrum disorder. Journal of Intellectual Disability Research. 2016; 61 (2):168–180. doi: 10.1111/jir.12311. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Tobin M, Drager K, Richardson L. A systematic review of social participation for adults with autism spectrum disorders: Support, social functioning, and quality of life. Research in Autism Spectrum Disorders. 2014; 8 (3):214–229. doi: 10.1016/j.rasd.2013.12.002. [ CrossRef ] [ Google Scholar ]
- Uchino B, Holt-Lunstad J, Uno D, Flinders J. Heterogeneity in the social networks of young and older adults: Prediction of mental health and cardiovascular reactivity during acute stress. Journal of Behavioral Medicine. 2001; 24 (4):361–382. doi: 10.1023/a:1010634902498. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Wong YI, Solomon PL. Community integration of persons with psychiatric disabilities in supportive independent housing: A conceptual model and methodological considerations. Mental Health Services Research. 2002; 4 (1):13–28. doi: 10.1023/A:1014093008857. [ PubMed ] [ CrossRef ] [ Google Scholar ]
- Wood L, Martin K, Christian H, Nathan A, Lauritsen C, Houghton S, Kawachi I, McCune S. The pet factor–companion animals as a conduit for getting to know people, friendship formation and social support. PloS one. 2015; 10 (4):e0122085. doi: 10.1371/journal.pone.0122085. [ PMC free article ] [ PubMed ] [ CrossRef ] [ Google Scholar ]

Helping Youth & Families Thrive
ATLAS programs help young people living with a chronic health condition thrive as they transition to adulthood; we also provide support for parents around this transition. Support ATLAS programs by donating to Jodie's Fund today!
About ATLAS
Adolescents Transitioning to Leadership and Success (ATLAS) offers a range of Duke-affiliated services developed to foster resilience and independence in adolescents and young adults with special healthcare needs. Each program aims to help youth thrive as they transition from childhood to adulthood. In addition, ATLAS strives to provide support for parents around this transition. If you have any questions about ATLAS programming, please e-mail [email protected] or call 919-385-0842.
Please note that to join any of our programs, you will need to speak to a staff member first to determine which program(s) are the best fit and sign a participation agreement. All programs are returning in person this fall, and a virtual option will be offered as well unless otherwise noted.
Monthly Programs
Leadership program.
A mentoring program in which middle school students and high school students with chronic health conditions and college student mentors also with chronic conditions meet monthly to share their experiences growing up with chronic illness and pursue leadership development and life success. This group also has a parent group and will continue to offer a virtual option.
In-person meetings are held on the first Thursday evening of the month from 5-8:30pm in the Duke University School of Nursing. Virtual meetings are held on the third Thursday of the month from 6-7:15 pm. Contact [email protected] for more information or complete the appropriate participant agreement to sign up:
- Under Age 18 ATLAS Leadership Participant Agreement
- Age 18 and up ATLAS Leadership Participant Agreement
In-person meeting dates and topics for 2024-25 program year:
- September 5th: Living as a Teen with a Chronic Health Condition
- October 3rd: After High School: College and the Workforce
- November 7th: Independence
- December 5th: Healthcare Transition, Pediatrics to Adult Medicine
- January 9th: Health & Wellness, Part 1
- February 6th: Health & Wellness, Part 2
- March 6th: Communication with Providers
- April 10th: Personal Relationships and Communication
- May 1st: Graduation
LEAP (Leadership, Experience, Advocacy, and Progress) Program
A peer support program where individuals between the ages of 18-28 who live with chronic health conditions meet regularly to share their experiences as they move towards independence and into adult healthcare. Meetings will be held the second Thursday of every other month. Please note that LEAP is a virtual group. Contact [email protected] for more information.
ATLASfit is a health and wellness program for young adults ages 18-30 with intellectual or developmental disabilities and their families. ATLASfit runs quarterly topic-specific month-long classes. This group also includes a parent group.
If you are interested in ATLASfit, please complete the participation agreement below. Please note that you must speak to an ATLASfit staff member to make sure it is a good fit before you can attend a meeting. Contact [email protected] for more information or complete the participant agreement to sign up:
ATLASfit Participant Agreement
Campference

Campference is a four-day overnight summer leadership program (part camp and part conference) for adolescents and young adults (ages 15-22) with chronic health conditions.
Summer 2024 Campference was held Thursday, July 25, to Sunday, July 28. Planning for Campference 2025 is in the works!
Check back later for 2025 dates and registration materials!
Jodie’s Prom

