Get science-backed answers as you write with Paperpal's Research feature

How to Write a Conclusion for Research Papers (with Examples)

The conclusion of a research paper is a crucial section that plays a significant role in the overall impact and effectiveness of your research paper. However, this is also the section that typically receives less attention compared to the introduction and the body of the paper. The conclusion serves to provide a concise summary of the key findings, their significance, their implications, and a sense of closure to the study. Discussing how can the findings be applied in real-world scenarios or inform policy, practice, or decision-making is especially valuable to practitioners and policymakers. The research paper conclusion also provides researchers with clear insights and valuable information for their own work, which they can then build on and contribute to the advancement of knowledge in the field.
The research paper conclusion should explain the significance of your findings within the broader context of your field. It restates how your results contribute to the existing body of knowledge and whether they confirm or challenge existing theories or hypotheses. Also, by identifying unanswered questions or areas requiring further investigation, your awareness of the broader research landscape can be demonstrated.
Remember to tailor the research paper conclusion to the specific needs and interests of your intended audience, which may include researchers, practitioners, policymakers, or a combination of these.
Table of Contents
What is a conclusion in a research paper, summarizing conclusion, editorial conclusion, externalizing conclusion, importance of a good research paper conclusion, how to write a conclusion for your research paper, research paper conclusion examples.
- How to write a research paper conclusion with Paperpal?
Frequently Asked Questions
A conclusion in a research paper is the final section where you summarize and wrap up your research, presenting the key findings and insights derived from your study. The research paper conclusion is not the place to introduce new information or data that was not discussed in the main body of the paper. When working on how to conclude a research paper, remember to stick to summarizing and interpreting existing content. The research paper conclusion serves the following purposes: 1
- Warn readers of the possible consequences of not attending to the problem.
- Recommend specific course(s) of action.
- Restate key ideas to drive home the ultimate point of your research paper.
- Provide a “take-home” message that you want the readers to remember about your study.

Types of conclusions for research papers
In research papers, the conclusion provides closure to the reader. The type of research paper conclusion you choose depends on the nature of your study, your goals, and your target audience. I provide you with three common types of conclusions:
A summarizing conclusion is the most common type of conclusion in research papers. It involves summarizing the main points, reiterating the research question, and restating the significance of the findings. This common type of research paper conclusion is used across different disciplines.
An editorial conclusion is less common but can be used in research papers that are focused on proposing or advocating for a particular viewpoint or policy. It involves presenting a strong editorial or opinion based on the research findings and offering recommendations or calls to action.
An externalizing conclusion is a type of conclusion that extends the research beyond the scope of the paper by suggesting potential future research directions or discussing the broader implications of the findings. This type of conclusion is often used in more theoretical or exploratory research papers.
Align your conclusion’s tone with the rest of your research paper. Start Writing with Paperpal Now!
The conclusion in a research paper serves several important purposes:
- Offers Implications and Recommendations : Your research paper conclusion is an excellent place to discuss the broader implications of your research and suggest potential areas for further study. It’s also an opportunity to offer practical recommendations based on your findings.
- Provides Closure : A good research paper conclusion provides a sense of closure to your paper. It should leave the reader with a feeling that they have reached the end of a well-structured and thought-provoking research project.
- Leaves a Lasting Impression : Writing a well-crafted research paper conclusion leaves a lasting impression on your readers. It’s your final opportunity to leave them with a new idea, a call to action, or a memorable quote.

Writing a strong conclusion for your research paper is essential to leave a lasting impression on your readers. Here’s a step-by-step process to help you create and know what to put in the conclusion of a research paper: 2
- Research Statement : Begin your research paper conclusion by restating your research statement. This reminds the reader of the main point you’ve been trying to prove throughout your paper. Keep it concise and clear.
- Key Points : Summarize the main arguments and key points you’ve made in your paper. Avoid introducing new information in the research paper conclusion. Instead, provide a concise overview of what you’ve discussed in the body of your paper.
- Address the Research Questions : If your research paper is based on specific research questions or hypotheses, briefly address whether you’ve answered them or achieved your research goals. Discuss the significance of your findings in this context.
- Significance : Highlight the importance of your research and its relevance in the broader context. Explain why your findings matter and how they contribute to the existing knowledge in your field.
- Implications : Explore the practical or theoretical implications of your research. How might your findings impact future research, policy, or real-world applications? Consider the “so what?” question.
- Future Research : Offer suggestions for future research in your area. What questions or aspects remain unanswered or warrant further investigation? This shows that your work opens the door for future exploration.
- Closing Thought : Conclude your research paper conclusion with a thought-provoking or memorable statement. This can leave a lasting impression on your readers and wrap up your paper effectively. Avoid introducing new information or arguments here.
- Proofread and Revise : Carefully proofread your conclusion for grammar, spelling, and clarity. Ensure that your ideas flow smoothly and that your conclusion is coherent and well-structured.
Write your research paper conclusion 2x faster with Paperpal. Try it now!
Remember that a well-crafted research paper conclusion is a reflection of the strength of your research and your ability to communicate its significance effectively. It should leave a lasting impression on your readers and tie together all the threads of your paper. Now you know how to start the conclusion of a research paper and what elements to include to make it impactful, let’s look at a research paper conclusion sample.

How to write a research paper conclusion with Paperpal?
A research paper conclusion is not just a summary of your study, but a synthesis of the key findings that ties the research together and places it in a broader context. A research paper conclusion should be concise, typically around one paragraph in length. However, some complex topics may require a longer conclusion to ensure the reader is left with a clear understanding of the study’s significance. Paperpal, an AI writing assistant trusted by over 800,000 academics globally, can help you write a well-structured conclusion for your research paper.
- Sign Up or Log In: Create a new Paperpal account or login with your details.
- Navigate to Features : Once logged in, head over to the features’ side navigation pane. Click on Templates and you’ll find a suite of generative AI features to help you write better, faster.
- Generate an outline: Under Templates, select ‘Outlines’. Choose ‘Research article’ as your document type.
- Select your section: Since you’re focusing on the conclusion, select this section when prompted.
- Choose your field of study: Identifying your field of study allows Paperpal to provide more targeted suggestions, ensuring the relevance of your conclusion to your specific area of research.
- Provide a brief description of your study: Enter details about your research topic and findings. This information helps Paperpal generate a tailored outline that aligns with your paper’s content.
- Generate the conclusion outline: After entering all necessary details, click on ‘generate’. Paperpal will then create a structured outline for your conclusion, to help you start writing and build upon the outline.
- Write your conclusion: Use the generated outline to build your conclusion. The outline serves as a guide, ensuring you cover all critical aspects of a strong conclusion, from summarizing key findings to highlighting the research’s implications.
- Refine and enhance: Paperpal’s ‘Make Academic’ feature can be particularly useful in the final stages. Select any paragraph of your conclusion and use this feature to elevate the academic tone, ensuring your writing is aligned to the academic journal standards.
By following these steps, Paperpal not only simplifies the process of writing a research paper conclusion but also ensures it is impactful, concise, and aligned with academic standards. Sign up with Paperpal today and write your research paper conclusion 2x faster .
The research paper conclusion is a crucial part of your paper as it provides the final opportunity to leave a strong impression on your readers. In the research paper conclusion, summarize the main points of your research paper by restating your research statement, highlighting the most important findings, addressing the research questions or objectives, explaining the broader context of the study, discussing the significance of your findings, providing recommendations if applicable, and emphasizing the takeaway message. The main purpose of the conclusion is to remind the reader of the main point or argument of your paper and to provide a clear and concise summary of the key findings and their implications. All these elements should feature on your list of what to put in the conclusion of a research paper to create a strong final statement for your work.
A strong conclusion is a critical component of a research paper, as it provides an opportunity to wrap up your arguments, reiterate your main points, and leave a lasting impression on your readers. Here are the key elements of a strong research paper conclusion: 1. Conciseness : A research paper conclusion should be concise and to the point. It should not introduce new information or ideas that were not discussed in the body of the paper. 2. Summarization : The research paper conclusion should be comprehensive enough to give the reader a clear understanding of the research’s main contributions. 3 . Relevance : Ensure that the information included in the research paper conclusion is directly relevant to the research paper’s main topic and objectives; avoid unnecessary details. 4 . Connection to the Introduction : A well-structured research paper conclusion often revisits the key points made in the introduction and shows how the research has addressed the initial questions or objectives. 5. Emphasis : Highlight the significance and implications of your research. Why is your study important? What are the broader implications or applications of your findings? 6 . Call to Action : Include a call to action or a recommendation for future research or action based on your findings.
The length of a research paper conclusion can vary depending on several factors, including the overall length of the paper, the complexity of the research, and the specific journal requirements. While there is no strict rule for the length of a conclusion, but it’s generally advisable to keep it relatively short. A typical research paper conclusion might be around 5-10% of the paper’s total length. For example, if your paper is 10 pages long, the conclusion might be roughly half a page to one page in length.
In general, you do not need to include citations in the research paper conclusion. Citations are typically reserved for the body of the paper to support your arguments and provide evidence for your claims. However, there may be some exceptions to this rule: 1. If you are drawing a direct quote or paraphrasing a specific source in your research paper conclusion, you should include a citation to give proper credit to the original author. 2. If your conclusion refers to or discusses specific research, data, or sources that are crucial to the overall argument, citations can be included to reinforce your conclusion’s validity.
The conclusion of a research paper serves several important purposes: 1. Summarize the Key Points 2. Reinforce the Main Argument 3. Provide Closure 4. Offer Insights or Implications 5. Engage the Reader. 6. Reflect on Limitations
Remember that the primary purpose of the research paper conclusion is to leave a lasting impression on the reader, reinforcing the key points and providing closure to your research. It’s often the last part of the paper that the reader will see, so it should be strong and well-crafted.
- Makar, G., Foltz, C., Lendner, M., & Vaccaro, A. R. (2018). How to write effective discussion and conclusion sections. Clinical spine surgery, 31(8), 345-346.
- Bunton, D. (2005). The structure of PhD conclusion chapters. Journal of English for academic purposes , 4 (3), 207-224.
Paperpal is a comprehensive AI writing toolkit that helps students and researchers achieve 2x the writing in half the time. It leverages 21+ years of STM experience and insights from millions of research articles to provide in-depth academic writing, language editing, and submission readiness support to help you write better, faster.
Get accurate academic translations, rewriting support, grammar checks, vocabulary suggestions, and generative AI assistance that delivers human precision at machine speed. Try for free or upgrade to Paperpal Prime starting at US$19 a month to access premium features, including consistency, plagiarism, and 30+ submission readiness checks to help you succeed.
Experience the future of academic writing – Sign up to Paperpal and start writing for free!
Related Reads:
- 5 Reasons for Rejection After Peer Review
- Ethical Research Practices For Research with Human Subjects
7 Ways to Improve Your Academic Writing Process
- Paraphrasing in Academic Writing: Answering Top Author Queries
Preflight For Editorial Desk: The Perfect Hybrid (AI + Human) Assistance Against Compromised Manuscripts
You may also like, how to write a high-quality conference paper, academic editing: how to self-edit academic text with..., measuring academic success: definition & strategies for excellence, phd qualifying exam: tips for success , ai in education: it’s time to change the..., is it ethical to use ai-generated abstracts without..., what are journal guidelines on using generative ai..., quillbot review: features, pricing, and free alternatives, what is an academic paper types and elements , should you use ai tools like chatgpt for....
When you choose to publish with PLOS, your research makes an impact. Make your work accessible to all, without restrictions, and accelerate scientific discovery with options like preprints and published peer review that make your work more Open.
- PLOS Biology
- PLOS Climate
- PLOS Complex Systems
- PLOS Computational Biology
- PLOS Digital Health
- PLOS Genetics
- PLOS Global Public Health
- PLOS Medicine
- PLOS Mental Health
- PLOS Neglected Tropical Diseases
- PLOS Pathogens
- PLOS Sustainability and Transformation
- PLOS Collections
- How to Write Discussions and Conclusions

The discussion section contains the results and outcomes of a study. An effective discussion informs readers what can be learned from your experiment and provides context for the results.
What makes an effective discussion?
When you’re ready to write your discussion, you’ve already introduced the purpose of your study and provided an in-depth description of the methodology. The discussion informs readers about the larger implications of your study based on the results. Highlighting these implications while not overstating the findings can be challenging, especially when you’re submitting to a journal that selects articles based on novelty or potential impact. Regardless of what journal you are submitting to, the discussion section always serves the same purpose: concluding what your study results actually mean.
A successful discussion section puts your findings in context. It should include:
- the results of your research,
- a discussion of related research, and
- a comparison between your results and initial hypothesis.
Tip: Not all journals share the same naming conventions.
You can apply the advice in this article to the conclusion, results or discussion sections of your manuscript.
Our Early Career Researcher community tells us that the conclusion is often considered the most difficult aspect of a manuscript to write. To help, this guide provides questions to ask yourself, a basic structure to model your discussion off of and examples from published manuscripts.

Questions to ask yourself:
- Was my hypothesis correct?
- If my hypothesis is partially correct or entirely different, what can be learned from the results?
- How do the conclusions reshape or add onto the existing knowledge in the field? What does previous research say about the topic?
- Why are the results important or relevant to your audience? Do they add further evidence to a scientific consensus or disprove prior studies?
- How can future research build on these observations? What are the key experiments that must be done?
- What is the “take-home” message you want your reader to leave with?
How to structure a discussion
Trying to fit a complete discussion into a single paragraph can add unnecessary stress to the writing process. If possible, you’ll want to give yourself two or three paragraphs to give the reader a comprehensive understanding of your study as a whole. Here’s one way to structure an effective discussion:

Writing Tips
While the above sections can help you brainstorm and structure your discussion, there are many common mistakes that writers revert to when having difficulties with their paper. Writing a discussion can be a delicate balance between summarizing your results, providing proper context for your research and avoiding introducing new information. Remember that your paper should be both confident and honest about the results!

- Read the journal’s guidelines on the discussion and conclusion sections. If possible, learn about the guidelines before writing the discussion to ensure you’re writing to meet their expectations.
- Begin with a clear statement of the principal findings. This will reinforce the main take-away for the reader and set up the rest of the discussion.
- Explain why the outcomes of your study are important to the reader. Discuss the implications of your findings realistically based on previous literature, highlighting both the strengths and limitations of the research.
- State whether the results prove or disprove your hypothesis. If your hypothesis was disproved, what might be the reasons?
- Introduce new or expanded ways to think about the research question. Indicate what next steps can be taken to further pursue any unresolved questions.
- If dealing with a contemporary or ongoing problem, such as climate change, discuss possible consequences if the problem is avoided.
- Be concise. Adding unnecessary detail can distract from the main findings.

Don’t
- Rewrite your abstract. Statements with “we investigated” or “we studied” generally do not belong in the discussion.
- Include new arguments or evidence not previously discussed. Necessary information and evidence should be introduced in the main body of the paper.
- Apologize. Even if your research contains significant limitations, don’t undermine your authority by including statements that doubt your methodology or execution.
- Shy away from speaking on limitations or negative results. Including limitations and negative results will give readers a complete understanding of the presented research. Potential limitations include sources of potential bias, threats to internal or external validity, barriers to implementing an intervention and other issues inherent to the study design.
- Overstate the importance of your findings. Making grand statements about how a study will fully resolve large questions can lead readers to doubt the success of the research.
Snippets of Effective Discussions:
Consumer-based actions to reduce plastic pollution in rivers: A multi-criteria decision analysis approach
Identifying reliable indicators of fitness in polar bears
- How to Write a Great Title
- How to Write an Abstract
- How to Write Your Methods
- How to Report Statistics
- How to Edit Your Work
The contents of the Peer Review Center are also available as a live, interactive training session, complete with slides, talking points, and activities. …
The contents of the Writing Center are also available as a live, interactive training session, complete with slides, talking points, and activities. …
There’s a lot to consider when deciding where to submit your work. Learn how to choose a journal that will help your study reach its audience, while reflecting your values as a researcher…
How to write a strong conclusion for your research paper
Last updated
17 February 2024
Reviewed by
Writing a research paper is a chance to share your knowledge and hypothesis. It's an opportunity to demonstrate your many hours of research and prove your ability to write convincingly.
Ideally, by the end of your research paper, you'll have brought your readers on a journey to reach the conclusions you've pre-determined. However, if you don't stick the landing with a good conclusion, you'll risk losing your reader’s trust.
Writing a strong conclusion for your research paper involves a few important steps, including restating the thesis and summing up everything properly.
Find out what to include and what to avoid, so you can effectively demonstrate your understanding of the topic and prove your expertise.
- Why is a good conclusion important?
A good conclusion can cement your paper in the reader’s mind. Making a strong impression in your introduction can draw your readers in, but it's the conclusion that will inspire them.
- What to include in a research paper conclusion
There are a few specifics you should include in your research paper conclusion. Offer your readers some sense of urgency or consequence by pointing out why they should care about the topic you have covered. Discuss any common problems associated with your topic and provide suggestions as to how these problems can be solved or addressed.
The conclusion should include a restatement of your initial thesis. Thesis statements are strengthened after you’ve presented supporting evidence (as you will have done in the paper), so make a point to reintroduce it at the end.
Finally, recap the main points of your research paper, highlighting the key takeaways you want readers to remember. If you've made multiple points throughout the paper, refer to the ones with the strongest supporting evidence.
- Steps for writing a research paper conclusion
Many writers find the conclusion the most challenging part of any research project . By following these three steps, you'll be prepared to write a conclusion that is effective and concise.
- Step 1: Restate the problem
Always begin by restating the research problem in the conclusion of a research paper. This serves to remind the reader of your hypothesis and refresh them on the main point of the paper.
When restating the problem, take care to avoid using exactly the same words you employed earlier in the paper.
- Step 2: Sum up the paper
After you've restated the problem, sum up the paper by revealing your overall findings. The method for this differs slightly, depending on whether you're crafting an argumentative paper or an empirical paper.
Argumentative paper: Restate your thesis and arguments
Argumentative papers involve introducing a thesis statement early on. In crafting the conclusion for an argumentative paper, always restate the thesis, outlining the way you've developed it throughout the entire paper.
It might be appropriate to mention any counterarguments in the conclusion, so you can demonstrate how your thesis is correct or how the data best supports your main points.
Empirical paper: Summarize research findings
Empirical papers break down a series of research questions. In your conclusion, discuss the findings your research revealed, including any information that surprised you.
Be clear about the conclusions you reached, and explain whether or not you expected to arrive at these particular ones.
- Step 3: Discuss the implications of your research
Argumentative papers and empirical papers also differ in this part of a research paper conclusion. Here are some tips on crafting conclusions for argumentative and empirical papers.
Argumentative paper: Powerful closing statement
In an argumentative paper, you'll have spent a great deal of time expressing the opinions you formed after doing a significant amount of research. Make a strong closing statement in your argumentative paper's conclusion to share the significance of your work.
You can outline the next steps through a bold call to action, or restate how powerful your ideas turned out to be.
Empirical paper: Directions for future research
Empirical papers are broader in scope. They usually cover a variety of aspects and can include several points of view.
To write a good conclusion for an empirical paper, suggest the type of research that could be done in the future, including methods for further investigation or outlining ways other researchers might proceed.
If you feel your research had any limitations, even if they were outside your control, you could mention these in your conclusion.
After you finish outlining your conclusion, ask someone to read it and offer feedback. In any research project you're especially close to, it can be hard to identify problem areas. Having a close friend or someone whose opinion you value read the research paper and provide honest feedback can be invaluable. Take note of any suggested edits and consider incorporating them into your paper if they make sense.
- Things to avoid in a research paper conclusion
Keep these aspects to avoid in mind as you're writing your conclusion and refer to them after you've created an outline.
Dry summary
Writing a memorable, succinct conclusion is arguably more important than a strong introduction. Take care to avoid just rephrasing your main points, and don't fall into the trap of repeating dry facts or citations.
You can provide a new perspective for your readers to think about or contextualize your research. Either way, make the conclusion vibrant and interesting, rather than a rote recitation of your research paper’s highlights.
Clichéd or generic phrasing
Your research paper conclusion should feel fresh and inspiring. Avoid generic phrases like "to sum up" or "in conclusion." These phrases tend to be overused, especially in an academic context and might turn your readers off.
The conclusion also isn't the time to introduce colloquial phrases or informal language. Retain a professional, confident tone consistent throughout your paper’s conclusion so it feels exciting and bold.
New data or evidence
While you should present strong data throughout your paper, the conclusion isn't the place to introduce new evidence. This is because readers are engaged in actively learning as they read through the body of your paper.
By the time they reach the conclusion, they will have formed an opinion one way or the other (hopefully in your favor!). Introducing new evidence in the conclusion will only serve to surprise or frustrate your reader.
Ignoring contradictory evidence
If your research reveals contradictory evidence, don't ignore it in the conclusion. This will damage your credibility as an expert and might even serve to highlight the contradictions.
Be as transparent as possible and admit to any shortcomings in your research, but don't dwell on them for too long.
Ambiguous or unclear resolutions
The point of a research paper conclusion is to provide closure and bring all your ideas together. You should wrap up any arguments you introduced in the paper and tie up any loose ends, while demonstrating why your research and data are strong.
Use direct language in your conclusion and avoid ambiguity. Even if some of the data and sources you cite are inconclusive or contradictory, note this in your conclusion to come across as confident and trustworthy.
- Examples of research paper conclusions
Your research paper should provide a compelling close to the paper as a whole, highlighting your research and hard work. While the conclusion should represent your unique style, these examples offer a starting point:
Ultimately, the data we examined all point to the same conclusion: Encouraging a good work-life balance improves employee productivity and benefits the company overall. The research suggests that when employees feel their personal lives are valued and respected by their employers, they are more likely to be productive when at work. In addition, company turnover tends to be reduced when employees have a balance between their personal and professional lives. While additional research is required to establish ways companies can support employees in creating a stronger work-life balance, it's clear the need is there.
Social media is a primary method of communication among young people. As we've seen in the data presented, most young people in high school use a variety of social media applications at least every hour, including Instagram and Facebook. While social media is an avenue for connection with peers, research increasingly suggests that social media use correlates with body image issues. Young girls with lower self-esteem tend to use social media more often than those who don't log onto social media apps every day. As new applications continue to gain popularity, and as more high school students are given smartphones, more research will be required to measure the effects of prolonged social media use.
What are the different kinds of research paper conclusions?
There are no formal types of research paper conclusions. Ultimately, the conclusion depends on the outline of your paper and the type of research you’re presenting. While some experts note that research papers can end with a new perspective or commentary, most papers should conclude with a combination of both. The most important aspect of a good research paper conclusion is that it accurately represents the body of the paper.
Can I present new arguments in my research paper conclusion?
Research paper conclusions are not the place to introduce new data or arguments. The body of your paper is where you should share research and insights, where the reader is actively absorbing the content. By the time a reader reaches the conclusion of the research paper, they should have formed their opinion. Introducing new arguments in the conclusion can take a reader by surprise, and not in a positive way. It might also serve to frustrate readers.
How long should a research paper conclusion be?
There's no set length for a research paper conclusion. However, it's a good idea not to run on too long, since conclusions are supposed to be succinct. A good rule of thumb is to keep your conclusion around 5 to 10 percent of the paper's total length. If your paper is 10 pages, try to keep your conclusion under one page.
What should I include in a research paper conclusion?
A good research paper conclusion should always include a sense of urgency, so the reader can see how and why the topic should matter to them. You can also note some recommended actions to help fix the problem and some obstacles they might encounter. A conclusion should also remind the reader of the thesis statement, along with the main points you covered in the paper. At the end of the conclusion, add a powerful closing statement that helps cement the paper in the mind of the reader.
Should you be using a customer insights hub?
Do you want to discover previous research faster?
Do you share your research findings with others?
Do you analyze research data?
Start for free today, add your research, and get to key insights faster
Editor’s picks
Last updated: 11 January 2024
Last updated: 15 January 2024
Last updated: 17 January 2024
Last updated: 25 November 2023
Last updated: 12 May 2023
Last updated: 30 April 2024
Last updated: 13 May 2024
Latest articles
Related topics, .css-je19u9{-webkit-align-items:flex-end;-webkit-box-align:flex-end;-ms-flex-align:flex-end;align-items:flex-end;display:-webkit-box;display:-webkit-flex;display:-ms-flexbox;display:flex;-webkit-flex-direction:row;-ms-flex-direction:row;flex-direction:row;-webkit-box-flex-wrap:wrap;-webkit-flex-wrap:wrap;-ms-flex-wrap:wrap;flex-wrap:wrap;-webkit-box-pack:center;-ms-flex-pack:center;-webkit-justify-content:center;justify-content:center;row-gap:0;text-align:center;max-width:671px;}@media (max-width: 1079px){.css-je19u9{max-width:400px;}.css-je19u9>span{white-space:pre;}}@media (max-width: 799px){.css-je19u9{max-width:400px;}.css-je19u9>span{white-space:pre;}} decide what to .css-1kiodld{max-height:56px;display:-webkit-box;display:-webkit-flex;display:-ms-flexbox;display:flex;-webkit-align-items:center;-webkit-box-align:center;-ms-flex-align:center;align-items:center;}@media (max-width: 1079px){.css-1kiodld{display:none;}} build next, decide what to build next.

Users report unexpectedly high data usage, especially during streaming sessions.

Users find it hard to navigate from the home page to relevant playlists in the app.

It would be great to have a sleep timer feature, especially for bedtime listening.