Jodie's Prom at Duke Children's—formerly known as the Duke Children's Prom—is held annually each spring for current and former Duke Children's Pediatric patients ages 12 and up. For more information, please email [email protected] .
Jodie's Prom was held April 20, 2024 in the atrium of Duke Children's Hospital. The theme was "All Around the World: Discover Your Potential."
More than 111 participants — pediatric patients and their family members — came together in the atrium of Duke Children’s Hospital Clinic to spend an evening taking a trip around the world. Participants had fun out on the dance floor and at the eight “stops” on the world tour: appetizers in Istanbul, Berlin and Addis Ababa; arts and crafts in Paris and Taipei; dessert in Mexico City, and glamour red carpet moments in Hollywood and Las Vegas.
Folks danced, laughed, and celebrated life. We were joined this year by more than 40 volunteers from across the Duke system – medical providers, administrative staff, and, most crucially, the Duke Men’s and Women’s Lacrosse teams who were instrumental in set-up, tear-down, and creating good vibes and an environment of acceptance.
Save the date: Jodie's Prom 2025 will be April 26th!

Donations & Sponsors
If you would like to support Prom and other ATLAS programs, please click here . If you have any questions or would like to discuss your gift, please contact Emily C. Espenshade, Director of Development for the Neurosciences & Behavioral Health, at [email protected] .
If you would prefer to send a donation by mail, please address a check to Duke University and list ATLAS Prom (Dr. Maslow) in the memo line. Please mail check to the following address:
Duke Health Development Attn: ATLAS / Emily Espenshade 300 West Morgan Street, Suite 1000 Durham, NC 27701
ATLAS programming is supported by the Pratt Family Foundation, the Duke Hospital Auxiliary and private donations.
Jodie's Prom are generously funded by the Meg’s Smile Foundation, the Duke Hospital Auxiliary, and private donations, and coordinated by the ATLAS Programs team.