I need better filters to find the songs or artists I’m looking for.
Log in or sign up
Get started for free
- Link to facebook
- Link to linkedin
- Link to twitter
- Link to youtube
- Writing Tips
How to Write a Conclusion for a Research Paper

3-minute read
- 29th August 2023
If you’re writing a research paper, the conclusion is your opportunity to summarize your findings and leave a lasting impression on your readers. In this post, we’ll take you through how to write an effective conclusion for a research paper and how you can:
· Reword your thesis statement
· Highlight the significance of your research
· Discuss limitations
· Connect to the introduction
· End with a thought-provoking statement
Rewording Your Thesis Statement
Begin your conclusion by restating your thesis statement in a way that is slightly different from the wording used in the introduction. Avoid presenting new information or evidence in your conclusion. Just summarize the main points and arguments of your essay and keep this part as concise as possible. Remember that you’ve already covered the in-depth analyses and investigations in the main body paragraphs of your essay, so it’s not necessary to restate these details in the conclusion.
Find this useful?
Subscribe to our newsletter and get writing tips from our editors straight to your inbox.
Highlighting the Significance of Your Research
The conclusion is a good place to emphasize the implications of your research . Avoid ambiguous or vague language such as “I think” or “maybe,” which could weaken your position. Clearly explain why your research is significant and how it contributes to the broader field of study.
Here’s an example from a (fictional) study on the impact of social media on mental health:
Discussing Limitations
Although it’s important to emphasize the significance of your study, you can also use the conclusion to briefly address any limitations you discovered while conducting your research, such as time constraints or a shortage of resources. Doing this demonstrates a balanced and honest approach to your research.
Connecting to the Introduction
In your conclusion, you can circle back to your introduction , perhaps by referring to a quote or anecdote you discussed earlier. If you end your paper on a similar note to how you began it, you will create a sense of cohesion for the reader and remind them of the meaning and significance of your research.
Ending With a Thought-Provoking Statement
Consider ending your paper with a thought-provoking and memorable statement that relates to the impact of your research questions or hypothesis. This statement can be a call to action, a philosophical question, or a prediction for the future (positive or negative). Here’s an example that uses the same topic as above (social media and mental health):
Expert Proofreading Services
Ensure that your essay ends on a high note by having our experts proofread your research paper. Our team has experience with a wide variety of academic fields and subjects and can help make your paper stand out from the crowd – get started today and see the difference it can make in your work.
Share this article:
Post A New Comment
Got content that needs a quick turnaround? Let us polish your work. Explore our editorial business services.
9-minute read
How to Use Infographics to Boost Your Presentation
Is your content getting noticed? Capturing and maintaining an audience’s attention is a challenge when...
8-minute read
Why Interactive PDFs Are Better for Engagement
Are you looking to enhance engagement and captivate your audience through your professional documents? Interactive...
7-minute read
Seven Key Strategies for Voice Search Optimization
Voice search optimization is rapidly shaping the digital landscape, requiring content professionals to adapt their...
4-minute read
Five Creative Ways to Showcase Your Digital Portfolio
Are you a creative freelancer looking to make a lasting impression on potential clients or...
How to Ace Slack Messaging for Contractors and Freelancers
Effective professional communication is an important skill for contractors and freelancers navigating remote work environments....
How to Insert a Text Box in a Google Doc
Google Docs is a powerful collaborative tool, and mastering its features can significantly enhance your...
Make sure your writing is the best it can be with our expert English proofreading and editing.
- Privacy Policy
Home » Research Summary – Structure, Examples and Writing Guide
Research Summary – Structure, Examples and Writing Guide
Table of Contents

Research Summary
Definition:
A research summary is a brief and concise overview of a research project or study that highlights its key findings, main points, and conclusions. It typically includes a description of the research problem, the research methods used, the results obtained, and the implications or significance of the findings. It is often used as a tool to quickly communicate the main findings of a study to other researchers, stakeholders, or decision-makers.
Structure of Research Summary
The Structure of a Research Summary typically include:
- Introduction : This section provides a brief background of the research problem or question, explains the purpose of the study, and outlines the research objectives.
- Methodology : This section explains the research design, methods, and procedures used to conduct the study. It describes the sample size, data collection methods, and data analysis techniques.
- Results : This section presents the main findings of the study, including statistical analysis if applicable. It may include tables, charts, or graphs to visually represent the data.
- Discussion : This section interprets the results and explains their implications. It discusses the significance of the findings, compares them to previous research, and identifies any limitations or future directions for research.
- Conclusion : This section summarizes the main points of the research and provides a conclusion based on the findings. It may also suggest implications for future research or practical applications of the results.
- References : This section lists the sources cited in the research summary, following the appropriate citation style.
How to Write Research Summary
Here are the steps you can follow to write a research summary:
- Read the research article or study thoroughly: To write a summary, you must understand the research article or study you are summarizing. Therefore, read the article or study carefully to understand its purpose, research design, methodology, results, and conclusions.
- Identify the main points : Once you have read the research article or study, identify the main points, key findings, and research question. You can highlight or take notes of the essential points and findings to use as a reference when writing your summary.
- Write the introduction: Start your summary by introducing the research problem, research question, and purpose of the study. Briefly explain why the research is important and its significance.
- Summarize the methodology : In this section, summarize the research design, methods, and procedures used to conduct the study. Explain the sample size, data collection methods, and data analysis techniques.
- Present the results: Summarize the main findings of the study. Use tables, charts, or graphs to visually represent the data if necessary.
- Interpret the results: In this section, interpret the results and explain their implications. Discuss the significance of the findings, compare them to previous research, and identify any limitations or future directions for research.
- Conclude the summary : Summarize the main points of the research and provide a conclusion based on the findings. Suggest implications for future research or practical applications of the results.
- Revise and edit : Once you have written the summary, revise and edit it to ensure that it is clear, concise, and free of errors. Make sure that your summary accurately represents the research article or study.
- Add references: Include a list of references cited in the research summary, following the appropriate citation style.
Example of Research Summary
Here is an example of a research summary:
Title: The Effects of Yoga on Mental Health: A Meta-Analysis
Introduction: This meta-analysis examines the effects of yoga on mental health. The study aimed to investigate whether yoga practice can improve mental health outcomes such as anxiety, depression, stress, and quality of life.
Methodology : The study analyzed data from 14 randomized controlled trials that investigated the effects of yoga on mental health outcomes. The sample included a total of 862 participants. The yoga interventions varied in length and frequency, ranging from four to twelve weeks, with sessions lasting from 45 to 90 minutes.
Results : The meta-analysis found that yoga practice significantly improved mental health outcomes. Participants who practiced yoga showed a significant reduction in anxiety and depression symptoms, as well as stress levels. Quality of life also improved in those who practiced yoga.
Discussion : The findings of this study suggest that yoga can be an effective intervention for improving mental health outcomes. The study supports the growing body of evidence that suggests that yoga can have a positive impact on mental health. Limitations of the study include the variability of the yoga interventions, which may affect the generalizability of the findings.
Conclusion : Overall, the findings of this meta-analysis support the use of yoga as an effective intervention for improving mental health outcomes. Further research is needed to determine the optimal length and frequency of yoga interventions for different populations.
References :
- Cramer, H., Lauche, R., Langhorst, J., Dobos, G., & Berger, B. (2013). Yoga for depression: a systematic review and meta-analysis. Depression and anxiety, 30(11), 1068-1083.
- Khalsa, S. B. (2004). Yoga as a therapeutic intervention: a bibliometric analysis of published research studies. Indian journal of physiology and pharmacology, 48(3), 269-285.
- Ross, A., & Thomas, S. (2010). The health benefits of yoga and exercise: a review of comparison studies. The Journal of Alternative and Complementary Medicine, 16(1), 3-12.
Purpose of Research Summary
The purpose of a research summary is to provide a brief overview of a research project or study, including its main points, findings, and conclusions. The summary allows readers to quickly understand the essential aspects of the research without having to read the entire article or study.
Research summaries serve several purposes, including:
- Facilitating comprehension: A research summary allows readers to quickly understand the main points and findings of a research project or study without having to read the entire article or study. This makes it easier for readers to comprehend the research and its significance.
- Communicating research findings: Research summaries are often used to communicate research findings to a wider audience, such as policymakers, practitioners, or the general public. The summary presents the essential aspects of the research in a clear and concise manner, making it easier for non-experts to understand.
- Supporting decision-making: Research summaries can be used to support decision-making processes by providing a summary of the research evidence on a particular topic. This information can be used by policymakers or practitioners to make informed decisions about interventions, programs, or policies.
- Saving time: Research summaries save time for researchers, practitioners, policymakers, and other stakeholders who need to review multiple research studies. Rather than having to read the entire article or study, they can quickly review the summary to determine whether the research is relevant to their needs.
Characteristics of Research Summary
The following are some of the key characteristics of a research summary:
- Concise : A research summary should be brief and to the point, providing a clear and concise overview of the main points of the research.
- Objective : A research summary should be written in an objective tone, presenting the research findings without bias or personal opinion.
- Comprehensive : A research summary should cover all the essential aspects of the research, including the research question, methodology, results, and conclusions.
- Accurate : A research summary should accurately reflect the key findings and conclusions of the research.
- Clear and well-organized: A research summary should be easy to read and understand, with a clear structure and logical flow.
- Relevant : A research summary should focus on the most important and relevant aspects of the research, highlighting the key findings and their implications.
- Audience-specific: A research summary should be tailored to the intended audience, using language and terminology that is appropriate and accessible to the reader.
- Citations : A research summary should include citations to the original research articles or studies, allowing readers to access the full text of the research if desired.
When to write Research Summary
Here are some situations when it may be appropriate to write a research summary:
- Proposal stage: A research summary can be included in a research proposal to provide a brief overview of the research aims, objectives, methodology, and expected outcomes.
- Conference presentation: A research summary can be prepared for a conference presentation to summarize the main findings of a study or research project.
- Journal submission: Many academic journals require authors to submit a research summary along with their research article or study. The summary provides a brief overview of the study’s main points, findings, and conclusions and helps readers quickly understand the research.
- Funding application: A research summary can be included in a funding application to provide a brief summary of the research aims, objectives, and expected outcomes.
- Policy brief: A research summary can be prepared as a policy brief to communicate research findings to policymakers or stakeholders in a concise and accessible manner.
Advantages of Research Summary
Research summaries offer several advantages, including:
- Time-saving: A research summary saves time for readers who need to understand the key findings and conclusions of a research project quickly. Rather than reading the entire research article or study, readers can quickly review the summary to determine whether the research is relevant to their needs.
- Clarity and accessibility: A research summary provides a clear and accessible overview of the research project’s main points, making it easier for readers to understand the research without having to be experts in the field.
- Improved comprehension: A research summary helps readers comprehend the research by providing a brief and focused overview of the key findings and conclusions, making it easier to understand the research and its significance.
- Enhanced communication: Research summaries can be used to communicate research findings to a wider audience, such as policymakers, practitioners, or the general public, in a concise and accessible manner.
- Facilitated decision-making: Research summaries can support decision-making processes by providing a summary of the research evidence on a particular topic. Policymakers or practitioners can use this information to make informed decisions about interventions, programs, or policies.
- Increased dissemination: Research summaries can be easily shared and disseminated, allowing research findings to reach a wider audience.
Limitations of Research Summary
Limitations of the Research Summary are as follows:
- Limited scope: Research summaries provide a brief overview of the research project’s main points, findings, and conclusions, which can be limiting. They may not include all the details, nuances, and complexities of the research that readers may need to fully understand the study’s implications.
- Risk of oversimplification: Research summaries can be oversimplified, reducing the complexity of the research and potentially distorting the findings or conclusions.
- Lack of context: Research summaries may not provide sufficient context to fully understand the research findings, such as the research background, methodology, or limitations. This may lead to misunderstandings or misinterpretations of the research.
- Possible bias: Research summaries may be biased if they selectively emphasize certain findings or conclusions over others, potentially distorting the overall picture of the research.
- Format limitations: Research summaries may be constrained by the format or length requirements, making it challenging to fully convey the research’s main points, findings, and conclusions.
- Accessibility: Research summaries may not be accessible to all readers, particularly those with limited literacy skills, visual impairments, or language barriers.
About the author

Muhammad Hassan
Researcher, Academic Writer, Web developer
You may also like

Data Collection – Methods Types and Examples

Delimitations in Research – Types, Examples and...

Research Process – Steps, Examples and Tips

Research Design – Types, Methods and Examples

Institutional Review Board – Application Sample...

Evaluating Research – Process, Examples and...
- SpringerLink shop
Discussion and Conclusions
Your Discussion and Conclusions sections should answer the question: What do your results mean?
In other words, the majority of the Discussion and Conclusions sections should be an interpretation of your results. You should:
- Discuss your conclusions in order of most to least important.
- Compare your results with those from other studies: Are they consistent? If not, discuss possible reasons for the difference.
- Mention any inconclusive results and explain them as best you can. You may suggest additional experiments needed to clarify your results.
- Briefly describe the limitations of your study to show reviewers and readers that you have considered your experiment’s weaknesses. Many researchers are hesitant to do this as they feel it highlights the weaknesses in their research to the editor and reviewer. However doing this actually makes a positive impression of your paper as it makes it clear that you have an in depth understanding of your topic and can think objectively of your research.
- Discuss what your results may mean for researchers in the same field as you, researchers in other fields, and the general public. How could your findings be applied?
- State how your results extend the findings of previous studies.
- If your findings are preliminary, suggest future studies that need to be carried out.
- At the end of your Discussion and Conclusions sections, state your main conclusions once again .
Back │ Next
- USC Libraries
- Research Guides
Organizing Your Social Sciences Research Paper
- 8. The Discussion
- Purpose of Guide
- Design Flaws to Avoid
- Independent and Dependent Variables
- Glossary of Research Terms
- Reading Research Effectively
- Narrowing a Topic Idea
- Broadening a Topic Idea
- Extending the Timeliness of a Topic Idea
- Academic Writing Style
- Applying Critical Thinking
- Choosing a Title
- Making an Outline
- Paragraph Development
- Research Process Video Series
- Executive Summary
- The C.A.R.S. Model
- Background Information
- The Research Problem/Question
- Theoretical Framework
- Citation Tracking
- Content Alert Services
- Evaluating Sources
- Primary Sources
- Secondary Sources
- Tiertiary Sources
- Scholarly vs. Popular Publications
- Qualitative Methods
- Quantitative Methods
- Insiderness
- Using Non-Textual Elements
- Limitations of the Study
- Common Grammar Mistakes
- Writing Concisely
- Avoiding Plagiarism
- Footnotes or Endnotes?
- Further Readings
- Generative AI and Writing
- USC Libraries Tutorials and Other Guides
- Bibliography
The purpose of the discussion section is to interpret and describe the significance of your findings in relation to what was already known about the research problem being investigated and to explain any new understanding or insights that emerged as a result of your research. The discussion will always connect to the introduction by way of the research questions or hypotheses you posed and the literature you reviewed, but the discussion does not simply repeat or rearrange the first parts of your paper; the discussion clearly explains how your study advanced the reader's understanding of the research problem from where you left them at the end of your review of prior research.
Annesley, Thomas M. “The Discussion Section: Your Closing Argument.” Clinical Chemistry 56 (November 2010): 1671-1674; Peacock, Matthew. “Communicative Moves in the Discussion Section of Research Articles.” System 30 (December 2002): 479-497.
Importance of a Good Discussion
The discussion section is often considered the most important part of your research paper because it:
- Most effectively demonstrates your ability as a researcher to think critically about an issue, to develop creative solutions to problems based upon a logical synthesis of the findings, and to formulate a deeper, more profound understanding of the research problem under investigation;
- Presents the underlying meaning of your research, notes possible implications in other areas of study, and explores possible improvements that can be made in order to further develop the concerns of your research;
- Highlights the importance of your study and how it can contribute to understanding the research problem within the field of study;
- Presents how the findings from your study revealed and helped fill gaps in the literature that had not been previously exposed or adequately described; and,
- Engages the reader in thinking critically about issues based on an evidence-based interpretation of findings; it is not governed strictly by objective reporting of information.
Annesley Thomas M. “The Discussion Section: Your Closing Argument.” Clinical Chemistry 56 (November 2010): 1671-1674; Bitchener, John and Helen Basturkmen. “Perceptions of the Difficulties of Postgraduate L2 Thesis Students Writing the Discussion Section.” Journal of English for Academic Purposes 5 (January 2006): 4-18; Kretchmer, Paul. Fourteen Steps to Writing an Effective Discussion Section. San Francisco Edit, 2003-2008.
Structure and Writing Style
I. General Rules
These are the general rules you should adopt when composing your discussion of the results :
- Do not be verbose or repetitive; be concise and make your points clearly
- Avoid the use of jargon or undefined technical language
- Follow a logical stream of thought; in general, interpret and discuss the significance of your findings in the same sequence you described them in your results section [a notable exception is to begin by highlighting an unexpected result or a finding that can grab the reader's attention]
- Use the present verb tense, especially for established facts; however, refer to specific works or prior studies in the past tense
- If needed, use subheadings to help organize your discussion or to categorize your interpretations into themes
II. The Content
The content of the discussion section of your paper most often includes :
- Explanation of results : Comment on whether or not the results were expected for each set of findings; go into greater depth to explain findings that were unexpected or especially profound. If appropriate, note any unusual or unanticipated patterns or trends that emerged from your results and explain their meaning in relation to the research problem.
- References to previous research : Either compare your results with the findings from other studies or use the studies to support a claim. This can include re-visiting key sources already cited in your literature review section, or, save them to cite later in the discussion section if they are more important to compare with your results instead of being a part of the general literature review of prior research used to provide context and background information. Note that you can make this decision to highlight specific studies after you have begun writing the discussion section.
- Deduction : A claim for how the results can be applied more generally. For example, describing lessons learned, proposing recommendations that can help improve a situation, or highlighting best practices.
- Hypothesis : A more general claim or possible conclusion arising from the results [which may be proved or disproved in subsequent research]. This can be framed as new research questions that emerged as a consequence of your analysis.
III. Organization and Structure
Keep the following sequential points in mind as you organize and write the discussion section of your paper:
- Think of your discussion as an inverted pyramid. Organize the discussion from the general to the specific, linking your findings to the literature, then to theory, then to practice [if appropriate].
- Use the same key terms, narrative style, and verb tense [present] that you used when describing the research problem in your introduction.
- Begin by briefly re-stating the research problem you were investigating and answer all of the research questions underpinning the problem that you posed in the introduction.
- Describe the patterns, principles, and relationships shown by each major findings and place them in proper perspective. The sequence of this information is important; first state the answer, then the relevant results, then cite the work of others. If appropriate, refer the reader to a figure or table to help enhance the interpretation of the data [either within the text or as an appendix].
- Regardless of where it's mentioned, a good discussion section includes analysis of any unexpected findings. This part of the discussion should begin with a description of the unanticipated finding, followed by a brief interpretation as to why you believe it appeared and, if necessary, its possible significance in relation to the overall study. If more than one unexpected finding emerged during the study, describe each of them in the order they appeared as you gathered or analyzed the data. As noted, the exception to discussing findings in the same order you described them in the results section would be to begin by highlighting the implications of a particularly unexpected or significant finding that emerged from the study, followed by a discussion of the remaining findings.
- Before concluding the discussion, identify potential limitations and weaknesses if you do not plan to do so in the conclusion of the paper. Comment on their relative importance in relation to your overall interpretation of the results and, if necessary, note how they may affect the validity of your findings. Avoid using an apologetic tone; however, be honest and self-critical [e.g., in retrospect, had you included a particular question in a survey instrument, additional data could have been revealed].
- The discussion section should end with a concise summary of the principal implications of the findings regardless of their significance. Give a brief explanation about why you believe the findings and conclusions of your study are important and how they support broader knowledge or understanding of the research problem. This can be followed by any recommendations for further research. However, do not offer recommendations which could have been easily addressed within the study. This would demonstrate to the reader that you have inadequately examined and interpreted the data.
IV. Overall Objectives
The objectives of your discussion section should include the following: I. Reiterate the Research Problem/State the Major Findings
Briefly reiterate the research problem or problems you are investigating and the methods you used to investigate them, then move quickly to describe the major findings of the study. You should write a direct, declarative, and succinct proclamation of the study results, usually in one paragraph.
II. Explain the Meaning of the Findings and Why They are Important
No one has thought as long and hard about your study as you have. Systematically explain the underlying meaning of your findings and state why you believe they are significant. After reading the discussion section, you want the reader to think critically about the results and why they are important. You don’t want to force the reader to go through the paper multiple times to figure out what it all means. If applicable, begin this part of the section by repeating what you consider to be your most significant or unanticipated finding first, then systematically review each finding. Otherwise, follow the general order you reported the findings presented in the results section.
III. Relate the Findings to Similar Studies
No study in the social sciences is so novel or possesses such a restricted focus that it has absolutely no relation to previously published research. The discussion section should relate your results to those found in other studies, particularly if questions raised from prior studies served as the motivation for your research. This is important because comparing and contrasting the findings of other studies helps to support the overall importance of your results and it highlights how and in what ways your study differs from other research about the topic. Note that any significant or unanticipated finding is often because there was no prior research to indicate the finding could occur. If there is prior research to indicate this, you need to explain why it was significant or unanticipated. IV. Consider Alternative Explanations of the Findings
It is important to remember that the purpose of research in the social sciences is to discover and not to prove . When writing the discussion section, you should carefully consider all possible explanations for the study results, rather than just those that fit your hypothesis or prior assumptions and biases. This is especially important when describing the discovery of significant or unanticipated findings.
V. Acknowledge the Study’s Limitations
It is far better for you to identify and acknowledge your study’s limitations than to have them pointed out by your professor! Note any unanswered questions or issues your study could not address and describe the generalizability of your results to other situations. If a limitation is applicable to the method chosen to gather information, then describe in detail the problems you encountered and why. VI. Make Suggestions for Further Research
You may choose to conclude the discussion section by making suggestions for further research [as opposed to offering suggestions in the conclusion of your paper]. Although your study can offer important insights about the research problem, this is where you can address other questions related to the problem that remain unanswered or highlight hidden issues that were revealed as a result of conducting your research. You should frame your suggestions by linking the need for further research to the limitations of your study [e.g., in future studies, the survey instrument should include more questions that ask..."] or linking to critical issues revealed from the data that were not considered initially in your research.
NOTE: Besides the literature review section, the preponderance of references to sources is usually found in the discussion section . A few historical references may be helpful for perspective, but most of the references should be relatively recent and included to aid in the interpretation of your results, to support the significance of a finding, and/or to place a finding within a particular context. If a study that you cited does not support your findings, don't ignore it--clearly explain why your research findings differ from theirs.
V. Problems to Avoid
- Do not waste time restating your results . Should you need to remind the reader of a finding to be discussed, use "bridge sentences" that relate the result to the interpretation. An example would be: “In the case of determining available housing to single women with children in rural areas of Texas, the findings suggest that access to good schools is important...," then move on to further explaining this finding and its implications.
- As noted, recommendations for further research can be included in either the discussion or conclusion of your paper, but do not repeat your recommendations in the both sections. Think about the overall narrative flow of your paper to determine where best to locate this information. However, if your findings raise a lot of new questions or issues, consider including suggestions for further research in the discussion section.
- Do not introduce new results in the discussion section. Be wary of mistaking the reiteration of a specific finding for an interpretation because it may confuse the reader. The description of findings [results section] and the interpretation of their significance [discussion section] should be distinct parts of your paper. If you choose to combine the results section and the discussion section into a single narrative, you must be clear in how you report the information discovered and your own interpretation of each finding. This approach is not recommended if you lack experience writing college-level research papers.
- Use of the first person pronoun is generally acceptable. Using first person singular pronouns can help emphasize a point or illustrate a contrasting finding. However, keep in mind that too much use of the first person can actually distract the reader from the main points [i.e., I know you're telling me this--just tell me!].
Analyzing vs. Summarizing. Department of English Writing Guide. George Mason University; Discussion. The Structure, Format, Content, and Style of a Journal-Style Scientific Paper. Department of Biology. Bates College; Hess, Dean R. "How to Write an Effective Discussion." Respiratory Care 49 (October 2004); Kretchmer, Paul. Fourteen Steps to Writing to Writing an Effective Discussion Section. San Francisco Edit, 2003-2008; The Lab Report. University College Writing Centre. University of Toronto; Sauaia, A. et al. "The Anatomy of an Article: The Discussion Section: "How Does the Article I Read Today Change What I Will Recommend to my Patients Tomorrow?” The Journal of Trauma and Acute Care Surgery 74 (June 2013): 1599-1602; Research Limitations & Future Research . Lund Research Ltd., 2012; Summary: Using it Wisely. The Writing Center. University of North Carolina; Schafer, Mickey S. Writing the Discussion. Writing in Psychology course syllabus. University of Florida; Yellin, Linda L. A Sociology Writer's Guide . Boston, MA: Allyn and Bacon, 2009.
Writing Tip
Don’t Over-Interpret the Results!
Interpretation is a subjective exercise. As such, you should always approach the selection and interpretation of your findings introspectively and to think critically about the possibility of judgmental biases unintentionally entering into discussions about the significance of your work. With this in mind, be careful that you do not read more into the findings than can be supported by the evidence you have gathered. Remember that the data are the data: nothing more, nothing less.
MacCoun, Robert J. "Biases in the Interpretation and Use of Research Results." Annual Review of Psychology 49 (February 1998): 259-287; Ward, Paulet al, editors. The Oxford Handbook of Expertise . Oxford, UK: Oxford University Press, 2018.
Another Writing Tip
Don't Write Two Results Sections!
One of the most common mistakes that you can make when discussing the results of your study is to present a superficial interpretation of the findings that more or less re-states the results section of your paper. Obviously, you must refer to your results when discussing them, but focus on the interpretation of those results and their significance in relation to the research problem, not the data itself.
Azar, Beth. "Discussing Your Findings." American Psychological Association gradPSYCH Magazine (January 2006).
Yet Another Writing Tip
Avoid Unwarranted Speculation!
The discussion section should remain focused on the findings of your study. For example, if the purpose of your research was to measure the impact of foreign aid on increasing access to education among disadvantaged children in Bangladesh, it would not be appropriate to speculate about how your findings might apply to populations in other countries without drawing from existing studies to support your claim or if analysis of other countries was not a part of your original research design. If you feel compelled to speculate, do so in the form of describing possible implications or explaining possible impacts. Be certain that you clearly identify your comments as speculation or as a suggestion for where further research is needed. Sometimes your professor will encourage you to expand your discussion of the results in this way, while others don’t care what your opinion is beyond your effort to interpret the data in relation to the research problem.
- << Previous: Using Non-Textual Elements
- Next: Limitations of the Study >>
- Last Updated: May 22, 2024 12:03 PM
- URL: https://libguides.usc.edu/writingguide
Organizing Academic Research Papers: 9. The Conclusion
- Purpose of Guide
- Design Flaws to Avoid
- Glossary of Research Terms
- Narrowing a Topic Idea
- Broadening a Topic Idea
- Extending the Timeliness of a Topic Idea
- Academic Writing Style
- Choosing a Title
- Making an Outline
- Paragraph Development
- Executive Summary
- Background Information
- The Research Problem/Question
- Theoretical Framework
- Citation Tracking
- Content Alert Services
- Evaluating Sources
- Primary Sources
- Secondary Sources
- Tertiary Sources
- What Is Scholarly vs. Popular?
- Qualitative Methods
- Quantitative Methods
- Using Non-Textual Elements
- Limitations of the Study
- Common Grammar Mistakes
- Avoiding Plagiarism
- Footnotes or Endnotes?
- Further Readings
- Annotated Bibliography
- Dealing with Nervousness
- Using Visual Aids
- Grading Someone Else's Paper
- How to Manage Group Projects
- Multiple Book Review Essay
- Reviewing Collected Essays
- About Informed Consent
- Writing Field Notes
- Writing a Policy Memo
- Writing a Research Proposal
- Acknowledgements
The conclusion is intended to help the reader understand why your research should matter to them after they have finished reading the paper. A conclusion is not merely a summary of your points or a re-statement of your research problem but a synthesis of key points. For most essays, one well-developed paragraph is sufficient for a conclusion, although in some cases, a two-or-three paragraph conclusion may be required.
Importance of a Good Conclusion
A well-written conclusion provides you with several important opportunities to demonstrate your overall understanding of the research problem to the reader. These include:
- Presenting the last word on the issues you raised in your paper . Just as the introduction gives a first impression to your reader, the conclusion offers a chance to leave a lasting impression. Do this, for example, by highlighting key points in your analysis or findings.
- Summarizing your thoughts and conveying the larger implications of your study . The conclusion is an opportunity to succinctly answer the "so what?" question by placing the study within the context of past research about the topic you've investigated.
- Demonstrating the importance of your ideas . Don't be shy. The conclusion offers you a chance to elaborate on the significance of your findings.
- Introducing possible new or expanded ways of thinking about the research problem . This does not refer to introducing new information [which should be avoided], but to offer new insight and creative approaches for framing/contextualizing the research problem based on the results of your study.
Conclusions . The Writing Center. University of North Carolina; Kretchmer, Paul. Twelve Steps to Writing an Effective Conclusion . San Francisco Edit, 2003-2008.
Structure and Writing Style
https://writing.wisc.edu/wp-content/uploads/sites/535/2018/07/conclusions_uwmadison_writingcenter_aug2012.pdf I. General Rules
When writing the conclusion to your paper, follow these general rules:
- State your conclusions in clear, simple language.
- Do not simply reiterate your results or the discussion.
- Indicate opportunities for future research, as long as you haven't already done so in the discussion section of your paper.
The function of your paper's conclusion is to restate the main argument . It reminds the reader of the strengths of your main argument(s) and reiterates the most important evidence supporting those argument(s). Make sure, however, that your conclusion is not simply a repetitive summary of the findings because this reduces the impact of the argument(s) you have developed in your essay.
Consider the following points to help ensure your conclusion is appropriate:
- If the argument or point of your paper is complex, you may need to summarize the argument for your reader.
- If, prior to your conclusion, you have not yet explained the significance of your findings or if you are proceeding inductively, use the end of your paper to describe your main points and explain their significance.
- Move from a detailed to a general level of consideration that returns the topic to the context provided by the introduction or within a new context that emerges from the data.
The conclusion also provides a place for you to persuasively and succinctly restate your research problem, given that the reader has now been presented with all the information about the topic . Depending on the discipline you are writing in, the concluding paragraph may contain your reflections on the evidence presented, or on the essay's central research problem. However, the nature of being introspective about the research you have done will depend on the topic and whether your professor wants you to express your observations in this way.
NOTE : Don't delve into idle speculation. Being introspective means looking within yourself as an author to try and understand an issue more deeply not to guess at possible outcomes.
II. Developing a Compelling Conclusion
Strategies to help you move beyond merely summarizing the key points of your research paper may include any of the following.
- If your essay deals with a contemporary problem, warn readers of the possible consequences of not attending to the problem.
- Recommend a specific course or courses of action.
- Cite a relevant quotation or expert opinion to lend authority to the conclusion you have reached [a good place to look is research from your literature review].
- Restate a key statistic, fact, or visual image to drive home the ultimate point of your paper.
- If your discipline encourages personal reflection, illustrate your concluding point with a relevant narrative drawn from your own life experiences.
- Return to an anecdote, an example, or a quotation that you introduced in your introduction, but add further insight that is derived from the findings of your study; use your interpretation of results to reframe it in new ways.
- Provide a "take-home" message in the form of a strong, succient statement that you want the reader to remember about your study.
III. Problems to Avoid Failure to be concise The conclusion section should be concise and to the point. Conclusions that are too long often have unnecessary detail. The conclusion section is not the place for details about your methodology or results. Although you should give a summary of what was learned from your research, this summary should be relatively brief, since the emphasis in the conclusion is on the implications, evaluations, insights, etc. that you make. Failure to comment on larger, more significant issues In the introduction, your task was to move from general [the field of study] to specific [your research problem]. However, in the conclusion, your task is to move from specific [your research problem] back to general [your field, i.e., how your research contributes new understanding or fills an important gap in the literature]. In other words, the conclusion is where you place your research within a larger context. Failure to reveal problems and negative results Negative aspects of the research process should never be ignored. Problems, drawbacks, and challenges encountered during your study should be included as a way of qualifying your overall conclusions. If you encountered negative results [findings that are validated outside the research context in which they were generated], you must report them in the results section of your paper. In the conclusion, use the negative results as an opportunity to explain how they provide information on which future research can be based. Failure to provide a clear summary of what was learned In order to be able to discuss how your research fits back into your field of study [and possibly the world at large], you need to summarize it briefly and directly. Often this element of your conclusion is only a few sentences long. Failure to match the objectives of your research Often research objectives change while the research is being carried out. This is not a problem unless you forget to go back and refine your original objectives in your introduction, as these changes emerge they must be documented so that they accurately reflect what you were trying to accomplish in your research [not what you thought you might accomplish when you began].
Resist the urge to apologize If you've immersed yourself in studying the research problem, you now know a good deal about it, perhaps even more than your professor! Nevertheless, by the time you have finished writing, you may be having some doubts about what you have produced. Repress those doubts! Don't undermine your authority by saying something like, "This is just one approach to examining this problem; there may be other, much better approaches...."
Concluding Paragraphs. College Writing Center at Meramec. St. Louis Community College; Conclusions . The Writing Center. University of North Carolina; Conclusions . The Writing Lab and The OWL. Purdue University; Freedman, Leora and Jerry Plotnick. Introductions and Conclusions . The Lab Report. University College Writing Centre. University of Toronto; Leibensperger, Summer. Draft Your Conclusion. Academic Center, the University of Houston-Victoria, 2003; Make Your Last Words Count . The Writer’s Handbook. Writing Center. University of Wisconsin, Madison; Tips for Writing a Good Conclusion . Writing@CSU. Colorado State University; Kretchmer, Paul. Twelve Steps to Writing an Effective Conclusion . San Francisco Edit, 2003-2008; Writing Conclusions . Writing Tutorial Services, Center for Innovative Teaching and Learning. Indiana University; Writing: Considering Structure and Organization . Institute for Writing Rhetoric. Dartmouth College.
Writing Tip
Don't Belabor the Obvious!
Avoid phrases like "in conclusion...," "in summary...," or "in closing...." These phrases can be useful, even welcome, in oral presentations. But readers can see by the tell-tale section heading and number of pages remaining to read, when an essay is about to end. You'll irritate your readers if you belabor the obvious.
Another Writing Tip
New Insight, Not New Information!
Don't surprise the reader with new information in your Conclusion that was never referenced anywhere else in the paper. If you have new information to present, add it to the Discussion or other appropriate section of the paper. Note that, although no actual new information is introduced, the conclusion is where you offer your most "original" contributions in the paper; it's where you describe the value of your research, demonstrate your understanding of the material that you’ve presented, and locate your findings within the larger context of scholarship on the topic.
- << Previous: Limitations of the Study
- Next: Appendices >>
- Last Updated: Jul 18, 2023 11:58 AM
- URL: https://library.sacredheart.edu/c.php?g=29803
- QuickSearch
- Library Catalog
- Databases A-Z
- Publication Finder
- Course Reserves
- Citation Linker
- Digital Commons
- Our Website
Research Support
- Ask a Librarian
- Appointments
- Interlibrary Loan (ILL)
- Research Guides
- Databases by Subject
- Citation Help
Using the Library
- Reserve a Group Study Room
- Renew Books
- Honors Study Rooms
- Off-Campus Access
- Library Policies
- Library Technology
User Information
- Grad Students
- Online Students
- COVID-19 Updates
- Staff Directory
- News & Announcements
- Library Newsletter
My Accounts
- Interlibrary Loan
- Staff Site Login
FIND US ON
- Differences between a finding, a conclusion, and a recommendation: examples
- Learning Center

Table of Contents
- Defining the Terms: What Is a Finding, a Conclusion, and a Recommendation in M&E?
- Why It Matters: Understanding the Importance of Differentiating between Findings, Conclusions, and Recommendations in M&E
- How to Identify and Distinguish between Findings, Conclusions, and Recommendations in M&E
- How to Communicate Findings, Conclusions, and Recommendations Effectively in M&E Reports
- The Benefits of Clear and Accurate Reporting of Findings, Conclusions, and Recommendations in M&E
1. Defining the Terms: What Is a Finding, a Conclusion, and a Recommendation in M&E?
Monitoring and Evaluation (M&E) is a critical process for assessing the effectiveness of development programs and policies. During the M&E process, evaluators collect and analyze data to draw conclusions and make recommendations for program improvement. In M&E, it is essential to differentiate between findings, conclusions, and recommendations to ensure that the evaluation report accurately reflects the program’s strengths, weaknesses, and potential areas for improvement.
In an evaluation report, a finding, a conclusion, and a recommendation serve different purposes and convey different information. Here are the differences between these three elements:
1.1 Finding
A finding is a factual statement that is based on evidence collected during the evaluation . It describes what was observed, heard, or experienced during the evaluation process. A finding should be objective, unbiased, and supported by data. Findings are typically presented in the form of a summary or a list of key points, and they provide the basis for the evaluation’s conclusions and recommendations.
Findings are an important part of the evaluation process, as they provide objective and unbiased information about what was observed, heard, or experienced during the evaluation. Findings are based on the evidence collected during the evaluation, and they should be supported by data and other relevant information. They are typically presented in a summary or list format, and they serve as the basis for the evaluation’s conclusions and recommendations. By presenting clear and accurate findings, evaluators can help stakeholders understand the strengths and weaknesses of the program or initiative being evaluated, and identify opportunities for improvement.
Catch HR’s eye instantly?
- Resume Review
- Resume Writing
- Resume Optimization
Premier global development resume service since 2012
Stand Out with a Pro Resume
1.2 Examples of Finding
Here are some examples of findings in M&E:
- “Program participants reported a high level of satisfaction with the quality of training provided, with 85% rating it as good or excellent.”
- “The program was successful in increasing the number of girls enrolled in secondary school, with a 25% increase observed in the target communities.”
- “Program beneficiaries reported improved access to healthcare services, with a 40% increase in the number of individuals accessing healthcare facilities in the program area.”
- “The program’s training curriculum was found to be outdated and ineffective, with only 30% of participants reporting that the training was useful.”
- “The program’s monitoring and evaluation system was found to be inadequate, with data quality issues and insufficient capacity among staff to carry out effective monitoring and evaluation activities.”
These findings represent objective, measurable results of the data collected during the M&E process, and can be used to inform program design and implementation, as well as to draw conclusions and make recommendations for improvement.
1.3 Conclusion
A conclusion is a judgment or interpretation of the findings based on the evidence collected during the evaluation. It is typically expressed in terms of what the findings mean or what can be inferred from them. Conclusions should be logical, evidence-based, and free from personal bias or opinion.
Conclusions often answer the evaluation questions or objectives, and they provide insights into the effectiveness or impact of the program, project, or intervention being evaluated. By synthesizing the findings into a cohesive narrative, evaluators can provide stakeholders with a clear and actionable understanding of the program or initiative being evaluated. Conclusions can also inform future planning and decision-making, by identifying areas for improvement and highlighting successful strategies or interventions. Overall, conclusions are a crucial component of the evaluation process, as they help stakeholders make informed decisions about the programs and initiatives they are involved in.
1.4 Examples of Conclusion
Here are some examples of conclusions in M&E:
- Based on the data collected, it can be concluded that the program was successful in achieving its objective of increasing access to clean water in the target communities.”
- “The data indicates that the program’s training curriculum is ineffective and in need of revision in order to better meet the needs of participants.”
- “It can be concluded that the program’s community mobilization efforts were successful in increasing community participation and ownership of the program.”
- “Based on the data collected, it is concluded that the program’s impact on improving maternal and child health outcomes is limited and further efforts are needed to address the underlying health system and infrastructure issues.”
- “The data collected indicates that the program’s impact on reducing poverty in the target area is modest, but still significant, and further investment in complementary programs may be needed to achieve more substantial reductions in poverty rates.”
- These conclusions are based on the evidence presented in the findings and represent the interpretation or explanation of the meaning of the findings. They help to provide insight into the impact and effectiveness of the program and can be used to make recommendations for improvement.
1.5 Recommendation
A recommendation is a specific action or set of actions proposed based on the findings and conclusions of the evaluation. Recommendations should be practical, feasible, and tailored to the needs of the stakeholders who will be implementing them. They should be supported by evidence and aligned with the goals of the program, project, or intervention being evaluated.
Recommendations often provide guidance on how to improve the effectiveness or efficiency of the program, project, or intervention, and they can help to inform decision-making and resource allocation. By presenting clear and actionable recommendations, evaluators can help stakeholders identify and prioritize areas for improvement, and develop strategies to address identified issues. Recommendations can also serve as a roadmap for future planning and implementation and can help to ensure that the program or initiative continues to achieve its intended outcomes over time.
Overall, recommendations are an essential component of the evaluation process, as they help to bridge the gap between evaluation findings and programmatic action. By proposing specific and evidence-based actions, evaluators can help to ensure that evaluation results are translated into meaningful improvements in program design, implementation, and outcomes.
1.6 Examples of Recommendation
Here are some examples of recommendations in M&E:
- “To improve the effectiveness of the program’s training, the curriculum should be revised to better meet the needs of participants, with a focus on practical, hands-on learning activities.”
- “To address the data quality issues identified in the monitoring and evaluation system, staff should receive additional training on data collection and management, and the system should be revised to incorporate additional quality control measures.”
- “To build on the success of the program’s community mobilization efforts, further investments should be made in strengthening community-based organizations and networks, and in promoting greater community participation in program planning and decision-making.”
- “To improve the program’s impact on maternal and child health outcomes, efforts should be made to address underlying health system and infrastructure issues, such as improving access to health facilities and training health workers.”
- “To achieve more substantial reductions in poverty rates in the target area, complementary programs should be implemented to address issues such as economic development, education, and social protection.”
These recommendations are specific actions that can be taken based on the findings and conclusions of the M&E process. They should be practical, feasible, and based on the evidence presented in the evaluation report. By implementing these recommendations, development practitioners can improve program effectiveness and impact, and better meet the needs of the target population.
2. Why It Matters: Understanding the Importance of Differentiating between Findings, Conclusions, and Recommendations in M&E
Differentiating between findings, conclusions, and recommendations is crucial in M&E for several reasons. First, it ensures accuracy and clarity in the evaluation report. Findings, conclusions, and recommendations are distinct components of an evaluation report, and they serve different purposes. By clearly defining and differentiating these components, evaluators can ensure that the report accurately reflects the program’s strengths and weaknesses, potential areas for improvement, and the evidence supporting the evaluation’s conclusions.
Second, differentiating between findings, conclusions, and recommendations helps to facilitate evidence-based decision-making. By clearly presenting the evidence supporting the evaluation’s findings and conclusions, and making recommendations based on that evidence, evaluators can help program managers and policymakers make informed decisions about program design, implementation, and resource allocation.
Finally, differentiating between findings, conclusions, and recommendations can help to increase the credibility and trustworthiness of the evaluation report. Clear and accurate reporting of findings, conclusions, and recommendations helps to ensure that stakeholders understand the evaluation’s results and recommendations, and can have confidence in the evaluation’s rigor and objectivity.
In summary, differentiating between findings, conclusions, and recommendations is essential in M&E to ensure accuracy and clarity in the evaluation report, facilitate evidence-based decision-making, and increase the credibility and trustworthiness of the evaluation.
3. How to Identify and Distinguish between Findings, Conclusions, and Recommendations in M&E
Identifying and distinguishing between findings, conclusions, and recommendations in M&E requires careful consideration of the evidence and the purpose of each component. Here are some tips for identifying and distinguishing between findings, conclusions, and recommendations in M&E:
- Findings: Findings are the results of the data analysis and should be objective and evidence-based. To identify findings, look for statements that summarize the data collected and analyzed during the evaluation. Findings should be specific, measurable, and clearly stated.
- Conclusions: Conclusions are interpretations of the findings and should be supported by the evidence. To distinguish conclusions from findings, look for statements that interpret or explain the meaning of the findings. Conclusions should be logical and clearly explained, and should take into account any limitations of the data or analysis.
- Recommendations: Recommendations are specific actions that can be taken based on the findings and conclusions. To distinguish recommendations from conclusions, look for statements that propose actions to address the issues identified in the evaluation. Recommendations should be practical, feasible, and clearly explained, and should be based on the evidence presented in the findings and conclusions.
It is also important to ensure that each component is clearly labeled and presented in a logical order in the evaluation report. Findings should be presented first, followed by conclusions and then recommendations.
In summary, identifying and distinguishing between findings, conclusions, and recommendations in M&E requires careful consideration of the evidence and the purpose of each component. By ensuring that each component is clearly labeled and presented in a logical order, evaluators can help to ensure that the evaluation report accurately reflects the program’s strengths, weaknesses, and potential areas for improvement, and facilitates evidence-based decision-making.
4. How to Communicate Findings, Conclusions, and Recommendations Effectively in M&E Reports
Communicating findings, conclusions, and recommendations effectively in M&E reports is critical to ensuring that stakeholders understand the evaluation’s results and recommendations and can use them to inform decision-making. Here are some tips for communicating findings, conclusions, and recommendations effectively in M&E reports:
- Use clear and concise language: Use clear, simple language to explain the findings, conclusions, and recommendations. Avoid technical jargon and use examples to illustrate key points.
- Present data visually: Use tables, graphs, and charts to present data visually, making it easier for stakeholders to understand and interpret the findings.
- Provide context: Provide context for the findings, conclusions, and recommendations by explaining the evaluation’s purpose, methodology, and limitations. This helps stakeholders understand the scope and significance of the evaluation’s results and recommendations.
- Highlight key points: Use headings, bullet points, and other formatting techniques to highlight key points, making it easier for stakeholders to identify and remember the most important findings, conclusions, and recommendations.
- Be objective: Present the findings, conclusions, and recommendations objectively and avoid bias. This helps to ensure that stakeholders have confidence in the evaluation’s rigor and objectivity.
- Tailor the report to the audience: Tailor the report to the audience by using language and examples that are relevant to their interests and needs. This helps to ensure that the report is accessible and useful to stakeholders.
In summary, communicating findings, conclusions, and recommendations effectively in M&E reports requires clear and concise language, visual presentation of data, contextualization, highlighting of key points, objectivity, and audience-tailoring. By following these tips, evaluators can help to ensure that stakeholders understand the evaluation’s results and recommendations and can use them to inform decision-making.
5. The Benefits of Clear and Accurate Reporting of Findings, Conclusions, and Recommendations in M&E
Clear and accurate reporting of M&E findings, conclusions, and recommendations has many benefits for development programs and policies. One of the most significant benefits is improved program design and implementation. By clearly identifying areas for improvement, program designers and implementers can make adjustments that lead to more effective and efficient programs that better meet the needs of the target population.
Another important benefit is evidence-based decision-making. When M&E findings, conclusions, and recommendations are reported accurately and clearly, decision-makers have access to reliable information on which to base their decisions. This can lead to more informed decisions about program design, implementation, and resource allocation.
Clear and accurate reporting of M&E findings, conclusions, and recommendations also supports accountability. By reporting transparently on program performance, development practitioners can build trust and support among stakeholders, including program beneficiaries, donors, and the general public.
M&E findings, conclusions, and recommendations also support continuous learning and improvement. By identifying best practices, lessons learned, and areas for improvement, development practitioners can use this information to improve future programming.
Finally, clear and accurate reporting of M&E findings, conclusions, and recommendations can increase program impact. By identifying areas for improvement and supporting evidence-based decision-making, development programs can have a greater positive impact on the communities they serve.
In summary, clear and accurate reporting of M&E findings, conclusions, and recommendations is critical for improving program design and implementation, supporting evidence-based decision-making, ensuring accountability, supporting continuous learning and improvement, and increasing program impact. By prioritizing clear and accurate reporting, development practitioners can ensure that their programs are effective, efficient, and have a positive impact on the communities they serve.