IMAGES
COMMENTS
About the journal. Research in Autism Spectrum Disorders (RASD) publishes high quality empirical articles and reviews that contribute to a better understanding of Autism Spectrum Disorders (ASD) at all levels of description; genetic, neurobiological, cognitive, and behavioral. The primary focus of the journal is to …. View full aims & scope.
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by deficits in social communication and the presence of restricted interests and repetitive behaviors . ... Ongoing research continues to deepen our understanding of potential etiologic mechanisms in ASD, but currently no single unifying cause has been elucidated. ...
Prevalence figures that referred to 4.5 per 10,000 in the 1960s have been replaced by newer estimates suggesting that 1 in 59 children (16 per 1,000) present with an autism spectrum disorder (ASD) in 2014 . The widening of the definition of autism has undoubtedly contributed to the significant increase in the numbers of people being diagnosed.
Atom. RSS Feed. Autism spectrum disorders are a group of neurodevelopmental disorders that are characterized by impaired social interaction and communication skills, and are often accompanied by ...
Autism spectrum disorders (ASD) are a group of neurodevelopmental disorders that affect individuals' social interactions, communication skills, and behavioral patterns, with significant individual differences and complex etiology. This article reviews the definition and characteristics of ASD, epidemiological profile, early research and diagnostic history, etiological studies, advances in ...
Read the latest articles of Research in Autism Spectrum Disorders at ScienceDirect.com, Elsevier's leading platform of peer-reviewed scholarly literature.
Menon V, Andrade C, Thennarasu K. Polycystic ovarian syndrome and autism spectrum disorder in the offspring: Should the primary outcome have been different? Mol Psychiatry. 2019. https://doi.org ...
Maternal androgens and autism spectrum disorder in the MARBLES prospective cohort study. Lauren Granillo, Ana-Maria Iosif, Amanda Goodrich, Nathaniel W. Snyder, Rebecca J. Schmidt. Article 102054. View PDF.
Research and training in autism spectrum disorder to catalyze the next genomic and neuroscience revolutions. Mol Psychiatry. 2020. https://doi. ... and autism spectrum disorder in the offspring ...
Autism spectrum disorder (ASD) is a neurodevelopmental disorder that typically manifests in early childhood as impaired social communication and restricted, repetitive behaviors and falls on a spectrum ranging from mild to severe. 1 For example, some people with ASD are nonverbal or speak only in simple sentences, while others are verbally skilled but have problems with social communication ...
Autism Research is an international journal which publishes research relevant to Autism Spectrum Disorder (ASD) and closely related neurodevelopmental disorders. We focus on genetic, neurobiological, immunological, epidemiological and psychological mechanisms and how these influence developmental processes in ASD.
ARI works to advance the understanding of autism spectrum disorder by funding research and education on its causes and treatments. ... Learn more about the physical and behavioral symptoms associated with autism spectrum disorder. Read More. Screening & Assessment. Explore information, research and tools available for support with autism ...
The Stanford Autism and Developmental Disorders Research Program would like to thank the children, as well as their parents and families, for contributing to research. ... 11/14/2013: Stanford drug trial seeks participants with autism spectrum disorder. 8/13/2012: Stanford researchers investigate the emotional side of autism. 5/29/2012: ...
Children with autism spectrum disorder between the ages of 2 and 4 years 11 months are invited to participate. This study involves up to a 5 month time commitment. The participant must be willing to complete cognitive and behavioral assessments (such as IQ and language testing) and be able to either sleep (young children) or lie still in the ...
Autism spectrum disorder (ASD) refers to any one of a group of disorders with an onset typically occurring during the preschool years and characterized by varying but often marked difficulties in communication and social interaction. ... APA's Division 33 is dedicated to advancing psychological research, professional education, and clinical ...
A mind-reading puzzle: Autistic people are more efficient at a theory-of-mind task. Estefania Loza, Frédérique Amsellem, Tiziana Zalla, Ariane Cartigny, ... Baudouin Forgeot d′Arc. Article 102105. View PDF. Article preview. Previous vol/issue. Read the latest articles of Research in Autism Spectrum Disorders at ScienceDirect.com, Elsevier ...
Autism Spectrum Disorders (ASDs) are lifelong neurodevelopmental conditions with mostly unknown etiology that have a huge impact on affected individuals and their families, and are a major public health concern. Significant gaps exist in the knowledge of ASD frequency and its possible rising trend.
Abstract. Autism spectrum disorder (autism) is a heterogeneous group of neurodevelopmental conditions characterized by early childhood-onset impairments in communication and social interaction alongside restricted and repetitive behaviors and interests. This review summarizes recent developments in human genetics research in autism ...
Autism spectrum disorder (ASD) is a class of neurodevelopmental conditions with a large epidemiological and societal impact worldwide. ... Our UR summarizes research evidence on the genetics of ...
A $12.3 million award will support research out of UC Santa Cruz, UC San Francisco, and UC Berkeley. August 30, 2024. By Emily Cerf. Share ... (CIRM) will support a team of UC Santa Cruz researchers in exploring the genetic underpinnings of autism spectrum disorder (ASD) and investigating possible treatments, in collaboration with teams at UC ...
Autism spectrum disorder is a condition related to brain development that impacts how a person perceives and socializes with others, causing problems in social interaction and communication. The disorder also includes limited and repetitive patterns of behavior. The term "spectrum" in autism spectrum disorder refers to the wide range of ...
Some research suggests a higher prevalence of Autism Spectrum Disorder (ASD) among terrorist offenders in comparison to the general population. However, the literature does not achieve consistency in terms of an evidential and theoretical basis that individuals with ASD are especially susceptible to terrorism engagement.
Key Points. Question Does maternal folic acid and/or multivitamin supplement use before and/or during pregnancy increase the risk of autism spectrum disorder in offspring?. Findings In this case-control cohort study of 45 300 offspring, statistically significant associations between maternal vitamin supplement use before and/or during pregnancy and reduced risk of autism spectrum disorder in ...
Background/Objectives: Parental involvement is vital for the academic success and overall development of students, particularly those with Autism Spectrum Disorder (ASD), who face unique educational challenges. This study investigates the influence of parental involvement on the academic performance and school adjustment of students with ASD, focusing on the interplay of cultural identity and ...
This article suggests future directions for research aimed at improved understanding of the etiology and pathophysiology of autism spectrum disorder (ASD) as well as pharmacologic and psychosocial interventions for ASD across the lifespan. The past few years have witnessed unprecedented transformations in the understanding of ASD neurobiology ...
Autism spectrum disorder (ASD) is a developmental disorder that begins in early childhood and has been associated with several environmental and genetic factors. ... The effects of research ...
Yerys, B. E. et al. Attention deficit/hyperactivity disorder symptoms moderate cognition and behavior in children with autism spectrum disorders. Autism Res. 2 , 322-333 (2009).
The current understanding of autism among parents of children with Autism Spectrum Disorder (ASD) in Malaysia reflects a multifaceted perspective marked by various challenges including confusion, financial constraints, limited resources, and a shortage of trained special needs teachers and affordable centers.
Introduction. The diagnosis of individuals with autism spectrum disorder (ASD) has risen dramatically, from 1 in 150 8-year-olds in 2002 to 1 in 54 in 2016 (Center for Disease Control, 2020).While prevalence rates are most closely monitored in children, ASD is a lifelong disorder characterized by social and communication impairments as well as repeated and restricted patterns of behavior ...
Leadership Program. A mentoring program in which middle school students and high school students with chronic health conditions and college student mentors also with chronic conditions meet monthly to share their experiences growing up with chronic illness and pursue leadership development and life success.