Very interesting reading which clearly explain the M&E finding, recommendation and conclusion, which sometimes the terms can be confusing
Leave a Comment Cancel Reply
Your email address will not be published.
How strong is my Resume?
Only 2% of resumes land interviews.
Land a better, higher-paying career

Jobs for You
Water, sanitation and hygiene advisor (wash) – usaid/drc.
- Democratic Republic of the Congo
Health Supply Chain Specialist – USAID/DRC
Chief of party – bosnia and herzegovina.
- Bosnia and Herzegovina
Project Manager I
- United States
Business Development Associate
Director of finance and administration, request for information – collecting information on potential partners for local works evaluation.
- Washington, USA
Principal Field Monitors
Technical expert (health, wash, nutrition, education, child protection, hiv/aids, supplies), survey expert, data analyst, team leader, usaid-bha performance evaluation consultant.
- International Rescue Committee
Manager II, Institutional Support Program Implementation
Senior human resources associate, services you might be interested in, useful guides ....
How to Create a Strong Resume
Monitoring And Evaluation Specialist Resume
Resume Length for the International Development Sector
Types of Evaluation
Monitoring, Evaluation, Accountability, and Learning (MEAL)
LAND A JOB REFERRAL IN 2 WEEKS (NO ONLINE APPS!)
Sign Up & To Get My Free Referral Toolkit Now:
Thank you for visiting nature.com. You are using a browser version with limited support for CSS. To obtain the best experience, we recommend you use a more up to date browser (or turn off compatibility mode in Internet Explorer). In the meantime, to ensure continued support, we are displaying the site without styles and JavaScript.
- View all journals
- My Account Login
- Explore content
- About the journal
- Publish with us
- Sign up for alerts
- Open access
- Published: 21 May 2024
Investigating nutrient biomarkers of healthy brain aging: a multimodal brain imaging study
- Christopher E. Zwilling ORCID: orcid.org/0000-0002-2873-0115 1 , 2 ,
- Jisheng Wu ORCID: orcid.org/0009-0003-6000-453X 3 , 4 , 5 &
- Aron K. Barbey ORCID: orcid.org/0000-0002-6092-0912 1 , 2 , 3 , 4 , 5 , 6
npj Aging volume 10 , Article number: 27 ( 2024 ) Cite this article
436 Accesses
237 Altmetric
Metrics details
- Cognitive ageing
The emerging field of Nutritional Cognitive Neuroscience aims to uncover specific foods and nutrients that promote healthy brain aging. Central to this effort is the discovery of nutrient profiles that can be targeted in nutritional interventions designed to promote brain health with respect to multimodal neuroimaging measures of brain structure, function, and metabolism. The present study therefore conducted one of the largest and most comprehensive nutrient biomarker studies examining multimodal neuroimaging measures of brain health within a sample of 100 older adults. To assess brain health, a comprehensive battery of well-established cognitive and brain imaging measures was administered, along with 13 blood-based biomarkers of diet and nutrition. The findings of this study revealed distinct patterns of aging, categorized into two phenotypes of brain health based on hierarchical clustering. One phenotype demonstrated an accelerated rate of aging, while the other exhibited slower-than-expected aging. A t-test analysis of dietary biomarkers that distinguished these phenotypes revealed a nutrient profile with higher concentrations of specific fatty acids, antioxidants, and vitamins. Study participants with this nutrient profile demonstrated better cognitive scores and delayed brain aging, as determined by a t-test of the means. Notably, participant characteristics such as demographics, fitness levels, and anthropometrics did not account for the observed differences in brain aging. Therefore, the nutrient pattern identified by the present study motivates the design of neuroscience-guided dietary interventions to promote healthy brain aging.
Similar content being viewed by others

Temporal dynamics of the multi-omic response to endurance exercise training

Associations of dietary patterns with brain health from behavioral, neuroimaging, biochemical and genetic analyses

Alzheimer’s disease risk reduction in clinical practice: a priority in the emerging field of preventive neurology
Introduction.
Accumulating evidence in Nutritional Cognitive Neuroscience indicates that diet and nutrition may benefit the aging brain (for a review, see ref. 1 ). A recent review of the literature surveyed 52 studies comprising more than 21,000 participants and found that dietary markers of the Mediterranean Diet were associated with healthy brain aging, as measured by MRI indices of structural and functional connectivity 2 . Despite the promise of these findings, questions remain about the causal effects of diet and nutrition on brain health and their role in age-related neurobiological decline; for example, whether elements of the Mediterranean Diet, such as polyunsaturated fatty acids (PUFAs), may limit the reduction in white matter volume with age. The potential benefits of the Mediterranean Diet may result from its focus on nutrient classes that have known functional relationships with the brain. For example, fatty acids, including monounsaturated, polyunsaturated, and saturated fatty acids, are necessary for structural brain integrity and development, cellular energy metabolism, and neurotransmission and neuromodulation 3 . Indeed, randomized controlled trials (RCTs) examining the effects of fatty acids on brain health typically observe improvements in brain function, white matter integrity, and gray matter volume 4 , 5 , 6 , 7 . Notably, however, RCTs that investigate the effects of fatty acids on cognitive performance (without additional measures of brain health) demonstrate mixed results, with positive 8 or null findings 9 . In addition to fatty acids, the Mediterranean Diet includes antioxidants (i.e., vitamins, flavonoids, and carotenoids), which are known to reduce oxidative stress and therefore to benefit brain health 10 , 11 . RCTs examining the effects of antioxidants on the aging brain demonstrate benefits in cerebral blood flow and for measures of functional brain connectivity (e.g., functional brain network integration 12 ). Evidence further suggests that antioxidants may have favorable effects on episodic memory, although these findings do not extend to all forms of memory affected by aging 7 , 13
More broadly, a large association study of ~75,000 participants revealed that greater consumption of antioxidants was associated with a lower chance of developing subjective cognitive impairment in late life 14 . Finally, research also suggests that choline, an essential nutrient that promotes structural brain integrity, cellular energy metabolism, and neurotransmission, may improve multiple facets of cognition in older adults 15 . Taken together, these findings suggest that nutrition may support and enhance cognitive function and brain health, especially in healthy older adults.
The potential for nutritional interventions to promote healthy brain function is particularly significant given the well-established effects of aging on cognitive performance and brain health 16 , 17 , 18 , 19 , 20 , 21 . Senescence is accompanied by age-related neurodegeneration in gray and white matter structures and an increase in ventricular space 22 . White matter fiber integrity declines with age, as indexed by decreased fractional anisotropy and increases in axial, radial, and mean diffusivity 23 . Concentrations of metabolic markers of neuronal integrity, measured by magnetic resonance spectroscopy (MRS), also decline with age 22 . Advancing age is associated with smaller cerebral volume, likely due to cortical neuronal degeneration and synaptic density reduction, in addition to reduced cortical thickness and surface area 24 , 25 . The observed changes in the aging brain are also known to affect cognitive function, producing declines in cognitive control, fluid intelligence, processing speed, and memory 21 , 26 , 27 , 28 , 29 .
Age-related changes in brain health are known to vary within the population, reflecting individual differences in the onset, duration, and severity of age-related neurological symptoms 19 , 30 , 31 . Thus, chronological age alone does not fully explain the complex trajectory of brain health in late life. Indeed, recent evidence demonstrates that although structural MRI measures can predict chronological age, there are often deviations in the predicted and observed aging trajectory, such that accelerated aging results in a brain that is older than expected, whereas delayed aging results in a brain that is younger than predicted 32 , 33 .
Although the literature on healthy aging has identified important risk factors that accelerate brain aging, much less is known about preventative factors that reduce the severity of neurobiological disease in late life 34 . Our research therefore sought to identify nutrient biomarker patterns that are associated with Accelerated versus Delayed Brain Aging, with an interest in guiding the development of nutritional interventions designed to promote healthy brain aging. Specifically, the present study was motivated by three primary aims. First, we sought to identify distinct phenotypes of Accelerated versus Delayed Brain Aging within a sample of 100 healthy older adults. Brain imaging measures were acquired from a comprehensive battery of over 100 neuroimaging markers of brain health, including measures of brain structure (i.e., volumetrics and white matter tracts), functional brain connectivity, and brain metabolites, as measured by MRS. Second, using a well-validated neuropsychological test battery, we compared performance on measures of intelligence, executive function, and memory in the Accelerated versus Delayed Brain Aging phenotypes. Finally, we investigated whether the observed phenotypes captured distinct nutrient biomarker profiles, with a focus on nutrients that are known to have favorable effects on cognitive function and brain health from the Mediterranean Diet (i.e., fatty acids, antioxidants, and vitamins).
We predicted that phenotypes of Accelerated versus Delayed Brain Aging would emerge, given well-established individual differences in brain aging trajectories. We also predicted that these distinct phenotypes would embody differences in cognitive function manifested by the observed differences in brain aging. Finally, our predictions about the role of nutrition in healthy brain aging were guided by findings to suggest that specific nutrients may benefit brain health, including poly- and mono-unsaturated fatty acids, vitamins, antioxidants, and carotenoids. Thus, by combining advances in Nutritional Cognitive Neuroscience—nutrient biomarkers of diet, multimodal brain imaging, and statistical modeling of brain aging—this interdisciplinary study aimed to identify nutrient profiles associated with Accelerated versus Delayed Brain Aging and to establish nutritional targets for future interventions designed to promote brain health.
Brain health phenotypes
A total of 139 variables of brain health were collected in the study, including measures of structure, function, and metabolism (Table 1 ). Brain volumes were measured separately for the left and right hemispheres for the Structural Regions listed in Table 1 , for a total of 68 regions. Total white matter integrity was measured for each of the Structural Regions in Table 1 , for a total of 34 tracts. Functional connectivity was assessed using four graph theory metrics on each of 8 brain networks, for a total of 32 measures. Finally, three metabolite concentrations were measured within each brain region.
Hierarchical clustering of all 139 brain measures collected in the study revealed two distinct phenotypes of brain health: Accelerated and Delayed Aging. Hierarchical clustering uses a similarity metric that identifies individuals who are most like one another across all brain measures. The two phenotypes identified by hierarchical clustering indicate that, across all study participants, one group is similar with less optimal brain health while the other group is similar with more optimal brain health. The dendrogram is presented in Supplementary Fig. 1 . The average value for the two phenotypes for each brain imaging domain from Table 1 —structure, metabolism, and functional connectivity—is listed in Table 2 . Relative to individuals with Accelerated Aging, those with Delayed Aging have larger brain volumes (0.48 vs 0.43), increased white matter integrity (0.61 vs 0.49), increased concentrations of brain metabolites (0.444 vs 0.441), increased functional connectivity for the whole brain (0.51 vs 0.45) and small world propensity (0.52 vs 0.43). Network functional connectivity was greater for individuals with Accelerated Aging relative to those with Delayed Aging for strength (0.57 vs 0.45), local efficiency (0.52 vs 0.47) and global efficiency (0.55 vs 0.43). Supplementary Figs. 2 , 3 and 4 present heatmaps of the values for each participant for each network or region of all brain measurements presented in Table 1 .
Brain age and brain health phenotypes
Brain Age (BA) was estimated for both brain health phenotypes. Individuals in the Accelerated Aging phenotype have an average BA of 65.1 whereas those in the Delayed Aging have an average BA of 59.7. This difference of 5.4 BA years is significant ( t statistic = 2.66, p value = 0.010). Chronological Age (CA) and BA are presented in Fig. 1 for both brain phenotypes. Many individuals in the Accelerated Aging phenotype have BAs closer to their CAs whereas many individuals in the Delayed Aging phenotype have BAs less than their CAs. Correlations between BA were computed with multiple brain modalities. BA was negatively associated with brain volumes ( r = −0.19, p value = 0.058), white matter tracts ( r = −0.37, p value = 0.00014), brain metabolites ( r = −0.25, p value = 0.017) and functional connectivity measures ( r = −0.19, p value = 0.063). These robust negative correlations suggest that a young BA is associated with the Delayed Brain Aging phenotype, indicating multiple brain modalities can predict BA specifically and brain health generally.

Chronological age (left side of each panel) versus brain age (right side of each panel) for the accelerated (left panel) and delayed (right panel) brain aging phenotypes.
Brain health and cognition
The study results established robust differences in brain structure, function, and metabolism between the two phenotypes of brain health. Furthermore, these phenotypes were inversely correlated with BA, where the individuals with Accelerated Aging have an Old BA and those with Delayed Aging have a Young BA. We next examined how differences in Delayed and Accelerated Brain Aging phenotypes map onto cognition. We assessed measures of intelligence (WASI), executive function (DKEFS), and memory (WMS). Individuals with Delayed Brain Aging outperformed those with Accelerated Brain Aging for all cognitive tests (see Fig. 2 ). Two scores for the Delayed Brain Aging Phenotype, reaction time (DKEFS Trails 5) and response errors (DKEFS Trails Errors), are negative and smaller than the Accelerated Brain Aging Phenotype, reflecting better cognitive performance for the Delayed Brain Aging Phenotype. A t test comparing the means between the Delayed and Accelerated Brain Aging groups is significant (p-value < 0.05) for tests of general and fluid intelligence (WASI_FSIQ4 and WASI_PRI), executive function (DKEFS_Trails.1) and memory (WMS_IMI). Supplementary Table 1 includes the scaled scores for all 15 cognitive tests.

The scores for Accelerated Brain Aging were set to a baseline of 0 for each cognitive measure and the Delayed Brain Aging group is expressed as a difference relative to that baseline, with values further from the baseline reflecting a larger difference. All cognitive scores were scaled between 0 and 1.
Nutrient profile of healthy brain aging
Having established two distinct phenotypes of brain aging derived from measures of brain structure, function, and metabolism, and based on a comprehensive cognitive battery, we lastly determined the nutritional profile of the Delayed Brain Aging phenotype (illustrated in Table 3 ). We examined the nutritional status of study participants using blood-based biomarkers. The nutrient biomarker profile of individuals in the Delayed Brain Aging phenotype was characterized by greater concentrations of 13 key nutrients compared to the Accelerated Aging phenotype, as determined by a t-test comparing the group means. Notably, the observed nutrient profile encompassed several nutrient categories important for brain health, including monounsaturated fatty acids (C18:1n-7 and C20:1n-9), ω-3 polyunsaturated fatty acids (C18:3n-3 and C20:5n-3, commonly known as ALA and EPA, respectively), ω-6 polyunsaturated fatty acids (C22:2n-6 and C20:2n-6), one long-chain saturated fatty acid (C24:0), the carotenoids lutein and zeaxanthin, and vitamin E and choline (see Supplementary Table 2 ). Nutrients that did not differ between the Accelerated versus Delayed Brain Aging phenotypes include Vitamins A, B2, B6, B12, D and E, carotenoids lycopene and carotene, short and medium chain saturated fatty acids (i.e., C10:0 to C22:0), and some PUFAs (e.g., C18:4n-3 and C22:4n-6). The coefficient of variability and intraclass correlation coefficient for the blood biomarkers in Table 3 are presented in Supplementary Table 3 .
Additionally, to rule out the possibility that other covariates contributed to brain aging differences between the phenotypes, we investigated multiple measures of demographics, anthropometrics, and physical fitness collected in the study. None of these variables differed between the two phenotypes using a t-test of the means, suggesting these factors do not explain the observed differences in brain aging (see Supplementary Table 4 ). Finally, following standard conventions, we controlled for BMI, sex, income, and education by including these factors as covariates in the analysis.
Nutritional Cognitive Neuroscience aims to identify specific foods and nutrients that promote healthy brain aging. Central to this effort is the discovery of nutrient profiles that can be targeted in nutritional interventions designed to promote brain health with respect to multimodal neuroimaging measures of brain structure, function, and metabolism. The present study advances four primary conclusions pursuant to this goal.
First, we provide evidence for a multimodal characterization of healthy brain aging, classified according to neuroimaging measures associated with Delayed or Accelerated Brain Aging. Specifically, relative to Accelerated Brain Aging, older adults with Delayed Brain Aging exhibited: (1) larger brain volumes, (2) better structural DTI integrity across 34 brain regions, (3) better functional connectivity for whole brain and network-level measures of local and global efficiency, and for small world propensity, and (4) greater concentrations of the brain metabolites choline, creatine, and NAA. These findings are notable given that prior research has focused primarily on a single brain imaging modality, limiting the nature and scope of conclusions drawn about the role of diet and nutrition in healthy brain aging.
Second, Delayed Brain Aging was inversely correlated with neuroimaging biomarkers of BA, demonstrating that a younger BA is associated with favorable brain health outcomes with respect to measures of brain structure, function, and metabolism 35 .
Third, scores on cognitive assessments of intelligence, executive function, and memory were higher for older adults with Delayed Brain Aging compared to those with Accelerated Brain Aging. These results are consistently supported by findings from the cognitive neuroscience of aging, namely that older adults with larger brain volumes, white matter tracts with greater integrity, and more efficient functional connectivity also demonstrate better cognitive performance 26 , 27 , 28 .
Fourth, the discovered nutrient profile for healthy brain aging was not derived from dietary questionnaires, as is typically employed in nutritional epidemiology, but from nutrient biomarkers which accurately reflect the concentrations of nutrients from the diet 36 , 37 . The observed nutrient profile is both broad, including fatty acids, carotenoids, and vitamins, and specific, identifying the amount and type of specific nutrients in each category.
Finally, the current study identified a nutrient profile related to healthy brain aging and a clinically relevant neuroimaging biomarker of BA. Although nutrition represents an established risk factor for age-related neurological disease 34 , the potential benefits of nutrition for promoting brain health are less well understood. Thus, the nutrient pattern identified by the present study motivates the design of neuroscience-guided dietary interventions to promote healthy brain aging. We now review the primary elements of the observed nutritional pattern and the mechanisms of action that have been proposed in the nutritional sciences to explain their benefits on cognitive and brain health.
Fatty acids
In our study, the fatty acid nutritional profile of individuals in the Delayed Brain Aging phenotype includes increased concentrations of EPA, ALA, docosadienoic acid, and eicosadienoic acid, all of which are known to reduce inflammation. Inflammation makes the vascular blood–brain barrier more permeable to cytokines, and chemokines, which interfere with neuronal and glial well-being and interrupt brain homeostasis 38 , 39 , 40 . Accumulating evidence has linked increased inflammation to decline in brain structure and function, cognitive decline, and increased risk of dementia 41 , 42 , 43 . We review the relationship between inflammation and each of these fatty acids in turn below.
Eicosanoids, signaling molecules responsible for cellular functions regulating inflammation and the central nervous system, derive from competing metabolic pathways that begin with three different 20-carbon fatty acids: arachidonic acid (20:4 ω-6, AA), eicosapentaenoic acid (20:5 ω-3, EPA), and di-homo γ linolenic acid (20:3 ω-6, DGLA) 44 . The ω-6 AA pathway promotes inflammation whereas the ω-3 DGLA and EPA pathways are less inflammatory, biologically inert, or even anti-inflammatory. Moreover, the three pathways compete for the same enzymes, rate-limiting molecules, transport, and acylation pathways. Hence, the greater the presence of anti-inflammatory generating ω-3 EPA in the diet, as is observed in our nutrient profile of Delayed Brain Aging, the fewer inflammatory eicosanoids will be generated by the AA pathway.
Another nutrient in the Delayed Brain Aging phenotype related to EPA and beneficial inflammation is α-linolenic acid or ALA. ALA is one of two essential fatty acids. EPA is obtained through diet or endogenously produced, via a metabolic pathway beginning with ALA. ALA converts to EPA with 10–20% efficiency 45 . Thus, greater concentrations of ALA in the diet, as is the case for individuals with healthy brain aging, can theoretically yield more of the beneficial EPA to compete with the inflammatory AA cascade. Excellent dietary sources of EPA and ALA include fish and shellfish, flaxseed, hemp seed, olive oil, soya oil, canola oil, chia seeds, pumpkin seeds, sunflower seeds, leafy vegetables, and walnuts.
The DGLA pathway is another beneficial competitor to the AA cascade, resulting in less severe inflammation or even anti-inflammatory metabolites. Two other nutrients in the profile of Delayed Brain Aging, eicosadienoic and docosadienoic acids, are closely related to the DGLA pathway. Eicosadienoic acid is the direct precursor of DGLA while docosadienoic acid is the immediate elongation product of DGLA. These two fatty acids have antioxidant abilities and anti-inflammatory properties meeting or exceeding those of DHA 46 . They also exhibit inhibitory activity against inflammation-causing enzymes by exerting similar physiological effects as over the counter non-steroidal anti-inflammatory drugs (e.g., ibuprofen) that block the COX-I and COX-II enzymes responsible for inflammation and pain 47 .
Saturated fatty acids are traditionally viewed as unhealthy 48 . However recent research suggests some long-chain fatty acids, with more than 20 carbon atoms, may confer health benefits, with evidence suggesting that they are associated with lower risk of coronary heart disease and type 2 diabetes, and may promote healthy aging 49 . Our nutrient profile of Delayed Brain Aging includes one very long chain saturated fatty acid, lignoceric acid (C24.0). Peanuts, macadamia nuts, and certain seed oils are excellent sources of lignoceric acid 49 . A recent study demonstrated that higher concentrations of long-chain fatty acids in plasma in mid-life resulted in reduced cognitive decline in a test of verbal fluency 20 years later 50 . Another study examined the concentration of lignoceric acid in brain tissue and discovered that females without cognitive impairment exhibited a larger concentration of C24.0 compared to females who developed Alzheimer’s disease. These findings provide a rationale for suggesting that long-chain saturated fatty acids, and lignoceric acid specifically, are important biomarkers of cognitive and brain health.
The final two fatty acids discovered in our nutrient profile of Delayed Brain Aging, vaccenic and gondoic acids, are both mono-unsaturated fatty acids, or MUFAs. MUFAs, which are common in olive oil and the Mediterranean Diet, are known to support brain and cognitive health 51 . Both vaccenic and gondoic acid have robust antioxidant activities 47 . Vaccenic acid is the primary type of fat from dairy products, such as milk, butter, and yogurt. Increasing consumption of dairy products increases the concentration of vaccenic acid in plasma 52 . The importance of vaccenic acid for brain health may lie in its metabolic conversion to conjugated linoleic acid, or CLA 53 . CLA is incorporated and metabolized into brain tissue, which further extends its anti-neuroinflammatory properties 54 . Nervonic acid is the predominant fatty acid in the white matter tissue of humans and one of its metabolic precursors is gondoic acid 55 . Based on these findings, it is possible that increased dietary concentrations of vaccenic and gondoic acids may enhance white matter brain integrity, although future research in Nutritional Cognitive Neuroscience is needed to clarify the precise role of these MUFAs in brain and cognitive health.
Carotenoids
Three different carotenoids, phytopigments that give many fruits and vegetables their characteristic color, figure prominently in the nutritional profile of Delayed Brain Aging. Carotenoid-rich foods include spinach, kale, corn, bell peppers (red, green, or yellow), tomatoes, watermelon, grapefruit, cantaloupe, broccoli, and carrots. Carotenoids have known benefits to cognitive and brain health, as demonstrated by studies that examine their effects on brain structure, brain network function, and memory 7 , 56 , 57 , 58 . Carotenoids accumulate in the retina of the eye and in the brain, and greater consumption of carotenoids increases their concentration in these tissues 59 . Carotenoids are known to benefit the brain because of their antioxidant properties. The brain is particularly vulnerable to oxidative stress due to its high lipid concentrations and high energy requirements 60 .
Vitamin E and choline were identified as important nutrients that promote cognitive and brain health in the Delayed Brain Aging phenotype. Multiple studies, including RCTs, have shown that high concentrations of Vitamin E in plasma are associated with better cognitive performance in healthy populations, aging populations, and Alzheimer disease patients 56 , 61 . Vitamin E’s efficacy in mitigating cognitive decline is likely through its antioxidant properties and its ability to aid in the transporting of fatty acids 62 . A recent RCT demonstrated that supplementation of Vitamin E, along with ω-3 fatty acids and carotenoids, improves performance on tests of working memory 57 . These findings are consistent with the results of the present study, which observed higher scores on tests of intelligence and memory within the Delayed Brain Aging phenotype. Notably, intelligence and memory are supported by multiple cortical regions (e.g., prefrontal, cingulate, and parietal cortices) and networks (e.g., frontoparietal network, the default mode network, and the salience network) 63 . Within the Delayed Brain Aging phenotype, we observed that these regions and networks demonstrated superior performance compared to the Accelerated Brain Aging phenotype based on measures of cortical volume and functional brain network efficiency, respectively. Excellent dietary sources of Vitamin E include nuts, seeds, and vegetable oils while significant amounts also come from green leafy vegetables and fortified cereals.
Choline, an essential B-vitamin-like nutrient, is also in the nutrient profile of Delayed Brain Aging. Choline plays at least two critical functions for cognitive and brain health: it is a necessary precursor for phosphatidylcholine, the predominant lipid in cell membranes and it is required for the synthesis and release of acetylcholine, a critical neurotransmitter 64 . Furthermore, brain white matter tracts and brain volume, which are enhanced in the Delayed Brain Aging phenotype, critically depend on choline for their cellular structure and integrity. Choline benefits both executive function and memory 15 , 64 . Excellent dietary sources of choline include animal-based proteins such as meat, poultry, fish, and eggs, while cruciferous vegetables and certain beans are also rich in choline.
Overall, there is strong evidence to support the nutrient profile underlying the Delayed Brain Aging phenotype in promoting cognitive and brain health. Many of the biochemical pathways underlying fatty acid synthesis and metabolism are well-known; but the implications of those competing pathways for cognitive and brain health, which importantly depend on the nutrients available from the diet, are only beginning to be understood. Moreover, future research should examine the differential impact of nutrition on different brain regions and networks, as certain nutrients may be important for different regions of the brain whereas other nutrients are required by the brain globally. Applying methods from Nutritional Cognitive Neuroscience, future RCTs should systematically investigate the effects of specific nutrient profiles on the structural integrity and functional efficiency of specific cortical regions and networks (e.g., combining nutrient biomarker analysis with MRI measures of local and global brain network operations). The current results provide evidence that some metabolic pathways (e.g., the DGLA pathway compared to the AA pathway) may yield more optimal brain and cognitive outcomes. Furthermore, the observed metabolic pathways that are less optimal for cognitive and brain health often result in higher levels of inflammation. Carotenoids and vitamins identified in the current study that benefit cognitive and brain health, such as lutein, choline, and Vitamin E, require regular consumption to have their beneficial effect. Importantly, these nutrients may accumulate preferentially in certain brain regions or networks, motivating an investigation of the selectivity of nutrition for promoting the health and function of specific brain regions and cortical networks.
Limitations
While some of the nutrients observed in the present study have solid molecular mechanisms to help explain their role in cognitive and brain health, other nutrients are less well understood. Research on long-chain saturated fatty acids and MUFAs (vaccenic acid and gondoic acid) have several preliminary studies suggesting their benefits on cognitive and brain health, but more research is needed to establish the precise mechanisms by which they exert an effect. Another limitation of the present study concerns the cross-sectional study design, sample size, and Caucasian participants. The Delayed Brain Aging phenotype identifies a set of nutrients that longitudinal and randomized controlled trials should target in future studies to determine their effects on cognitive and brain aging. Other statistical tools, such as canonical correlation analysis and structural equation modeling, may also be applied to draw new insights about the associations between brain aging and nutrition. The results of the present study need to be examined in non-Caucasian participants to assess the generality of findings. Moreover, while the current study examined brain health applying measures of brain structure, function, and metabolism, future research should also seek to understand how diet and nutrition effect the trajectory of brain aging within each of these measures. Additionally, the nutrient profile of Delayed Brain Aging identified in the current study does not imply they are the only nutrients that matter for brain health. Clearly, the brain needs many nutrients for healthy functioning, including amino acids, multiple B vitamins, ω-3 and ω-6 polyunsaturated fatty acids, monounsaturated fatty acids, choline, Vitamins C and D, and minerals like iron, zinc, and magnesium 65 . The nutrient profile identified in the current study differentiates Delayed Brain Aging from Accelerated Brain Aging. Finally, while the nutrient profiles discovered here suggest a basis for future testing of dietary interventions for optimal brain health, additional studies are needed to further establish and validate the present findings. It will also be important to build large-scale studies and research consortia to investigate the relationship between alternate measures of dietary intake and nutritional status, examining the reliability and validity of nutrient biomarkers, food frequency questionnaires, and their respective merits and limitations 66 , 67 .
The present study identified a specific profile of nutrients that may promote healthy brain aging, motivating further research to establish and validate these findings in the context of a randomized controlled trial. By building upon the observed findings, future research can inform the development of more effective, targeted dietary interventions that apply methods in Nutritional Cognitive Neuroscience. We believe this approach holds promise for the development of dietary strategies to support cognitive function and brain health in the aging population.
This cross-sectional study enrolled 100 healthy elderly adults from the Illinois Brain Aging Study cohort, a sample of community-dwelling Caucasian men and women aged 65–75 years. Participants were neurologically healthy and did not have evidence of cognitive impairment, as determined by a score of lower than 26 on the Mini-Mental State Examination 68 . Participants with mild cognitive impairment, dementia, a psychiatric illness within the last three years, a stroke within the past twelve months, cancer in the last three years, an inability to complete study activities, prior involvement in cognitive training or dietary intervention studies, or contraindications for magnetic resonance imaging (MRI) were excluded. All participants were right-handed with normal, or corrected to normal, vision.
Standard protocol approval and patient consent
In accordance with the University of Illinois and Carle Foundation Hospital Institutional Review Boards, informed consent was obtained from all participants in this study.
Nutrient biomarker acquisition and analysis
Fasting plasma was collected from each participant between 7:00 AM and 12:00 noon Central Time. Nutrient biomarkers were assayed, comprising three general classes of nutrients: fatty acids, carotenoids, and vitamins. Ethylenediaminetetraacetic acid (EDTA) plasma carotenoids and tocopherols were analyzed by high-performance liquid chromatography with a photodiode array detector (HPLC-PDA) using UV detection 69 . Plasma lipids were measured with gas chromatography using flame ionization and peaks of interest were identified by comparison to authentic fatty acid standards 70 . Vitamins were measured by a chemiluminescent immunometric assay or after extraction by radioimmunoassay 71 , 72 .
MRI data acquisition and processing
All data were collected on a Siemens Magnetom 3T Trio scanner using a 32-channel head coil in the MRI Laboratory of the Beckman Institute Biomedical Imaging Center at the University of Illinois.
MRI data acquisition
A high-resolution multi-echo T1-weighted magnetization prepared gradient-echo structural image was acquired for each participant (0.9 mm isotropic, TR: 1900 ms, TI: 900 ms, TE = 2.32 ms, with GRAPPA and an acceleration factor of 2). The functional neuroimaging data were acquired using an accelerated gradient-echo echoplanar imaging sequence sensitive to blood oxygenation level dependent (BOLD) contrast (2.5 × 2.5 × 3.0 mm voxel size, 38 slices with 10% slice gap, TR = 2000 ms, TE = 25 ms, FOV = 230 mm, 90° flip angle, 7 min acquisition time). During the resting-state fMRI scan, participants were shown a white crosshair on a black background viewed on an LCD monitor through a head coil-mounted mirror. Participants were instructed to lie still, focus on the visually presented crosshair, and to keep their eyes open 73 .
MRI data preprocessing
All MRI data processing was performed using FSL tools available in Functional Magnetic Resonance Imaging of the Brain (FMRIB) Software Library version 5.0. The high-resolution T1 Magnetization-Prepared Rapid Gradient-Echo (MPRAGE) was extracted using the Brain Extraction Tool 74 . FMRIB’s Automated Segmentation Tool 75 was applied to delineate gray matter, white matter, and cerebral spinal fluid (CSF) voxels. The resting-state fMRI data were pre-processed using the FSL FMRI Preprocessing and Model-Based Analysis (FEAT) analysis tool 76 , 77 . Pre-processing entailed: slice timing correction, motion correction, spatial smoothing (3 mm full width at half maximum kernel), nuisance signal regression (described below), standard fMRI temporal bandpass filtering (0.009–0.1 Hz, linear registration of functional images to structural images, and non-linear registration of structural images to the MNI152 brain template (2 mm isotropic voxel resolution).
Nuisance variables were modeled via General Linear Modeling (GLM) analyses to remove spurious correlations, noise introduced by head motion, and variables of no interest. These included head motion correction parameters (using the extended 12 motion parameters estimated in FEAT preprocessing), modeling of individual volume motion outliers estimated using DVARS (outliers flagged using the boxplot cutoff 1.5 × interquartile range 76 ), and averaging of mean white matter and cerebrospinal fluid signals across all voxels identified from the segmentation of the high resolution MPRAGE. The fully preprocessed resting-state fMRI data comprised the residual obtained from fitting these nuisance variables in the GLM framework. The residuals were transformed into normalized MNI152 space and re-sampled to 4 mm isotropic voxels to reduce computational complexity in post data processing for network analysis.
Brain volumetrics
Cortical reconstruction was performed with the Freesurfer image analysis software 78 . For this analysis, all the cortical gray matter volumes provided by the Freesurfer parcellation were examined. This included 68 regions throughout the frontal, parietal, temporal, and occipital lobes. Volumetric measures were adjusted for intracranial volume and sex using a regression model. The adjusted values were then used in further statistical analyses.
Volumetric analysis was performed on data from a 3D high-resolution (0.9 mm isotropic) T1-weighted scan using MPRAGE acquisition. Cortical reconstruction was performed with the Freesurfer image analysis suite, which is documented and freely available for download online ( http://surfer.nmr.mgh . harvard.edu/ ). All cortical reconstructions were manually checked for accuracy, as recommended by the software developers. The volumetric analyses focused on gray matter volume in the temporal cortex provided by Freesurfer parcellation. Regions of interest included the superior temporal cortex, middle temporal cortex, inferior temporal cortex, banks of the superior temporal sulcus, fusiform cortex, transverse temporal cortex, entorhinal cortex, temporal pole, and parahippocampal cortex.
Diffusion tractography imaging (DTI)
Whole brain diffusion tensor imaging was acquired with the following parameters: FOV = 240 × 240 mm; 72 slices, slice thickness = 2 mm; TE = 98 ms; TR = 10,000 ms; in-plane resolution = 1.875 × 1.875 mm; diffusion encoding directions = 30; b = 0 s/mm 2 and 1000 s/mm 2 . Data were processed using the University of Oxford’s Center for FMRIB Software Library (FSL) release 5.0 79 diffusion toolbox 80 , 81 . Eddy current correction was accomplished using the eddy correction tool and a diffusion tensor model was fit in each voxel using the DTIFIT tool, which generates fractional anisotropy (FA) values in every voxel. FA images were further processed using the FSL tract-based spatial statistics 82 toolbox, which projects each subjects’ FA data onto a mean white matter skeleton, representing the white-matter tracts common to all subjects. Mean FA within the white matter skeleton for specific regions of interest were calculated for each subject using the JHU ICBM DTI-81 atlas 83 .
Graph theory metrics of brain efficiency
The efficiency of brain network function was examined by investigating the small-world organization 84 of seven well-established intrinsic connectivity networks of the brain 85 . A small-word organization represents the optimal balance of local and global network efficiency, providing a parsimonious neural architecture that supports high local clustering (local efficiency) and short average path length (global efficiency). The procedure for computing small-world propensity is presented below.
First, the mean fMRI BOLD time series was extracted from subjects’ gray matter voxels using the Craddock parcellated brain atlas as a mask 86 . This parcellation of 200 regions provided whole-brain coverage and sufficiently high spatial resolution for conducting network analysis. A subject-wise functional connectivity matrix reflecting pairwise Pearson correlations between the mean BOLD time series signals obtained from nodes defined by the Craddock atlas was then computed and Fisher’s Z-transformed to achieve normality. These were standardized to Z-scores through multiplication with their standard deviation approximated as σ = 1/√( n − 3), where n is the number of time points corresponding to the BOLD signal 87 . A Bonferroni-corrected statistical Z-threshold was applied to identify significant positive correlations ( p < 0.05) within each subject’s whole-brain functional connectivity matrix derived from Craddock’s 800 parcellation atlas 88 , 89 . The thresholded Z-scores were rescaled to represent connection weights ranging from 0 to 1. Based on these positive connection weights, weighted connectivity matrices representing functional connectivity between nodes representative of seven intrinsic connectivity networks were obtained for each subject. The seven intrinsic connectivity network maps—visual, somatosensory, limbic, default mode, dorsal attention, ventral attention and frontoparietal—are at https://surfer.nmr.mgh.harvard.edu/fswiki/CorticalParcellation_Yeo2011 .
We then examined small-world propensity within the rescaled connectivity matrices derived for each of the seven intrinsic connectivity networks. Small world propensity Φ is calculated as the fractional deviation between a network’s clustering coefficient, C obs , and characteristic path length, L obs , from both lattice ( C latt , L latt ) and random ( C rand , L rand ) networks constructed with the same number of nodes and the same degree distribution:
The ratios Δ C and Δ L represent the fractional deviation of the metric ( C obs or L obs ) from its respective null model (a lattice or random network).
Magnetic resonance spectroscopy (MRS)
Metabolite concentration from MRS was determined using the procedure in ref. 90 . The anatomical scan was used to position a single voxel spectroscopy (SVS) scan in the parietal cortex extending into posterior cingulate cortex (voxel size: (20 mm), TR: 3000 ms, TE: 30 ms, 40 averages, BW: 2000 Hz, vector size: 1024). The voxel straddled the midline, including equal portions of the right and left hemispheres. Weak water suppression was employed, and six regional saturation bands were placed around the voxel to reduce contamination from subcutaneous fat. An additional scan was performed without water suppression to aid with quantification. Immediately following the spectroscopy acquisition, a T2-weighted overlay scan was performed with the same center location and orientation as the spectroscopy scan (TR = 5000 ms, TE = 84 ms, slice thickness 2 mm with 0.5 mm of spacing, FOV: 240 × 240 mm, 128 × 128 matrix size, GRAPPA acceleration factor: 2, 35 slices).
Metabolite quantitation was performed using tissue water as a reference. Water-scaled spectra were analyzed using LCModel software (Version 6.3-1H). No correction was performed to account for relaxation of metabolite signal. Because NAA and NAAG are difficult to differentiate, here we analyze the combined concentration of NAA + NAAG, labeled herein as NAAt with a peak appearing at 2.02 ppm.
Accurate water scaling requires corrections for the tissue composition of the voxel. Using the high-resolution structural scan, we calculated the volume fractions of gray matter (GM), white matter (WM), and CSF within each voxel using Matlab scripts (MathWorks, Natick, MA) that called functions from SPM8 (Wellcome Trust Centre for Neuroimaging). First, we segmented the MPRAGE using SPM8 to obtain tissue probability maps of GM, WM and CSF. We then created a mask in the space of the T2 overlay corresponding to the location of the spectroscopy scan. This mask has the same center and orientation as the T2 overlay but higher resolution (0.5 × 0.5 × 0.5 mm). We then registered the MPRAGE to the T2 overlay. The rotations and translations required for the registration were then applied to the tissue probability masks. We resliced the tissue probability maps into the space of the mask, and used the mask to calculate the volume fractions of GM, WM, and CSF within the volume of the spectroscopy voxel. These tissue fractions were later used to statistically correct NAAt for tissue volume-fraction dependencies.
Brain age (BA)
BA was derived using Brain-Age Regression Analysis and Computation Utility Software, or BARACUS, using T1-weighted structural images 33 , 91 .
Cognitive assessments
Neuropsychological tests investigating multiple facets of memory, executive function, and intelligence were administered. Our battery included the Wechsler Adult Intelligence Scale (WAIS 92 ), the trail-making test from the Delis-Kaplan Executive Function System (DKEFS 93 ), and the Wechsler Memory Systems (WMS 94 ).
Memory was measured by the Wechsler Memory Scale—Fourth Edition (WMS-IV) Older Adult Battery 94 . This assessment measured memory by way of four indices: Auditory Memory Index, Visual Memory Index, Immediate Memory Index, and Delayed Memory Index. The Auditory Memory Index indicates a participant’s ability to remember orally presented information. The Visual Memory Index indicates a participant’s ability to remember visually presented information. The Immediate Memory Index indicates a participant’s ability to recall visually and orally presented information immediately after it is presented. The Delayed Memory Index indicates a participant’s ability to recall and recognize visually- and orally-presented information after a 20 to 30-min delay. Participants’ raw scores on each subtest were converted to normalized scaled scores and subsequently combined into indices. Z-scores for each index were calculated and then averaged to create a composite memory score 95 .
Executive function
Executive functions were measured by the Delis–Kaplan Executive Function System (D–KEFS) Trail Making Test 93 . This assessment yields a measure of the executive functions that can be isolated from underlying skills, including visual scanning, number sequencing, letter sequencing, and motor speed. In this task, participants alternate between multiple task goals (either number or letter sequencing), which elicits a specific component of the executive functions known as cognitive flexibility. The reported results from the D-KEFS Trail Making Test assess cognitive flexibility while controlling for number and letter sequencing trials and therefore provide a measure of cognitive flexibility that is not confounded by underlying cognitive abilities (i.e., number and letter sequencing) required by the task.
Intelligence
General intelligence was measured by the Wechsler Abbreviated Scale of Intelligence– second edition (WASI-II 92 ). Per the scoring guidelines, this assessment measured general intelligence by way of an estimated intelligence quotient score, derived from fluid and crystallized test scores which, in turn, were derived from four subtests: a block design subtest, a matrix reasoning subtest, a vocabulary subtest, and a similarities subtest. In the block design subtest, participants were asked to reproduce pictured designs using specifically designed blocks as quickly and accurately as possible. In the matrix reasoning subtest, participants were asked to complete a matrix or serial reasoning problem by selecting the missing section from five response items. In the vocabulary subtest, participants were asked to verbally define vocabulary words (i.e., What does lamp mean?) that became progressively more challenging. In the similarities subtest, participants were asked to relate pairs of concepts (i.e., How are a cow and bear alike?) that became progressively more challenging. Per scoring guidelines, subjects’ raw scores were converted to standardized scores and combined into an estimated intelligence quotient score, which provided a measure of general intelligence.
Demographics, anthropometrics, and fitness
Demographics, including sex, education, and income, were collected via questionnaire responses provided by the participants. Anthropometric measures of weight, height, hip, and waist circumference were assessed by the study coordinator at the first study visit. Several measures of physical fitness were also collected or determined. Body Mass Index (BMI) was calculated from measured height and weight. Resting Heart Rate (RHR) was measured by the study coordinator during the participant’s first visit to the lab. Physical activity and the metabolic equivalent of VO 2 were assessed via a published questionnaire and required BMI and RHR as inputs 96 .
Analysis overview
First, individual differences in brain health were determined from the multimodal neuroimaging features using hierarchical clustering. Individuals with similar brain health were grouped together. Second, brain aging trajectories were computed for everyone and for each brain health group. Third, we examined cognitive aging differences within each brain health group. Fourth, a nutrient profile for the healthy brain and cognitive aging group was determined. Finally, lifestyle factors other than diet were examined to determine their role in brain and cognitive aging.
Statistical analyses
All statistical analyses were conducted in R Studio Version 2022.2.3.492 97 using the R statistical computing software environment Version 4.0.3 98 . Covariates with the weakest inter-correlations associated with age-related cognitive decline (age, gender, education, income, and Body Mass Index) were included as predictors in a separate regression model for each outcome measure of nutrition, brain, and cognition. Residualization was performed using the Frisch-Waugh-Lowell theorem. The net result of residualization is to remove the potential effects of covariates on the outcome. The residuals from each model were normally transformed using Tukey’s Ladder of Powers 99 and then [0,1] scaled. This process also had the effect of transforming outlier values to a normal range and resulting in a range of 0 to 1 for all variables. Hierarchical clustering, using the complete linkage method, was used to cluster individuals according to similarity of their brain features and it is not sensitive to multicollinearity. T tests of the mean were used to assess the magnitude and significance of differences between phenotypes.
Reporting summary
Further information on research design is available in the Nature Research Reporting Summary linked to this article.
Data availability
The individual de-identified participant data can be made available upon request.
Code availability
Codes used for this study are available upon reasonable request from the authors.
Zamroziewicz, M. & Barbey, A. Nutritional cognitive neuroscience: innovations for healthy brain aging. Front. Neurosci. 10 , 240 (2016).
Article PubMed PubMed Central Google Scholar
Jensen, D., Leoni, V., Klein-Flügge, M., Ebmeier, K. & Suri, S. Associations of dietary markers with brain volume and connectivity: a systematic review of MRI studies. Ageing Res. Rev. 70 , 101360 (2021).
Article CAS PubMed Google Scholar
Tracey, T., Steyn, F., Wolvetang, E. & Ngo, S. Neuronal lipid metabolism: multiple pathways driving functional outcomes in health and disease. Front. Mol. Neurosci. 11 , 10 (2018).
Köbe, T., Witte, A., Schnelle, A., Lesemann, A. & Fabian, S. Combined omega-3 fatty acids, aerobic exercise and cognitive stimulation prevents decline in gray matter volume of the frontal, parietal and cingulate cortex in patients with mild cognitive impairment. NeuroImage 131 , 226–238 (2016).
Article PubMed Google Scholar
Witte, A., Kerti, L., Hermannstädter, H., Fiebach, J. & Schreiber, S. Long-chain omega-3 fatty acids improve brain function and structure in older adults. Cereb. Cortex 24 , 3059–3068 (2014).
Jernerén, F., Elshorbagy, A., Oulhaj, A., Smith, S. & Refsum, H. Brain atrophy in cognitively impaired elderly: the importance of long-chain ω-3 fatty acids and B vitamin status in a randomized controlled trial. Am. J. Clin. Nutr. 102 , 215–221 (2015).
Sueyasu, T., Yasumoto, K., Tokuda, H., Kaneda, Y. & Obata, H. Effects of long-chain polyunsaturated fatty acids in combination with lutein and zeaxanthin on episodic memory in healthy older adults. Nutrients 15 , 2825 (2023).
Article CAS PubMed PubMed Central Google Scholar
Zwilling, C., Strang, A., Anderson, E., Jurcsisn, J. & Johnson, E. Enhanced physical and cognitive performance in active duty Airmen: evidence from a randomized multimodal physical fitness and nutritional intervention. Nat. Sci. Rep. 10 , 17826 (2020).
CAS Google Scholar
Mazereeuw, G., Lanctôt, K., Chau, S., Swardfager, W. & Herrmann, N. Effects of ω-3 fatty acids on cognitive performance: a meta-analysis. Neurobiol. Aging 33 , e17–e29 (2012).
Article Google Scholar
Franzoni, F. et al. Oxidative stress and cognitive decline: the neuroprotective role of natural antioxidants. Front. Neurosci. 15 , 729–757 (2021).
Terracina, S., Petrella, C., Francati, S., Lucarelli, M. & Barbato, C. Antioxidant intervention to improve cognition in the aging brain: the example of hydroxytyrosol and resveratrol. Int. J. Mol. Sci. 23 , 156–174 (2022).
Lindbergh, C., Lv, J., Zhao, Y., Mewborn, C. & Puente, A. The effects of lutein and zeaxanthin on resting state functional connectivity in older Caucasian adults: a randomized controlled trial. Brain Imaging Behav. 14 , 668–681 (2020).
Sloan, R., Wall, M. & Yeung, L. Insights into the role of diet and dietary flavanols in cognitive aging: results of a randomized controlled trial. Sci. Rep. 11 , 3837 (2021).
Yeh, T., Yuan, C., Ascherio, A., Rosner, B. & Willett, W. Long-term dietary flavonoid intake and subjective cognitive decline in US men and women. Neurology 97 , e1041–e1056 (2021).
CAS PubMed PubMed Central Google Scholar
Nakazaki, E., Mah, E., Sanoshy, K., Citrolo, D. & Watanabe, F. Citicoline and memory function in healthy older adults: a randomized, double-blind, placebo-controlled clinical trial. J. Nutr. 151 , 2153–2160 (2021).
López-Otín, C., Blasco, M., Partridge, L., Serrano, M. & Kroemer, G. The hallmarks of aging. Cell 153 , 1194–1217 (2013).
Kirkwood, T. Understanding the odd science of aging. Cell 120 , 437–447 (2005).
Kirkwood, T. B. A systematic look at an old problem. Nature 451 , 644–647 (2008).
Wrigglesworth, J., Ward, P., Harding, I., Nilaweera, D. & Wu, Z. Factors associated with brain ageing—a systematic review. BMC Neurolol. 21 , 312 (2021).
Bethlehem, R., Seidlitz, J., White, S. & Vogel, J. Brain charts for the human lifespan. Nature 604 , 525–533 (2022).
Harada, C., Natelson Love, M. & Triebel, K. Normal cognitive aging. Clin. Geriatr. Med. 29 , 737–752 (2013).
Raz, N. & Rodrigue, K. Differential aging of the brain: patterns, cognitive correlates and modifiers. Neurosci. Biobehav. Rev. 30 , 730–748 (2006).
Sexton, C., Walhovd, K., Storsve, A., Tamnes, C. & Westlye, L. Accelerated changes in white matter microstructure during aging: a longitudinal diffusion tensor imaging study. J. Neurosci. 34 , 15425–15436 (2014).
Lockhart, S. & DeCarli, C. Structural imaging measures of brain aging. Neuropsychol. Rev. 24 , 271–289 (2014).
Fjell, A., McEvoy, L., Holland, D., Dale, A. & Walhovd, K. Alzheimer’s Disease Neuroimaging Initiative Brain changes in older adults at very low risk for Alzheimer’s disease. J. Neurosci. 33 , 8237–8242 (2013).
Park, D. & Reuter-Lorenz, P. The adaptive brain: aging and neurocognitive scaffolding. Annu. Rev. Psychol. 60 , 173–196 (2009).
Salthouse, T. What and when of cognitive aging. Curr. Direc. Psychol. Sci. 13 , 140–144 (2004).
IJ, D., Corley, J., Gow, A., Harris, S. & Houlihan, L. Age-associated cognitive decline. Br. Med. Bull. 92 , 135–152 (2009).
Craik, F. I., Salthouse, T. A. The Handbook of Aging and Cogntion, 1st edn (Psychology Press, New York City, 2008).
Mattay, V., Goldberg, T., Sambataro, F. & Weinberger, D. Neurobiology of cognitive aging: insights from imaging genetics. Biol. Psychol. 79 , 9–22 (2008).
Nyberg, L. & Pudas, S. Successful memory aging. Annu. Rev. Psychol. 70 , 219–243 (2019).
Franke, K., Ziegler, G., Klöppel, S. & Gaser, C. Alzheimer’s Disease Neuroimaging Initiative Estimating the age of healthy subjects from T1-weighted MRI scans using kernel methods: exploring the influence of various parameters. Neuroimage 50 , 883–892 (2010).
Liem, F. Predicting brain-age from multimodal imaging data captures cognitive impairment. Neuroimage 148 , 179–188 (2017).
Franke, K. & Gaser, C. Ten years of brainAGE as a neuroimaging biomarker of brain aging: what insights have we gained? Front. Neurol 10 , 789 (2019).
Talukdar, T., Zwilling, C. & Barbey, A. Integrating nutrient biomarkers, cognitive function, and structural MRI data to build multivariate phenotypes of healthy aging. J. Nutr. 153 , 1338–1346 (2023).
Zamroziewicz, M., Paul, E. J., Zwilling, C. E. & Barbey, A. K. Determinants of fluid intelligence in healthy aging: omega-3 polyunsaturated fatty acid status and frontoparietal cortex structure. Nutr. Neurosci. 21 , 570–579 (2018).
Zamroziewicz, M., Paul, E., Zwilling, C. & Barbey, A. Predictors of memory in healthy aging: polyunsaturated fatty acid balance and fornix white matter integrity. Aging Dis. 8 , 372–383 (2017).
Galea, I. The blood-brain barrier in systemic infection and inflammation. Cell Mol. Immunol. 18 , 2489–2501 (2021).
Sankowski, R., Mader, S. & Valdés-Ferrer, S. Systemic inflammation and the brain: novel roles of genetic, molecular, and environmental cues as drivers of neurodegeneration. Front. Cell Neurosci. 9 , 29 (2015).
Sun, Y., Koyama, Y. & Shimada, S. Inflammation from peripheral organs to the brain: how does systemic inflammation cause neuroinflammation? Front. Aging Neurosci. 14 , 903455 (2022).
Sartori, A., Vance, D., Slater, L. & Crowe, M. The impact of inflammation on cognitive function in older adults: implications for healthcare practice and research. J. Neurosci. Nurs. 44 , 206–217 (2012).
Sæther, L., Ueland, T., Haatveit, B., Maglanoc, L. & Szabo, A. Inflammation and cognition in severe mental illness: patterns of covariation and subgroups. Mol. Psychiatry 28 , 1284–1292 (2023).
Kipinoinen, T., Toppala, S., Rinne, J., Viitanen, M. & Jula, A. Association of midlife inflammatory markers with cognitive performance at 10-year follow-up. Neurology 99 , e2294–e2302 (2022).
Soberman, R. & Christmas, P. The organization and consequences of eicosanoid signaling. J. Clin. Investig. 111 , 1107–1113 (2003).
Goyens, P., Spilker, M., Zock, P., Katan, M. & Mensink, R. Conversion of α-linolenic acid in humans is influenced by the absolute amounts of α-linolenic acid and linoleic acid in the diet and not by their ratio. Am. J. Clin. Nutr. 84 , 44–53 (2006).
Chen, Y., Qiu, X. & Yang, J. Comparing the in vitro antitumor, antioxidant and anti-inflammatory activities between two new very long-chain polyunsaturated fatty acids, docosadienoic acid (DDA) and docosatrienoic acid (DTA), and docosahexaenoic acid (DHA). Nutr. Cancer 73 , 1697–1707 (2021).
Henry, G., Momin, R., Nair, M. & Dewitt, D. Antioxidant and cyclooxygenase activities of fatty acids found in food. J. Agric. Food Chem. 50 , 2231–2234 (2002).
Caballero, B. Ed., Encyclopedia of Human Nutrition in Health Effects of Saturated Fatty Acids , 215–219 (Academic Press, 2013).
Lemaitre, R. & King, I. Very long-chain saturated fatty acids and diabetes and cardiovascular disease. Curr. Opin. Lipidol. 33 , 76–82 (2022).
Li, D., Misialek, J., Jing, M., Tsai, M. & Eckfeldt, J. Plasma phospholipid very-long-chain SFAs in midlife and 20-year cognitive change in the Atherosclerosis Risk in Communities (ARIC): a cohort study. Am. J. Clin. Nutr. 111 , 1252–1258 (2020).
Zamroziewicz, M., Talukdar, M., Zwilling, C. & Barbey, A. Nutritional status, brain network organization, and general intelligence. NeuroImage 161 , 241–250 (2017).
Burdge, G., Tricon, S., Morgan, R., Kliem, K. & Childs, C. Incorporation of cis-9, trans-11 conjugated linoleic acid and vaccenic acid (trans-11 18:1) into plasma and leucocyte lipids in healthy men consuming dairy products naturally enriched in these fatty acids. Br. J. Nutr. 94 , 237–243 (2005).
Field, C., Blewett, H., Proctor, S. & Vine, D. Human health benefits of vaccenic acid. Appl. Physiol. Nutr. Metab. 34 , 979–991 (2009).
Murru, E., Carta, G., Manca, C., Sogos, V. & Pistis, M. Conjugated linoleic acid and brain metabolism: a possible anti-neuroinflammatory role mediated by PPARα activation. Front. Pharmacol. 11 , 587140 (2021).
Fan, Y., Meng, H., Hu, G. & Li, F. Iosynthesis of nervonic acid and perspectives for its production by microalgae and other microorganisms. Appl. Microbiol. Biotechnol. 102 , 3027–3035 (2018).
Zwilling, C., Talukdar, T., Zamroziewicz, M. & Barbey, A. Nutrient biomarker patterns, cognitive function, and fMRI measures of network efficiency in the aging brain. NeuroImage 188 , 239–251 (2019).
Power, R., Nolan, J., Prado-Cabrero, A., Roche, W. & Coen, R. Omega-3 fatty acid, carotenoid and vitamin E supplementation improves working memory in older adults: A randomised clinical trial. Clin Nutr 41 , 405–414 (2022).
Ceravolo, S., Hammond, B., Oliver, W., Clementz, B. & Miller, L. Dietary carotenoids lutein and zeaxanthin change brain activation in older adult participants: a randomized, double-masked, placebo-controlled trial. Mol. Nutr. Food Res. 63 , 15 (2019).
Tanprasertsuk, J., Scott, T., Barbey, A., Barger, K. & Wang, X. Carotenoid-rich brain nutrient pattern is positively correlated with higher cognition and lower depression in the oldest old with no dementia. Front. Nutr. 8 , 704691 (2021).
Lee, K., Cha, M. & Lee, B. Neuroprotective effect of antioxidants in the brain. Int. J. Mol. Sci. 21 , 7152 (2020).
La Fata, G., Weber, P. & Mohajeri, M. Effects of vitamin E on cognitive performance during ageing and in Alzheimer’s disease. Nutrients 6 , 5453–5472 (2014).
Lee, P. & Ulatowski, L. Vitamin E: mechanism of transport and regulation in the CNS. IUBMB Life 71 , 424–429 (2019).
Colom, R., Karama, S., Jung, R. & Haier, R. Human intelligence and brain networks. Front. Psychol. 12 , 489–501 (2010).
Google Scholar
Zamroziewicz, M., Zwilling, C. & Barbey, A. Inferior prefrontal cortex mediates the relationship between phosphatidylcholine and executive functions in healthy, older adults. Front. Aging Neurosci. 8 , 226 (2016).
PubMed PubMed Central Google Scholar
Gómez-Pinilla, F. Brain foods: the effects of nutrients on brain function. Nat. Rev. Neurosci. 9 , 568–578 (2008).
Bowman, G., Shannon, J., Ho, E., Traber, M. & Frei, B. Reliability and validity of food frequency questionnaire and nutrient biomarkers in elders with and without mild cognitive impairment. Alzheimer Dis. Assoc. Disord. 25 , 49–57 (2011).
Fraser, G., Jaceldo-Siegl, K., Henning, S., Fan, J. & Knutsen, S. Biomarkers of dietary intake are correlated with corresponding measures from repeated dietary recalls and food-frequency questionnaires in the adventist health study-2. J. Nutr. 146 , 586–594 (2016).
Folstein, M., Folstein, S. & McHugh, P. Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 12 , 189–198 (1975).
Zhimin, X. & Howard, L. R. Analysis of Antioxidant‐Rich Phytochemicals (John Wiley & Sons Ltd, 2012).
Folch, J., Lees, M. & Stanley, G. A simple method for the isolation and purification of total lipids from animal tissues. J. Biol. Chem. 226 , 497–509 (1957).
Babson, A. The Cirrus Immulite automated immunoassay system. J. Clin. Immunoassay 14 , 83–88 (1991).
Hart, G., Furniss, J., Laurie, D. & Durham, S. Measurement of vitamin D status: Background, clinical use, and methodologies. Clin Lab 52 , 335–343 (2006).
CAS PubMed Google Scholar
Van Dijk, K., Hedden, T., Venkataraman, A., Evans, K. & Lazar, S. Intrinsic functional connectivity as a tool for human connectomics: theory, properties, and optimization. J. Neurophysiol. 103 , 297–321 (2010).
Smith, S. Fast robust automated brain extraction. Hum. Brain Mapp. 17 , 143–155 (2002).
Zhang, Y., Brady, M. & Smith, S. Segmentation of brain MR images through a hidden Markov random field model and the expectation-maximization algorithm. IEEE Trans. Med. Imaging 20 , 45–57 (2001).
Jenkinson, M., Beckmann, C., Behrens, T., Woolrich, M. & Smith, S. Fsl. Neuroimage 62 , 782–790 (2012).
Satterthwaite, T., Wolf, D. & Loughead, J. Impact of in-scanner head motion on multiple measures of functional connectivity: relevance for studies of neurodevelopment in youth. Neuroimage 60 , 623–632 (2012).
Reuter, M., Rosas, H. D. & Fischl, B. Highly accurate inverse consistent registration: a robust approach. Neuroimage 53 , 1181–1196 (2010).
Smith, S., Jenkinson, M., Woolrich, M., Beckmann, C. & Behrens, T. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 23 , S208–S219 (2004).
Behrens, T. E. et al. Characterization and propagation of uncertainty in diffusion-weighted MR imaging. Magn. Reson. Med. 50 , 1077–1088 (2003).
Behrens, T., Berg, H., Jbabdi, S., Rushworth, M. & Woolrich, M. Probabilistic diffusion tractography with multiple fibre orientations: what can we gain? Neuroimage 34 , 144–155 (2007).
Smith, S., Jenkinson, M., Johansen-Berg, H., Rueckert, D. & Nichols, T. Tract-based spatial statistics: Voxelwise analysis of multi-subject diffusion data. Neuroimage 31 , 1487–1505 (2006).
Oishi, K., Zilles, K., Amunts, K., Faria, A. & Jiang, H. Human brain white matter atlas: identification and assignment of common anatomical structures in superficial white matter. Neuroimage 43 , 447–457 (2008).
Muldoon, S., Bridgeford, E. & Bassett, D. Small-world propensity and weighted brain networks. Sci. Rep. 6 , 22057 (2016).
Yeo, B., Krienen, F. & Sepulcre, J. The organization of the human cerebral cortex is estimated by intrinsic functional connectivity. J. Neurophysiol. 106 , 1125–1165 (2011).
Craddock, R., James, G., Holtzheimer, P., Hu, X. & Mayberg, H. A whole brain fMRI atlas generated via spatially constrained spectral clustering. Hum. Brain Mapp. 33 , 1914–1928 (2012).
Ree, M. Correlation and regression: applications for industrial organizational psychology and management. Organ. Res. Methods 5 , 200–201 (2002).
Fox, M., Zhang, D., Snyder, A. & Raichle, M. The global signal and observed anticorrelated resting state brain networks. J. Neurophysiol. 101 , 3270–3283 (2009).
Murphy, K., Birn, R., Handwerker, D., Jones, T. & Bandettini, P. The impact of global signal regression on resting state correlations: are anti-correlated networks introduced?. Neuroimage 44 , 893–905 (2009).
Paul, E., Larsen, R. & Barbey, A. Dissociable brain biomarkers of fluid intelligence. NeuroImage 137 , 201–211 (2016).
Fischl, B. FreeSurfer. NeuroImage 62 , 774–781 (2012).
Wechsler, D. Wechsler Abbreviated Scale of Intelligence (Psychological Corporation, 1999).
Delis, D. C., Kaplan, E. & Kramer, J. H. Delis-Kaplan Executive Function System (D–KEFS) (The Psychological Corporation, San Antonio, 2001).
Wechsler, D. WMS-IV: Wechsler Memory Scale-fourth Edition (Pearson, San Antonio, 2009).
Siedlecki, K., Honig, L. & Stern, Y. Exploring the structure of a neuropsychological battery across healthy elders and those with questionable dementia and Alzheimer’s disease. Neuropsychology 22 , 400–411 (2009).
Jurca, R., Jackson, A., LaMonte, M., Morrow, J. J. & Blair, S. Assessing cardiorespiratory fitness without performing exercise testing. Am. J. Prev. Med. 29 , 185–193 (2005).
CoreTeam, R Studio: Integrated Development Environment for R (RStudio, PBC, Boston, 2022).
Team, R: A Language and Environment for Statistical Computing (R Foundation for Statistical Computing, Vienna, 2020).
Salvatore, M. rcompanion: Functions to Support Extension Education Program Evaluation , R package version 2.3.25, (2020).
Download references
Acknowledgements
This work was supported by a grant from Abbott Nutrition through the Center for Nutrition, Learning, and Memory at the University of Illinois (ANGC1205; PI: Barbey). The interdisciplinary community and supportive environment within the Decision Neuroscience Laboratory ( https://www.decisionneurosciencelab.org ) proved invaluable in completing this research.
Author information
Authors and affiliations.
Department of Psychology, University of Illinois, Urbana, IL, USA
Christopher E. Zwilling & Aron K. Barbey
Beckman Institute for Advanced Science and Technology, University of Illinois, Urbana, IL, USA
Decision Neuroscience Laboratory, University of Nebraska-Lincoln, Lincoln, NE, USA
Jisheng Wu & Aron K. Barbey
Center for Brain, Biology, and Behavior, University of Nebraska-Lincoln, Lincoln, NE, USA
Department of Psychology, University of Nebraska-Lincoln, Lincoln, NE, USA
Department of Bioengineering, University of Illinois, Urbana, IL, USA
Aron K. Barbey
You can also search for this author in PubMed Google Scholar
Contributions
Project Conception (C.E.Z., J.W., and A.K.B.), Study Design (C.E.Z., J.W., and A.K.B.), Data Analysis (C.E.Z. and J.W.), Manuscript drafting (C.E.Z., J.W., and A.K.B.), Manuscript editing and final review (C.E.Z. and A.K.B.).
Corresponding author
Correspondence to Aron K. Barbey .
Ethics declarations
Competing interests.
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplemental information, reporting summary, rights and permissions.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ .
Reprints and permissions
About this article
Cite this article.
Zwilling, C.E., Wu, J. & Barbey, A.K. Investigating nutrient biomarkers of healthy brain aging: a multimodal brain imaging study. npj Aging 10 , 27 (2024). https://doi.org/10.1038/s41514-024-00150-8
Download citation
Received : 18 October 2023
Accepted : 15 April 2024
Published : 21 May 2024
DOI : https://doi.org/10.1038/s41514-024-00150-8
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
Quick links
- Explore articles by subject
- Guide to authors
- Editorial policies
Sign up for the Nature Briefing: Translational Research newsletter — top stories in biotechnology, drug discovery and pharma.

- Open access
- Published: 16 May 2024
Experiences of UK clinical scientists (Physical Sciences modality) with their regulator, the Health and Care Professions Council: results of a 2022 survey
- Mark McJury 1
BMC Health Services Research volume 24 , Article number: 635 ( 2024 ) Cite this article
907 Accesses
Metrics details
In healthcare, regulation of professions is an important tool to protect the public. With increasing regulation however, professions find themselves under increasing scrutiny. Recently there has also been considerable concern with regulator performance, with high profile reports pointing to cases of inefficiency and bias. Whilst reports have often focused on large staff groups, such as doctors, in the literature there is a dearth of data on the experiences of smaller professional groups such Clinical Scientists with their regulator, the Health and Care Professions Council.
This article reports the findings of a survey from Clinical Scientists (Physical Sciences modality) about their experiences with their regulator, and their perception of the quality and safety of that regulation.
Between July–October 2022, a survey was conducted via the Medical Physics and Engineering mail-base, open to all medical physicists & engineers. Questions covered typical topics of registration, communication, audit and fitness to practice. The questionnaire consisted of open and closed questions. Likert scoring, and thematic analysis were used to assess the quantitative and qualitative data.
Of 146 responses recorded, analysis was based on 143 respondents. Overall survey sentiment was significantly more negative than positive, in terms of regulator performance (negative responses 159; positive 106; significant at p < 0.001). Continuous Professional Development audit was rated median 4; other topics were rated as neutral (fitness to practice, policies & procedures); and some as poor (value).
Conclusions
The Clinical Scientist (Physical Sciences) professional registrants rated the performance of their regulator more negatively than other reported assessments (by the Professional Standards Authority). Survey respondents suggested a variety of performance aspects, such as communication and fitness to practice, would benefit from improvement. Indications from this small dataset, suggest a larger survey of HCPC registrants would be useful.
Peer Review reports
In Healthcare, protection of patients and the public is a core principle. Part the framework of protections, includes regulation of professions [ 1 ]. This aims to mitigate risks such as the risk from bogus practitioners – insufficiently trained people acting as fully-trained professional practitioners, see Fig. 1 .

Recent UK media report on a bogus healthcare practitioner [ 2 ]
Regulation of professions ensures that titles (e.g. Doctor, Dentist, Clinical Scientist) are protected in law. The protected title means someone may only use that title, if they are on the national register, managed by the regulator – the Health and Care Professions Council (HCPC). It is a criminal offence to use a protected title if you are not entitled to do so [ 3 ]. There are a large number of regulators in healthcare – see Table 1 . Most of the regulators manage a register for one profession, except the HCPC which regulates 15 professions.
To be included on the register, a candidate must meet the regulators criteria for knowledge and training, and a key element to remain, is to show evidence of continuous professional development (CPD). Being on the register ensures that a practitioner has met the appropriate level of competence and professional practice.
For many healthcare workers, being on the HCPC register is a compulsory requirement to be appointable to a post. They must pay the necessary annual fees, and abide by the policies drawn-up by the regulator, and generally professions have no choice of regulator – these are statutory bodies, setup by government.
Recently, there has been considerable public dissatisfaction with the activity & performance of some regulators, notably Ofwat [ 4 ], and Ofgem [ 5 ]. Healthcare workers should expect a high level of professionalism, efficiency, and integrity from a regulator, as the regulator’s performance directly affects staff and public safety.
In terms of the regulation of UK Clinical Scientists, there is a dearth of data regarding experiences with the HCPC and views on the quality of regulation provided.
Findings are reported here from a 2022 survey of Medical Physicists and Engineers (one of the 16 job roles or ‘modalities’ under the umbrella of Clinical Scientist). The research aim was to assess experiences, and the level of ‘satisfaction’ with the regulator. For the remainder of this report, the term Clinical Scientist will be taken to mean Clinical Scientist (Medical Physicist/Engineer). The survey was designed to gather & explore data about opinions and experiences regarding several key aspects of how the HCPC performs its role, and perception of the quality & safety of regulation delivered.
A short survey questionnaire was developed, with questions aimed to cover the main regulatory processes, including registration & renewal, CPD audit, and fitness-to-practice. There were also questions relating more generally to HCPC’s performance as an organisation, e.g. handling of personal data. Finally, participants were asked to rate the HCPC’s overall performance and what they felt was the ‘value’ of regulation. The survey questions are listed in the Supplementary file along with this article.
Questions were carefully worded and there was a balance of open and closed questions. A five-point Likert score was used to rate closed questions. The survey was anonymous, and the questions were not compulsory, allowing the responders to skip irrelevant or difficult questions. The survey also aimed to be as short & concise as possible, to be a minimal burden to busy clinical staff & hopefully maximise response rate. There were a small number of questions at the start of the survey, to collect basic demographics on the respondents (role, grade, UK nation etc.).
The survey was advertised on the online JISC-hosted UK Medical Physics and Engineering (UKMPE) mail-base. This offered convenient access for the majority of Clinical Scientists. The survey was advertised twice, to allow for potential work absence, holiday/illness etc. It was active from the end of July 2002 until October 2022, when responses appeared to saturate.
The data is a combination of quantitative rating scores, and qualitative text responses. This allows a mixed-methods approach to data analysis, combining quantitative assessment of the Likert scoring, and (recursive) thematic analysis of the free-text answers [ 6 ]. Thematic analysis is a standard tool, and has been reported as a useful & appropriate for assessing experiences, thoughts, or behaviours in a dataset [ 7 ]. The survey questions addressed the main themes, but further themes were identified using an inductive, data-driven approach. Qualitative data analysis (QDA) was performed using NVivo (QSR International).
Two survey questions attempted to obtain an overall perception of HCPC’s performance: the direct one (Q12), and a further question’Would you recommend HCPC as a regulator…?’. This latter question doesn’t perhaps add anything more, and in fact a few respondents suggested it was a slightly awkward question, given professions do not have a choice of regulator – so that has been excluded from the analysis.
Study conduct was performed in accordance with relevant guidelines and regulations [ 8 , 9 ]. Before conducting the survey of Clinical Scientists, the survey was sent to their professional body, the Institute of Physics and Engineering in Medicine (IPEM). The IPEM Professional Standards Committee reviewed the survey questions [ 10 ]. Written informed consent was obtained from participants.
Data analysis
Data was collected via an MS form, in a single excel sheet and stored on a secure network drive. The respondents were anonymised, and the data checked for errors. The data was then imported into NVivo v12.
Qualitative data was manually coded for themes, and auto-coded for sentiment. An inductive approach was used to develop themes.
The sample size of responses allowed the use of simple parametric tests to establish the level of statistical significance.
Survey demographics
A total of 146 responses were collected. Two respondents noted that they worked as an HCPC Partner (a paid role). They were excluded from the analysis due to potential conflict of interest. One respondent’s responses were all blank aside from the demographic data, so they were also excluded from further analysis.
Analysis is based on 143 responses, which represents ~ 6% of the UK profession [ 11 ]. It is arguable whether it is representative of the profession at this proportion of response – but these responses do offer the only sizeable pool of data currently available. The survey was aimed at those who are on the statutory register as they are most likely to have relevant interactions & experiences of the HCPC, but a small number of responses were also received from Clinical Technologists (Medical Technical Officers-MTOs) and Engineers (CEs) and these have been included in the analysis. Figure 2 shows the breakdown in respondents, by nation.

Proportion of respondents, by nation
Of the respondents, 91% are registered Clinical Scientists, and would therefore have a broad range of experience with HCPC and its processes. Mean time on the register was 12 yrs. Respondents show a large range in seniority, and their roles are shown in Fig. 3 (CS-Clinical Scientist; CE-Clinical Engineer; MTO-Medical Technical Officer/Technician; CS-P are those working in private healthcare settings, so not on Agenda for Change (AfC) pay bands).

Breakdown in respondents, by role and pay banding
These data can be compared with the most recent HCPC ‘snapshot’ of the CS registrants (find here: Registrants by profession snapshot—1967 to 2019 | ( https://www.hcpc-uk.org/resources/data/2019/registrant-snapshot/ )).
The perception of overall regulator performance, can be assessed in two ways – one interview question directly asked for a rating score, and the overall survey sentiment also offers additional insight.
The score for overall performance was a median of 3 (mean 2.7; response rate 90%) which suggests neutral satisfaction.
Respondents were not asked directly to explain this overall performance rating – themes were extracted from the questionnaire as a whole.
The auto-coded sentiment scores generated in the NVivo software are shown in Table 2 . There is a significantly stronger negative sentiment than positive for HCPC performance – moderate, strong and total sentiment scores are all higher for negative sentiment. The normal test for a single proportion (109), shows the negative and positive sentiment differences have statistical significance with p < 0.001. Whilst the PSA assessment of HCPC performance in 2022–23 shows 100% performance for 4 out of 5 assessment areas, survey data here from regulated professionals suggests considerably less satisfaction with HCPC. This raises associated questions about the relevance and validity of PSA assessment.
A large number of respondents seem to question the value of regulation. Whilst many accepted the value for it in terms of protecting the safety of the public, many questioned its relevance & benefit to themselves. Many respondents also queried the payment model where although the main beneficiaries of regulation are the public & the employer, it is the registrants actually pay the fees for registration. There was very little mention in survey responses, of benefit in terms of protected-title. These issues were amalgamated into Theme 1— Value of regulation , with the two sub-themes Value in monetary terms (value-for-money) and Value in professional terms (benefit and relevance to the individual professional) (see Table 3 ).
In the survey, several aspects of HCPC organisational performance were scored – handling of personal data, registration and renewal, engagement with the profession, audit, and the quality and usefulness of HCPC policies. These formed Theme 2 and its sub-themes.
A third theme Registrant competence and vulnerability , was developed to focus on responses to questions related to the assessment of registrant competence and Fitness To Practice (FTP) processes.
Finally, the survey also directly asked respondents if they could suggest improvements which would have resulted in higher scoring for regulation quality and performance. These were grouped into Theme 4.
Theme 1 – Value of regulation
Value in monetary terms.
The Likert score for value-for-money was a median of 2 (mean 2.3; response rate 100%) which suggests dissatisfaction. This is one of the few survey questions to elicit a 100% response rate – a clear signal of its importance for registrants.
There was a high number of responses suggesting fees are too expensive (and a significantly smaller number suggesting good value). This ties in with some respondents explaining that the ‘benefit’ from registration is mainly for the employer (an assurance of high quality, well-trained staff). Several respondents point to little ‘tangible’ benefit for registrants and query whether the payment model is fair and if the employer should pay registrant fees.
“Expensive fees for what appears to be very little support.” Resp094
“It seems that I pay about £100 per year to have my name written on a list. It is unclear to me what the HCPC actually does in order to justify such a high fee.” Resp014
“I get, quite literally, nothing from it. It’s essentially a tax on work.” Resp008
Several respondents suggested that as registration was mandated by the employer, it was in essence an additional ‘tax’ on their employment, which was highlighted previously by Unison [ 12 ]. A comparator for payment model, are the checks preformed on potential staff who will be working with children and vulnerable adults. In general, these ‘disclosure’ checks are paid for by the employer, however the checks are not recurrent cost for each individual, but done once at recruitment.
Value in professional terms & relevance
This was not a direct question on the questionnaire, but emerged consistently in survey responses. Aside from value-for-money, the value of regulation can also refer to more general benefit and relevance for a professional, for example in protecting a professional title or emphasising the importance of a role. Many respondents commented, in relation to the ‘value’ of regulation, about the relevance of the HCPC to them and their job/role.
The largest number of responses highlighted the lack of clarity about HCPC’s role, and also to note its lack of relevance felt by a significant proportion of respondents.
“Not sure I have seen any value in my registration except that it is a requirement for my role” Resp017
“I really fail to understand what (sic) the benefits of registration.” Resp018
“They do not promote the profession. I see no evidence of supporting the profession. I pay to have the title and I am not aware of any other benefits.” Resp038
Theme 2 – HCPC performance
Communication & handling data.
The survey questionnaire did not have a specific question relating to communication, therefore no specific Likert scores are available. Rather, communication was a sub-theme which emerged in survey responses. The response numbers related to positive (1) and negative experiences (50) clearly suggest an overall experience of poor communication processes (and statistically significant at p < 0.001 for a normal proportion test).
One respondent noted they had ‘given up’ trying to communicate with HCPC electronically. Several respondents also noted issues with conventional communication—letters from HCPC going to old addresses, or being very slow to arrive.
“…I have given up on contacting by electronic means.” Resp134
When trying to renew their registration, communication with HCPC was so difficult that two respondents noted they raised a formal complaint.
A number of respondents noted that when they eventually got through to the HCPC, staff were helpful, so the main communication issue may relate to insufficiently resourced lines of communication (phones & email) or the need for a more focussed first point of contact e.g. some form of helpdesk or triaging system.
“Recently long wait to get through to speak to someone… Once through staff very helpful.” Resp126
This topic overlaps with the next (Processing Registration & renewals) in that both involve online logins, website use etc.
Security & data handling was rated as neutral (median 3, mean 3.4; response rate 91%). Although responses were balanced in terms of satisfaction, a significant number noted a lack of knowledge about HCPC processes. There are almost equal proportions of respondents reporting no issues, some problems with handling of personal data, or insufficient knowledge to express an opinion.
Registration and renewal
The score for processing registrations & renewals, was a median of 4 (mean 3.5; response rate 92%) which suggests modest satisfaction.
The overall rating also suggests that the issues may have been experienced by a comparative minority of registrants and that for most, renewal was straightforward.
“They expected people to call their phone number, which then wasn’t picked up. They didn’t reply to emails except after repeated attempts and finally having to resort to raising a complaint.” Resp023
“Difficult to get a timely response. Difficult to discuss my situation with a human being…” Resp044
Although the Likert score is positive, the themes in responses explaining the rating, are more mixed. Many respondents mentioned either having or knowing others who had issues with registration renewal, and its online processes including payments. A few respondents mentioned that the process was unforgiving of small errors. One respondent, for example, missed ticking a box on the renewal form, was removed from the register and experienced significant difficulties (poor communication with HCPC) getting the issue resolved.
Some respondents noted issues related to a long absence from work (e.g. maternity/illness etc.) causing them to miss registration deadlines – for some, this seems to have resulted in additional fees to renew registration. It seems rather easy for small errors (on either side) to result in registrants being removed from the register. For registrants, this can have very serious consequences and it can then be difficult and slow to resolve this, sometimes whilst on no pay. There have also been other reported instances of renewal payment collection errors [ 13 ].
“I had been off work… and had missed their renewal emails…I was told that there would be no allowances for this situation, and I would have to pay an additional fee to re-register…” Resp139.
Some respondents raised the issue of exclusion – certain staff groups not being included on the register—such as Clinical Technologists and Clinical Engineers. This desire for inclusion, also points to a perception of value in being on the register. One respondent raised an issue of very difficult and slow processing of registration for a candidate from outside the UK.
“Staff member who qualified as medical physicist abroad…has had a dreadful, drawn out and fruitless experience.” Resp135
Overall, many respondents noted difficulties in renewing registration and issues with HCPC’s online processes. Some of these issues (e.g. website renewal problems) may have been temporary and are now resolved, but others (e.g. available routes for registration) remain to be resolved.
Audit process & policies
In the survey, 12% respondents reported having been audited by HCPC regarding their CPD (response rate 97%). This is well above the level of 2.5% of each profession, which HCPC aims to review at each renewal [ 14 ], and similar values reported by some professional bodies [ 15 ]. The participants seem representative, although two respondents mentioned their perception of low audit rates. Data on CPD audit is available here: https://www.hcpc-uk.org/about-us/insights-and-data/cpd/cpd-audit-reports/
Respondents rated the process of being audited as a median of 4 (mean 3.7), which is the joint highest score on the survey, pointing to satisfaction with the process. From the responses, the overall perception could be summed up as straight-forward, but time-consuming. Without regular record-keeping, unfortunately most audits will be time-consuming – the HCPC more so, as it is not an annual audit, but covers the two preceding years.
Some respondents did find the process not only straight-forward, but also useful (related to feedback received). However, responses regarding feedback were mixed, with comments on both good, and poor feedback from HCPC.
“Not difficult but quite long-winded” Resp008
“Very stressful and time consuming” Resp081
“While it was a lot of work the process seemed very thorough and well explained.” Resp114
The HCPC’s policies & procedures were rated as a median of 3 (mean 3.2; response rate 98%). This neutral score could suggest a mixture of confidence in HCPC practise. This score may also reflect the fact that the majority of respondents had either not read, or felt they had no need to read the policies, and so are largely unfamiliar with them.
The reasons for this lack of familiarity are also explained by some respondents – four commented that the policies & procedures are rather too generic/vague. Three respondents noted that they felt the policies were not sufficiently relevant to their clinical roles to be useful. This may be due to the policies being written at a level to be applicable to registrants from all 16 modalities – and perhaps a limitation of the nature of HCPC as a very large regulator. Familiarity seemed mainly to be restricted to policies around registration, and CPD. There were slightly lower response levels for positive sentiment (6), than negative sentiment (9).
“I’ve never had cause to read them.” Resp115
“Detached from the real clinical interface for our professions…” Resp083
HCPC split their policies into ‘corporate’- which relate to organisational issues (e.g. equality & diversity; find them here: Our policies and procedures | ( https://www.hcpc-uk.org/about-us/corporate-governance/freedom-of-information/policies/#:~:text=Our%20main%20policies%20and%20procedures%201%20Customer%20feedback,scheme%20...%207%20Freedom%20of%20Information%20Policy%20 )) and those more relevant to professions (e.g. relating to the register; find them here: Resources | ( https://www.hcpc-uk.org/resources/?Query=&Categories=76 )).
One respondent noted not only that the policies were ‘as you might expect’, but felt the policies were less demanding than those from other similar bodies such as the CQC ( https://www.cqc.org.uk/publications ).
“…Other regulatory bodies (such as the CQC for example) have policies and procedures that are a lot more challenging to comply with.” Resp022
Theme 3 – Registrant competence and vulnerability
In this survey, 3.5% (5/143) of respondents noted some involvement with the HCPC’s Fitness to Practice service. These interactions were rated at a median of 3 (mean 2.8) suggesting neutral sentiment.
Firstly, we can immediately see the level of interaction with the FTP team is very small. CS registrants represent approx. 2% of HCPC registrants, and the level of CS referrals to FTP in 2020–21 was 0.2% [ 16 ].
The data is a very small sample, but responses vary strongly, so it is worth digging a little further into the granularity of individual responses. Response scores were 1, 1, 2, 5, 5 – which are mainly at the extremes of the rating spectrum. The majority of respondents described poor experiences with the FTP team: errors, a process which was ‘extremely prolonged’, involved slow/poor communication, and processes which were ‘entirely opaque’.
“It is slow, the process was badly managed… and the system was entirely opaque,” Resp37
“They were hard to contact and I didn't feel they listened…no explanation, apology or assurance it would not happen again. It left my colleague disillusioned and me very angry on their behalf…” Resp044
Some respondents commented that the team were not only difficult to contact, but also didn’t seem to listen. At the end of a process which involved errors from HCPC, one respondent noted were ‘no explanation, apologies or assurance that it would not happen again’, leaving the registrant ‘disillusioned’. These experiences do not fit with the HCPC’s stated goal to be a compassionate regulator, see Fig. 4 . Arguably it is more difficult to change a culture of behaviour and beliefs, than to publish a corporate goal or statement of vision.

HCPC’s vision statement & purpose [ 17 ]
Some survey respondents have noted the necessity of regulation for our profession.
“Ultimately I am very grateful that I can register as a professional.” Resp024
Theme 4 – Suggestions for improved regulation
Following the question relating to overall performance, respondents were invited to suggest things which might improve their rating for HCPC’s performance and value. These suggestions were also combined with those which appeared in earlier survey responses.
Although we are in a current cost-of-living crisis, responses did not query simply high absolute cost of fees, but also queried the value/benefit of HCPC regulation for registrants. Many responses expressed doubt as to the added value & relevance of HCPC registration for them. They seem to point to a desire for more tangible benefit from their fees. Perhaps, given the costs and levels of scrutiny, registrants want some definite benefit to balance the scales .
“Cost less and do more for the people who are on the register.” Resp089
“Vastly reduced cost. Employer paying registrant fees.” Resp074
A significant number of responses pointed out that the main benefits of registration are for the public, and for employers – but that it is the registrants who pay for registration. Many queries why this should be, and whether there should be a different payment model, where for example employers pay.
Similarly, some respondents felt that the HCPC’s unusual position of regulating a large swathe of healthcare professions was not necessarily helpful for their profession or others.
Communication and response times are obviously an issue of concern for registrants, and improvements are needed based on the low satisfaction levels reported here. This is also linked to a wish for increased engagement with the CS profession.
“Engagement with the workforce, specialism specific development, reduced fees” Resp025
Some responses suggested they would be comforted by increased accountability / governance of HCPC including improved FTP efficiency.
“More accountability to registrants” Resp130
Finally, improvement in terms of additional registration routes for Engineers & Technical staff were also suggested. It may be damaging to work-place moral, if two professionals doing roles of a similar nature are not being governanced is the same way and if there is not parity of their gross salary due to mandatory professional fees & reductions.
Value-for-money : This will vary between individuals depending on many variables, such as upbringing & environment, salary, lifestyle priorities, political persuasion, and so on. However, many of these factors should balance in a large sample. In general, it can be suggestive of satisfaction (or lack of) with a service. The score here suggesting dissatisfaction, echoes with other reports on HCPC’s spending, and financial irregularities [ 18 , 19 ].
In the survey findings, respondents have voiced dissatisfaction with registration value for money. In fact, HCPC’s registration fees are not high when compared to the other healthcare professions regulators. Table 1 shows data from 2021–22 for regulator annual registration fees. However, the HCPC has risen from having the lowest regulator fees in 2014–5, to its current position (9 th of 13) slightly higher in the table. Perhaps more concerning than the absolute level of fees, are when large increases are proposed [ 12 , 20 , 21 , 22 ].
However, fees have regularly increased to current figure of £196.48 for a two-year cycle. During a consultation process in 2018, the Academy for Healthcare Clinical Scientists (AHCS) wrote an open letter to the HCPC, disputing what they felt was a disproportionate fee increase [ 23 ]. Further fee rises have also been well above the level of inflation at the time.
HCPC expenditure (which is linked to registration fees) has arguably been even more controversial than fee increases – noted by several respondents. A freedom of information (FOI) request in 2016 showed HCPC’s spending of £17,000 for their Christmas party [ 18 ] – which amounts to just over £76 per person. This cost was close to the annual registration fee (at that time) for registrants.
In 2019, regulation of social workers in England moved from HCPC, to Social Work England. This resulted in a loss of over 100,000 registrants, and a loss in registration fee income. HCPC raised fees to compensate, but a freedom of information (FoI) request in 2020 [ 18 ] showed that even though there was an associated lowering in workload associated with the loss of 100 k registrants, the HCPC had no redundancies, suggesting the loss of income was compensated mainly by the fees increase.
Inherent value & relevance
One of HCPC’s aims is to promote ‘the value of regulation’ [ 24 ]. However, not only is there dissatisfaction with value-for-money, the second highest response suggests a lack of inherent value (or benefit) from regulation to the individual registrant. In some ways, there is a lack of balance – registrants are under increasing scrutiny, but feel there is little direct benefit, to provide balance.
This also suggests that HCPC’s aim or message is not getting through to the CS profession. It’s not clear what the HCPC 2021–22 achieved milestone – ‘Embedded our registrant experiences research into employee learning and development and inductions’ has actually achieved.
A large number of responses pointed to the lack of clarity about HCPC’s role, and also to note its lack of relevance for respondents. Some of this is understandable – until recently, many CS registrants will have little interaction with HCPC. They would typically get one email reminder each year to renew their registration and pay those fees, and hear little else from the HCPC. That is beginning to change, and HCPC have recently begun to send more regular, direct emails/updates to registrants.
However, for many registrants, the HCPC appears not to be clearly communicating its role, or the relevance/importance of regulation. As mentioned above, this also links in to previous mentions of the lack of any tangible benefit for registrants. Some note little more relevance other than the mandatory aspects of regulation.
Finally, relevance is also queried in relation to the limited access for some professional groups to a professional register. The current situation of gaps in registration for some groups, results in two situations – firstly, for Clinical Scientists and Clinical Engineers/Technologists, one group has to compulsorily pay a fee to be allowed/approved to do their job and the other does not; also, the public are routinely helped and assisted by Clinical Scientists and Clinical Engineers/Technologists – but only one group is regulated to ensure public safety.
HCPC Communication
This was highlighted by respondents as often poor. Recently in the media, there has been a concern raised by The College of Paramedics (CoP) about communications issues with HCPC—changes to the HCPC policy on the use of social media [ 25 ]. They raised particular concerns about the use of social media content and ‘historical content’ in the context of investigations of fitness-to practice.
There have previously been some concerns raised on the UKMPE mail-base regarding handling of personal data, and lack of efficiency in addressing the issue [ 26 ]. Several messages detailed HCPC communicating unencrypted registrant passwords in emails and sending personal data to the incorrect registrant. Some on the forum noted that they had reported this problem over a period of several years to HCPC, suggesting HCPC’s response to these serious issues was extremely slow. Several responses noted these previous issues.
Registration processes
Although responses here show some satisfaction, there have been reports in the media of significant issues with registration (such as removing registrants from the register in error) with associated impact for patients and the public [ 27 , 28 ]. Similarly, there were reports on the UKMPE mail-base of significant issues with registration renewals being problematic [ 26 ]. In Scotland, NHS.net email accounts ceased to be supported in July-Sept 2020 and the associated lack of access to email accounts and messages used for HCPC communication and registration, caused a major issue in registration renewal. This coincided with COVID lockdowns and a period of unusually difficult communication with HCPC. If NHS staff lose registration (irrespective of the reason), respondents noted that some Human Resources (HR) departments were quick to suspend staff from work, and in some cases withhold pay. That spike in difficulties is likely the cause of the most common responses suggesting issues with a complicated process.
In safe-guarding public safety, a key task for a healthcare regulator is assessing the competence of registrants. This is done via a small set of related activities. Registrants must return regular evidence of CPD, and these are audited for 2.5% registrants. This process is simple and routine, and as seen in Theme 2 responses here suggest registrants are reasonably satisfied with this process.
More formal and in-depth competence assessment happens when a complaint is raised against a registrant, either by a work colleague/management, a member of the public or occasionally by the HCPC itself. The process is complex, lengthy and can end in a registrant attending a court hearing [ 29 ].
It is usual for registrants to continue in their normal job during FTP investigations – effectively the public remains at risk from a registrant if their competence is eventually proven to be below the regulators standards, so there is a need for investigations to be efficient both in timeliness, and outcome.
Obviously, being under investigation can be highly stressful, and has the potential for the registrant to be ‘struck off’ the register, and lose their job if registration is mandated (e.g. NHS posts). There are many reports of the process & experience either provoking or increasing underlying mental health challenges [ 30 , 31 , 32 ]. Along with efficiency, a regulator needs to behave compassionately. Investigations of highly-skilled professionals engaging in complex work activities, is also necessarily complex and requires a high degree of knowledge and experience from the regulator’s investigational panel.
The Professional Standards Authority (PSA) regulate the HCPC, and publish annual reviews of their performance ( https://www.professionalstandards.org.uk/publications/performance-reviews ) (see Table 4 ). HCPC performance as reported by PSA, seems to be generally higher than noted by survey respondents here. For 2022–23, aside from one area, the HCPC has scored 100% for performance, which seems at odds with these survey responses [ 33 ]. The FTP team is notable in repeatedly performing very poorly compared to most other sections of the HCPC (even though the majority of the HCPC budget goes to FTP activity, see Fig. 4 ). The HCPC Annual Report 2018–9 [ 34 ] highlighted the completion of the first phase of the Fitness-To-Practice Improvement Plan. This delivered “A root and branch review of this regulatory function… a restructure, tightened roles and processes and the introduction of a new Threshold Policy”, but this seems to have no impact on the performance reported by the PSA for the next few years shown in Table 4 . However, the most recent data does suggest improvement, and HCPC continues to develop FTP team practice [ 17 ].

HCPC expenditure for the year 2020–21 [ 17 ]
There are other reports of poor experiences with this team [ 35 , 36 ], and in one report the FTP team’s processes have been noted as being rather inhumane [ 35 ].
Regulation is an important part of public protection, but how effectively it is managed & enforced is also a concern, given it involves increased scrutiny of registrants. A topical comparator is the current dissatisfaction by a large section of the public about several other government regulators allowing seemingly poor performance to go unchecked [ 4 , 5 ].
It is arguable, that registrants remain on the register as long as the HCPC allows them. Several respondents in this survey noted being removed from the register through HCPC administrative error. Removal could also happen through poor judgement/decision-making – the FTP team handle large numbers of very complex investigational cases – 1603 concluded cases for the year 2021–22 and 1024 hearings [ 16 ]. Every justice system is subject to a level of error – guilty parties can be erroneously ‘cleared’, and vice-versa. It is essential therefore, that policies & procedures relating to FTP are fit for purpose—that the FTP team work effectively and humanely, and that there is genuine & effective governance of HCPC to ensure accountability. In this survey, some respondents seem to be saying that currently this seems not to be the case.
It might have been anticipated that the greatest concern is costs, especially in the current cost-of-living crisis. The recent HCPC consultation to increase fees [ 37 ] seems particularly tone-deaf and has caused concern across the professions [ 21 , 22 ].
Above findings show respondents are interested in lower fees, but also increased benefit for their fees. Some respondents pointed out that whilst registrants pay for registration, benefit is mainly for the public and employers. The HCPC is a statutory body, its funding model will have been designed/decided upon by government, and may be unlikely to change. However, there are a variety of potential regulation models [ 38 ], and so change is possible. A review of the financial model for regulation may be welcome.
Regulator size
Some aspects of HCPC performance, policies, and distribution of spending, is related to the nature of it being the largest and only multi-professional regulator in the healthcare sector. Data from the HCPC suggests (see Fig. 5 ) that the majority of spending relates to FTP activity. Data also points to Clinical Scientists having very low levels of FTP investigation compared to others in HCPC [ 16 ]. This suggests that a significant proportion of CS registrant fees are used to investigate other professions. It’s possible (perhaps simplistically) that if, like many other healthcare professions such as doctors & dentists who’s regulator is concerned only with that single profession, if CSs were regulated separately, their registrant fees may be reduced. This model of single-profession regulation may also mitigate against other disadvantages of the HCPC’s practice, such as the ‘generic’ policies aiming to apply to a pool of 15 professions.
Although there is a very low level of data for this topic, the concerned raised by registrants are serious in nature. There also seems to be issues in handling of complaints related to this service and advocacy for registrants. Certainly, there is a clear governance path via PSA, to the Health Secretary. However, this does not offer a route for individual complaints to be raised and addressed. Unlike complaints from the public in other areas, there is no recourse to an ombudsman for registrants. The only option for individual registrants, is the submission of a formal complaint to the HCPC itself, which is dealt with internally. Comments from survey respondents suggest this process does not guarantee satisfaction. Indeed, one of the respondents who mentioned submitting a complaint, made it clear they remained unhappy with HCPC’s response. Overall, there seems to be a lack of clear & effective advocacy for registrants.
“…the HCPC’s stance appeared to be guilty until proven innocent… At no point did I feel the HCPC cared that their (sic) was an individual involved....” Resp044.
FTP processes affect a comparatively small number of CS registrants, compared to other professions. However, it seems clear that the majority of those who have interacted with the FTP team have had poor experiences, and respondents have suggested improvements are needed. The reason for FTP investigations, is protection of staff and the public. If processes are slow, and investigations prolonged, or decisions flawed, the public may be exposed to increased levels of risk, as healthcare practitioners who may be lacking in competence continue to practice. The data in Table 4 shows concerning but improving trends in FTP performance levels.
Limitations
There are two main limitations to this work. Firstly, due to time constraints, there was no pilot work done when designing the survey questionnaire. This may have helped, as noted earlier, a few responses pointed to some awkwardness with one survey question. Although no pilot work was done, the questionnaire was reviewed by the IPEM Professional Standards Committee, as noted in the Acknowledgements section.
The other obvious limitation is the low response rate (~ 6% of UK Medical Physicists). Circulation of the survey was performed via the only online forum for the profession currently available. The survey was advertised multiple times to ensure visibility to staff who may have missed it initially due to leave etc. However, the forum does reach 100% of the profession, and some addressees may have filters set to send specific posts to junk folders etc. The professional body IPEM declined to offer support in circulating the survey (believing the issues involved would affect/be of interest only to a small minority of members.)
The low response rate also has a particular impact on the pool of responses relating to FTP issues, which inherently affect low numbers of registrants.
However, the importance of some of the findings here (e.g. expressed dissatisfaction with regulation in terms of value; the poor experience of some members with the Registration, Communication and FTP teams) and the low sample surveyed, both justify the need for a larger follow-on survey, across all of Clinical Science.
In Healthcare, regulation of professions is a key aspect of protecting the public. However, to be effective, regulation must be performed professionally, impartially, and associated concerns or complaints investigated efficiently and respectfully.
This report presents findings from a survey aimed at collecting a snap-shot of the experiences of Clinical Scientists with their regulator, and their perception of the quality and safety of that regulation performance.
Overall survey sentiment scores showed a significantly more negative responses than positive. Survey comments relate not only to current issues, but to previous problems and controversial issues [ 18 , 26 ]. It seems that some respondents have at some point lost confidence and trust in the HCPC, and survey responses suggest there has not been enough engagement and work done by HCPC to repair and rebuild this trust.
In the midst of a cost of living crisis, costs are a large concern for many. The HCPC fees are neither the highest not lowest amongst the healthcare regulators. Spending is transparent, and details can be found in any of the HCPC’s annual reports.
A repeating sub-theme in responses, was a lack of tangible value for the registrant, and that the employer should pay the costs of registration, where registration is mandated by the job.
Many respondents have suggested that they feel there should be more proactive engagement from HCPC with the profession. Most respondents were not familiar with or felt the HCPC policies are relevant/important to them.
Survey data showed moderate satisfaction with registration processes for the majority of respondents. Some respondents also noted a lack of registration route for engineering & technical healthcare staff. CPD processes also achieved a score indicating registrant satisfaction. This generated the highest ratings in the survey. Communication scored poorly and many respondents suggests there needs to be improved levels of communication in terms of response times and access to support.
The CS profession experiences low levels of interaction with the FTP service. However, those interactions which were recorded in the survey, show some poor experiences for registrants. There also seems to be a lack of advocacy/route for complaints about HCPC from individual registrants. There may need to be more engagement between registrants and their professional body regarding HCPC performance, and more proactivity from the stake-holder, IPEM.
Some of the findings reported here relate to important issues, but the survey data are based on a low response rate. A larger survey across all of Clinical Science is being planned.
Availability of data and materials
To protect confidentiality of survey respondents, the source data is not available publicly, but are available from the author on reasonable request.
Abbreviations
Agenda for Change
Academy for Healthcare Clinical Scientists
Continuous professional development
Clinical Engineer
Clinical Scientist
College of Paramedics
Clinical Technologist
Freedom of Information
Fitness-to-practice
Health and Care Professions Council
Human resources
Institute of Physics and Engineering in Medicine
Joint Information Systems Committee
Medical Technical Officer
Professional Standards Authority
Professional Standards Committee
Qualitative data analysis
UK Medical Physics and Engineering
Professional Standards Authority. Professional healthcare regulation in the UK. https://www.professionalstandards.org.uk/news-and-blog/blog/detail/blog/2018/04/10/professional-healthcare-regulation-explained#:~:text=Regulation%20is%20simply%20a%20way,may%20face%20when%20receiving%20treatment . Accessed 26 Jul 2023
Evening Standard. Bogus surgeon treated hundreds. https://www.standard.co.uk/hp/front/bogus-surgeon-treated-hundreds-6326549.html . Accessed 26 Jul 2023.
HCPC . About registration: protected titles. http://www.hcpc-uk.org/aboutregistration/protectedtitles/ . Accessed 27 Jul 23.
The Guardian. Public patience is wearing thin. Ofwat must wield the big stick | Nils Pratley | https://www.theguardian.com/business/nils-pratley-on-finance/2022/dec/08/public-patience-is-wearing-thin-ofwat-must-wield-the-big-stick . Accessed 19 Jul 2023.
TrustPilot. Reviews of Ofgem. Ofgem Reviews | Read Customer Service Reviews of ofgem.com (trustpilot.com). Accessed 19 Jul 2023.
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
Article Google Scholar
Kiger ME, Varpio L. Thematic analysis of qualitative data: AMEE Guide No. 131. Med Teach. 2020;42(8):846–54.
Article PubMed Google Scholar
Declaration of Helsinki. 2013. https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ . Accessed 12 Sept 2023.
UK Data Protection Act. 2018. https://www.gov.uk/data-protection . Accessed 15 Sept 2023.
Rowbottom C. Private communication on behalf of the IPEM Professional Standards Committee; 2022.
IPEM Workforce Team. Clinical scientist & engineer workforce data. Personal communication. 2022.
Unison. HCPC fee increase is an unjustified ‘tax on practising.’ https://www.unison.org.uk/news/press-release/2019/02/hcpc-fee-increase-unjustified-tax-practising/ . Accessed 27 Jul 2023.
HCPC. Direct debit collection errors. https://www.hcpc-uk.org/news-and-events/news/2020/early-direct-debit-collections/?dm_i=2NJF,141CO,7C0ZNI,4A8IE,1 . Accessed 27 Jul 23.
HCPC. CPD audit rates. https://www.hcpc-uk.org/cpd/cpd-audits/ . Accessed 21 Jul 2023.
IPEM. CPD audit rates. https://www.ipem.ac.uk/your-career/cpd-career-development/cpd-audit/ . Accessed 21 Jul 2023.
HCPC. Fitness to practice annual report 2020–21. https://www.hcpc-uk.org/about-us/insights-and-data/ftp/fitness-to-practise-annual-report-2020-21/ . Accessed 23 Jul 2023.
HCPC. Annual report and accounts, 2020–21. https://www.hcpc-uk.org/resources/reports/2022/annual-report-and-accounts-2020-21/ . Accessed 19 Jul 2023.
Wikipedia. The health and care professions council. https://en.wikipedia.org/wiki/Health_and_Care_Professions_Council . Accessed 2 Jul 23.
HCPC. Annual report 2005–06. https://www.hcpc-uk.org/resources/reports/2006/annual-report-2005-06/ . Accessed 19 Jul 2023.
British Dental Association. BDA very disappointed by HCPC decision to raise registration fees by 18%. https://www.bda.uk.com/resource/bda-very-disappointed-by-hcpc-decision-to-raise-registration-fees-by-18.html . Accessed 27 Jul 2023.
British Psychological Society. HCPC fees consultation – share your views. https://www.bps.org.uk/news/hcpc-fee-consultation-share-your-views . Accessed 27 Jul 23.
IBMS. IBMS response to the HCPC registration fees consultation. https://www.ibms.org/resources/news/ibms-response-to-hcpc-registration-fees-consultation/ . Accessed 17 Jul 23.
Association of HealthCare Scientists. Open letter to HCPC. https://www.ahcs.ac.uk/wp-content/uploads/2018/11/HCPC-Open-Letter.pdf . Accessed 27 Jul 23.
HCPC. Corporate plan 2022–23. https://www.hcpc-uk.org/resources/reports/2022/hcpc-corporate-plan-2022-23/ . Accessed 23 Jul 2023.
College of Paramedics. Our formal response to the HCPC consultation. https://collegeofparamedics.co.uk/COP/News/2023/Our%20formal%20response%20to%20the%20HCPC%20consultation.aspx . Accessed 27 Jul 23.
JISC Mail - MPE mailbase. JISCMail - Medical-physics-engineering list at www.jiscmail.ac.uk . Accessed 19 July 2023.
The Guardian. Thousands miss out on treatment as physiotherapists are taken off UK register. https://www.theguardian.com/society/2022/may/14/thousands-miss-out-on-treatment-as-physiotherapists-are-struck-off-uk-register . Accessed 27 Jul 2023.
HSJJobs.com. https://www.hsjjobs.com/article/thousands-of-clinicians-unable-to-work-after-registration-blunder . Accessed 27 Jul 2023.
HCPC. How we investigate. https://www.hcpc-uk.org/concerns/how-we-investigate/ . Accessed 21 Nov 2023.
Sirriyeh R, Lawton R, Gardner P, Armitage G. Coping with medical error: a systematic review of papers to assess the effects of involvement in medical errors on healthcare professionals’ psychological well-being. Br Med J Qual Saf. 2010;19:6.
Google Scholar
Bourne T, Wynants L, Peters M, van Audenhove C, Timmerman D, van Calster B, et al. The impact of complaints procedures on the welfare, health and clinical practise of 7926 doctors in the UK: a cross-sectional survey. BMJ Open. 2015;5:e006687.
Article PubMed PubMed Central Google Scholar
Jones-Berry S. Suicide risk for nurses during fitness to practice process. Ment Health Pract. 2016;19:8.
Professional Standards Authority. HCPC performance review 2022–23. https://www.professionalstandards.org.uk/publications/performance-review-detail/periodic-review-hcpc-2022-23 . Accessed 25 Jul 2023
HCPC. Annual report and accounts, 2018–19. https://www.hcpc-uk.org/resources/reports/2019/hcpc-annual-report-and-accounts-2018-19/ . Accessed 19 Jul 2023.
Maben J, Hoinville L, Querstret D, Taylor C, Zasada M, Abrams R. Living life in limbo: experiences of healthcare professionals during the HCPC fitness to practice investigation process in the UK. BMC Health Serv Res. 2021;21:839–54.
Leigh J, Worsley A, Richard C, McLaughlin K. An analysis of HCPC fitness to practise hearings: fit to practise or fit for purpose? Ethics Soc Welfare. 2017;11(4):382–96.
HCPC. Consultation changes to fees. https://www.hcpc-uk.org/news-and-events/consultations/2022/consultation-on-changes-to-fees/ . Accessed 27 Jul 23
Department of Health. Review of the regulation of public health professions. London: DoH; 2010.
Download references
Acknowledgements
The author wishes to kindly acknowledge the input of Dr Carl Rowbottom (IPEM Professional Standards Committee), in reviewing the survey questions. Thanks also to Dr Nina Cockton for helpful advice on ethics and recruitment issues.
There were no sources of funding required for this work.
Author information
Authors and affiliations.
University of Glasgow, Level 2, ICE Building, Queen Elizabeth University Hospital Campus, 1345 Govan Road, Glasgow, G51 4TF, UK
Mark McJury
You can also search for this author in PubMed Google Scholar
Contributions
All work to collect, analyse & publish this survey, are the work of the author Dr Mark McJury.
Corresponding author
Correspondence to Mark McJury .
Ethics declarations
Ethics approval and consent to participate.
As this study relates to low risk, survey data, formal ethics committee approval is not required (exemption obtained from NHSGGC REC04 REC Officer Dr Judith Godden [email protected]). As the survey responses were from members of a professional body (The Institute of Medical Physics and Engineering in Medicine (IPEM) it was consulted. Its Professional Standards Committee (PSC) reviewed the survey and raised no objections. The survey questions were assessed for bias and approved unchanged (acknowledged in the manuscript). Written informed consent was obtained from all participants in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1..
The survey questionnaire has been provided as a supplementary file.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/ . The Creative Commons Public Domain Dedication waiver ( http://creativecommons.org/publicdomain/zero/1.0/ ) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
Reprints and permissions
About this article
Cite this article.
McJury, M. Experiences of UK clinical scientists (Physical Sciences modality) with their regulator, the Health and Care Professions Council: results of a 2022 survey. BMC Health Serv Res 24 , 635 (2024). https://doi.org/10.1186/s12913-024-10956-7
Download citation
Received : 06 September 2023
Accepted : 05 April 2024
Published : 16 May 2024
DOI : https://doi.org/10.1186/s12913-024-10956-7
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Regulation of professions
- Clinical scientists
- Medical physicists
BMC Health Services Research
ISSN: 1472-6963
- General enquiries: [email protected]

Increased Risk of Pedestrian Accidents with Electric and Hybrid Vehicles: A UK Study Reveals
A ccording to recent research, pedestrians are at a greater risk of being struck by electric or hybrid cars than those powered by petrol or diesel. The study, which underwent peer review and was published in the Journal of Epidemiology and Community Health, examined road casualty statistics within the UK from 2013 to 2017.
Findings from the study have shown that the likelihood of electric and hybrid vehicles being involved in pedestrian accidents is twice that of petrol or diesel vehicles. The incidence rate is even higher in urban areas, being threefold more probable compared to rural regions.
Looking into 916,713 recorded incidents that involved pedestrian injuries, it was found that the average yearly pedestrian casualty rate per 100 million vehicle miles traveled was 5.16 for electric and hybrid vehicles, as opposed to 2.40 for petrol and diesel vehicles. These findings covered 32 billion miles of electric/hybrid vehicle travel and 3 trillion miles of petrol/diesel vehicle travel.
The study emphasized the impact of road injuries on mortality rates, being the most common cause of deaths among children and young people. It also pointed out that pedestrians make up one quarter of all road fatalities.
Related Articles:
“Mr Bean” Actor’s Opinions on Slow Electric Car Adoption
Scarlett Johansson Addresses the Unauthorized Use of Her Voice by OpenAI
The researchers attributed the heightened risk specifically to the relative silence of electric and hybrid vehicles, which can be significantly harder to hear for pedestrians, especially in noisy urban settings. Additionally, they noted the potential correlation between inexperienced younger drivers being both more prone to accidents and more likely to drive an electric vehicle.
The study summarized that while more people are injured by petrol and diesel cars, electric cars represent a higher risk to pedestrians, with urban environments showing a higher incidence rate.
Despite the findings, the study authors advocated for continued support of walking and cycling for their health benefits, highlighting the need to understand and mitigate any increased risks linked to traffic injury.
In light of the growing push to transition away from petrol and diesel cars , the research calls for measures to address the increased safety risks posed by electric and hybrid vehicles. While acknowledging limitations such as a lack of data post-2017 due to technical issues with the National Travel Survey (NTS), the study’s conclusions are aimed at informing policy for improved pedestrian safety. The Department for Transport has been approached by Sky News for their input on this issue.
FAQs about Electric Vehicle Pedestrian Safety
Electric and hybrid vehicles are generally quieter than petrol or diesel cars, making them harder for pedestrians to hear, especially in busy urban areas.
The study found that pedestrian accidents involving electric and hybrid vehicles are three times more likely to occur in urban areas than in rural ones.
The pedestrian casualty rate per 100 million miles traveled is 5.16 for electric/hybrid vehicles compared to 2.40 for petrol and diesel vehicles.
Yes, the researchers advocate for walking and cycling due to their health benefits, while emphasizing the importance of mitigating traffic injury risks.
Sky News has reached out to the Department for Transport for their comments but has not yet received a response.
The recent study published in the Journal of Epidemiology and Community Health has raised significant concerns regarding pedestrian safety in relation to electric and hybrid vehicles. The research clearly indicates that these vehicles pose a greater risk to pedestrians compared to traditional petrol and diesel cars, particularly in urban areas. While the study should not dissuade the public from engaging in active transportation, such as walking and cycling, it does underscore the need for greater awareness and preventive measures to protect pedestrians as societies move towards cleaner transportation technologies. Future policy-making and vehicle design must account for these findings to ensure the transition to electric vehicles does not come at the cost of public safety.

Technological advances and challenges of reclaimed asphalt pavement (RAP) application in road engineering—a bibliometric analysis from 2000 to 2022
- Research Article
- Published: 11 May 2024
Cite this article

- Qi Jiang 1 ,
- Wei Liu 1 &
- Shaopeng Wu 1
180 Accesses
Explore all metrics
Reclaimed asphalt pavement (RAP) is a valuable material that can be recycled and reused in road engineering to reduce environmental impact, resource utilization, and economic costs. However, the application of RAP in road engineering presents both opportunities and challenges. This study visually analyzes the knowledge background, research status, and latest knowledge structure of literature related to RAP using scientific metric methods such as VOSviewer and Citespace. The Web of Science (WoS) core collection database identified 2963 research publications from 2000 to 2022. Collaborative networks between highly cited references, journals, authors, academic institutions, countries, and funding organizations are analyzed in this study, along with a co-occurrence analysis of keywords for the RAP research publications. Results showed that the USA has long been a leader in RAP research, China surpassed the USA in annual publication output in 2019, increasing from 2 publications in 2002 to 177 publications in 2022, and has made significant investments in technological aspects. Chang’an University ranked first in total publication output (131 publications, 4.4%). Current major research themes include road performance, recycling technology, regeneration mechanisms, and the life cycle assessment of RAP. In addition, based on cluster analysis of keywords, text content analysis, and SWOT analysis, this study also discusses RAP’s challenges and future development directions in road engineering. These findings provide scholars with valuable information to gain insight into technological advances and challenges in the field of RAP.
This is a preview of subscription content, log in via an institution to check access.
Access this article
Price includes VAT (Russian Federation)
Instant access to the full article PDF.
Rent this article via DeepDyve
Institutional subscriptions
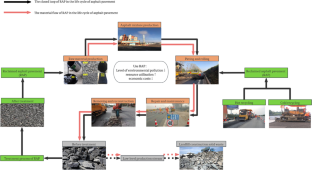
Similar content being viewed by others

A bibliometric analysis of rejuvenators in reclaimed asphalt pavement

Mapping Literature of Reclaimed Asphalt Pavement Using Bibliometric Analysis by VOSviewer

Research trends on ash stabilization in the pavement during 2002–2021
Data availability.
All the data used in this article are in the manuscript.
Aguirre MA, Hassan MM, Shirzad S, Daly WH, Mohammad LN (2016) Micro-encapsulation of asphalt rejuvenators using melamine-formaldehyde. Constr Build Mater 114:29–39
Article CAS Google Scholar
Ahmadinia E, Zargar M, Karim MR, Abdelaziz M, Ahmadinia E (2012) Performance evaluation of utilization of waste polyethylene terephthalate (PET) in stone mastic asphalt. Constr Build Mater 36:984–989
Article Google Scholar
Akbulut H, Gurer C (2007) Use of aggregates produced from marble quarry waste in asphalt pavements. Build Environ 42:1921–1930
Andersen MS (2007) An introductory note on the environmental economics of the circular economy. Sustain Sci 2:133–140
Androjic I, Kaluder G (2013) Cold recycling of asphalt pavements using foamed bitumen and cement. Gradevinar 65:463–471
Google Scholar
Antwi-Afari P, Ng ST, Hossain MU (2021) A review of the circularity gap in the construction industry through scientometric analysis. J Clean Prod 298:126870
Anuardo RG, Espuny M, Costa ACF, Oliveira OJ (2022) Toward a cleaner and more sustainable world: a framework to develop and improve waste management through organizations, governments and academia. Heliyon 8. https://doi.org/10.1016/j.heliyon.2022.e09225
Apeagyei AK, Diefenderfer BK (2013) Evaluation of cold in-place and cold central-plant recycling methods using laboratory testing of field-cored specimens. J Mater Civ Eng 25:1712–1720
Aria M, Cuccurullo C (2017) Bibliometrix: an R-tool for comprehensive science mapping analysis. J Informet 11:959–975
Arulrajah A, Piratheepan J, Disfani MM, Bo MW (2013) Geotechnical and geoenvironmental properties of recycled construction and demolition materials in pavement subbase applications. J Mater Civ Eng 25:1077–1088
Arulrajah A, Disfani MM, Horpibulsuk S, Suksiripattanapong C, Prongmanee N (2014) Physical properties and shear strength responses of recycled construction and demolition materials in unbound pavement base/subbase applications. Constr Build Mater 58:245–257
Ashtiani MZ, Mogawer WS, Austerman AJ (2018) A mechanical approach to quantify blending of aged binder from recycled materials in new hot mix asphalt mixtures. Transp Res Rec 2672:107–118
Aurangzeb Q, Al-Qadi IL (2014) Asphalt pavements with high reclaimed asphalt pavement content economic and environmental perspectives. Transp Res Rec 2456(1):161–169
Baghaee Moghaddam T, Baaj H (2016) The use of rejuvenating agents in production of recycled hot mix asphalt: a systematic review. Constr Build Mater 114:805–816
Balaguera A, Carvajal GI, Alberti J, Fullana-i-Palmer P (2018) Life cycle assessment of road construction alternative materials: a literature review. Resour Conserv Recycl 132:37–48
Behnood A (2019) Application of rejuvenators to improve the rheological and mechanical properties of asphalt binders and mixtures: a review. J Clean Prod 231:171–182
Bhatt Y, Ghuman K, Dhir A (2020) Sustainable manufacturing. Bibliometrics and content analysis. J Clean Prod:260
Bonaquist R (2007) Can I run more RAP? HMAT: hot mix asphalt technology 12
Bonoli A, Degli Esposti A, Magrini C (2020) A case study of industrial symbiosis to reduce GHG emissions: performance analysis and LCA of asphalt concretes made with RAP aggregates and steel slags. Front Mater 7:572955
Bowers BF, Huang BS, Shu X, Miller BC (2014) Investigation of reclaimed asphalt pavement blending efficiency through GPC and FTIR. Constr Build Mater 50:517–523
Brand AS, Roesler JR (2015) Ternary concrete with fractionated reclaimed asphalt pavement. ACI Mater J 112:155–163
Brand AS, Roesler JR (2017) Bonding in cementitious materials with asphalt-coated particles: Part I – The interfacial transition zone. Constr Build Mater 130:171–181
Cao ZL, Chen MZ, Han XB, Wang RY, Yu JY, Xu X et al (2020) Influence of characteristics of recycling agent on the early and long-term performance of regenerated SBS modified bitumen. Constr Build Mater 237:12
Cavalli MC, Griffa M, Bressi S, Partl MN, Tebaldi G, Poulikakos LD (2016) Multiscale imaging and characterization of the effect of mixing temperature on asphalt concrete containing recycled components. J Microsc 264:22–33
Cavalli MC, Zaumanis M, Mazza E, Partl MN, Poulikakos LD (2018) Effect of ageing on the mechanical and chemical properties of binder from RAP treated with bio-based rejuvenators. Composites Part B-Eng 141:174–181
Chen JS, Wang CH, Huang CC (2009) Engineering properties of bituminous mixtures blended with second reclaimed asphalt pavements (R2AP). Road Mater Pavement Des 10:129–149
Chen J, Dan H, Ding Y, Gao Y, Guo M, Guo S et al (2021) New innovations in pavement materials and engineering: a review on pavement engineering research 2021. J Traffic Transp Eng (English Edition) 8:815–999
China MoTotPsRo (2012) Guidance of the Ministry of Transportation on accelerating the recycling of highway pavement materials. Highway Bureau
Chiu C-T, Lee M-G (2006) Effectiveness of seal rejuvenators for bituminous pavement surfaces. J Test Eval 34(5):390–394
Chung SS, Lo CWH (2003) Evaluating sustainability in waste management: the case of construction and demolition, chemical and clinical wastes in Hong Kong. Resour Conserv Recycl 37:119–145
Copeland A (2011) Reclaimed asphalt pavement in asphalt mixtures: state of the practice. Office of Research, Development, and Technology
Costa JO, Borges PHR, dos Santos FA, Bezerra ACS, Van den bergh W, Blom J. (2020) Cementitious binders and reclaimed asphalt aggregates for sustainable pavement base layers: potential, challenges and research needs. Construct Build Mater 265:120325
Daim TU, Rueda G, Martin H, Gerdsri P (2006) Forecasting emerging technologies: use of bibliometrics and patent analysis. Technol Forecast Soc Chang 73:981–1012
Ding YJ, Huang BS, Shu X, Zhang YZ, Woods ME (2016a) Use of molecular dynamics to investigate diffusion between virgin and aged asphalt binders. Fuel 174:267–273
Ding ZK, Wang YF, Zou PXW (2016b) An agent based environmental impact assessment of building demolition waste management: conventional versus green management. J Clean Prod 133:1136–1153
Ding L, Wang X, Zhang M, Chen Z, Meng J, Shao X (2021) Morphology and properties changes of virgin and aged asphalt after fusion. Constr Build Mater 291:123284
Du XY, Meng CH, Guo ZH, Yan H (2023) An improved approach for measuring the efficiency of low carbon city practice in China. Energy 268
EAPA (2022) Asphalt in Figures 2020. European Asphalt Pavement Association, Brussels
Farahzadi L, Kioumarsi M (2023) Application of machine learning initiatives and intelligent perspectives for CO2 emissions reduction in construction. J Clean Prod 384:135504
Farina A, Zanetti MC, Santagata E, Blengini GA (2017) Life cycle assessment applied to bituminous mixtures containing recycled materials: crumb rubber and reclaimed asphalt pavement. Resour Conserv Recycl 117:204–212
Garcia A, Jelfs J, Austin CJ (2015) Internal asphalt mixture rejuvenation using capsules. Constr Build Mater 101:309–316
Garcia-Morales M, Partal P, Navarro FJ, Martinez-Boza F, Gallegos C (2004) Linear viscoelasticity of recycled EVA-modified bitumens. Energy Fuel 18:357–364
García-Morales M, Partal P, Navarro FJ, Gallegos C (2006) Effect of waste polymer addition on the rheology of modified bitumen. Fuel 85:936–943
Giani MI, Dotelli G, Brandini N, Zampori L (2015) Comparative life cycle assessment of asphalt pavements using reclaimed asphalt, warm mix technology and cold in-place recycling. Resour Conserv Recycl 104:224–238
Grinys A, Sivilevicius H, Dauksys M (2012) tyre rubber additive effect on concrete mixture strength. J Civ Eng Manag 18:393–401
Gu J, Liu X, Zhang Z (2023) Road base materials prepared by multi-industrial solid wastes in China: a review. Constr Build Mater 373:130860
Hajj EY, Sebaaly PE, Kandiah P (2010) Evaluation of the use of reclaimed asphalt pavement in airfield HMA pavements. J Transp Eng-Asce 136:181–189
Hansen K, Copeland A (2013) 2nd Annual asphalt pavement industry survey on reclaimed asphalt pavement, reclaimed asphalt shingles, and warm-mix Asphalt Usage: 2009–2011. Reclaimed Asphalt Pavements
Hasan U, Whyte A, Al JH (2020) Life cycle assessment of roadworks in United Arab Emirates: recycled construction waste, reclaimed asphalt pavement, warm-mix asphalt and blast furnace slag use against traditional approach. J Clean Prod 257:120531
He Q, Wang G, Luo L, Shi Q, Xie J, Meng X (2017) Mapping the managerial areas of Building Information Modeling (BIM) using scientometric analysis. Int J Proj Manag 35:670–685
Hou H, Su L, Guo D, Xu H (2023) Resource utilization of solid waste for the collaborative reduction of pollution and carbon emissions: case study of fly ash. J Clean Prod 383:135449
Hoy M, Horpibulsuk S, Arulrajah A (2016) Strength development of recycled asphalt pavement – fly ash geopolymer as a road construction material. Constr Build Mater 117:209–219
Huang SC, Turner TF (2014) Aging characteristics of RAP blend binders: rheological properties. J Mater Civ Eng 26:966–973
Huang B, Li G, Vukosavljevic D, Shu X, Egan BK (2005a) Laboratory investigation of mixing hot-mix asphalt with reclaimed asphalt pavement. Transp Res Rec 1929:37–45
Huang BS, Li GQ, Vukosavjevic D, Shu X, Egan BK, Trb. (2005b) Laboratory investigation of mixing hot-mix asphalt with reclaimed asphalt pavement. Bituminous Paving Mixtures 2005:37–45
Huang BS, Shu X, Li GQ (2005c) Laboratory investigation of portland cement concrete containing recycled asphalt pavements. Cem Concr Res 35:2008–2013
Huang Y, Bird RN, Heidrich O (2007) A review of the use of recycled solid waste materials in asphalt pavements. Resour Conserv Recycl 52:58–73
Inti S, Tandon V (2021) Towards precise sustainable road assessments and agreeable decisions. J Clean Prod 323:129167
Jahanbakhsh H, Karimi MM, Naseri H, Nejad FM (2020) Sustainable asphalt concrete containing high reclaimed asphalt pavements and recycling agents: performance assessment, cost analysis, and environmental impact. J Clean Prod 244:118837
Jia XY, Huang BS, Bowers BF, Zhao S (2014) Infrared spectra and rheological properties of asphalt cement containing waste engine oil residues. Constr Build Mater 50:683–691
Jiang W, Huang Y, Sha A (2018) A review of eco-friendly functional road materials. Constr Build Mater 191:1082–1092
Jin RY, Chen Q (2019) Overview of concrete recycling legislation and practice in the United States. J Constr Eng Manag 145(4):05019004
Kalantar ZN, Karim MR, Mahrez A (2012) A review of using waste and virgin polymer in pavement. Constr Build Mater 33:55–62
Kandhal PS, Mallick RB (1998) Pavement recycling guidelines for state and local governments: participant's reference book. ROSA P
Karki P, Zhou F (2016) Effect of rejuvenators on rheological, chemical, and aging properties of asphalt binders containing recycled binders. Transp Res Rec 2574:74–82
Kirchherr J, van Santen R (2019) Research on the circular economy: a critique of the field. Resour Conserv Recycl 151:104480
Kucukvar M, Tatari O (2012) Ecologically based hybrid life cycle analysis of continuously reinforced concrete and hot-mix asphalt pavements. Transp Res Part D-Transp Environ 17:86–90
Lee HVWC, Carlson R et al (2015) Development of quality standards for inclusion of high recycled asphalt pavement content in asphalt mixtures-phase II. University of Iowa
Lee N, Chou C-P, Chen K-Y (2012) Benefits in energy savings and CO 2 reduction by using reclaimed asphalt pavement. TRID
Li J, Xiao F, Zhang L, Amirkhanian SN (2019) Life cycle assessment and life cycle cost analysis of recycled solid waste materials in highway pavement: a review. J Clean Prod 233:1182–1206
Li HB, Zhang MM, Temitope AA, Guo XY, Sun JM, Yombah M et al (2022) Compound reutilization of waste cooking oil and waste engine oil as asphalt rejuvenator: performance evaluation and application. Environ Sci Pollut Res 29:90463–90478
Li J, Yang L, He L, Guo R, Li X, Chen Y et al (2023) Research progresses of fibers in asphalt and cement materials: a review. J Road Eng 3(1):35–70
Liang X, Kurniawan TA, Goh HH, Zhang DD, Dai W, Liu H et al (2022) Conversion of landfilled waste-to-electricity (WTE) for energy efficiency improvement in Shenzhen (China): a strategy to contribute to resource recovery of unused methane for generating renewable energy on-site. J Clean Prod 369:133078
Lin J, Hong J, Huang C, Liu J, Wu S (2014) Effectiveness of rejuvenator seal materials on performance of asphalt pavement. Constr Build Mater 55:63–68
Liu K, Da Y, Wang F, Ding W, Xu P, Pang H et al (2022a) An eco-friendly asphalt pavement deicing method by microwave heating and its comprehensive environmental assessments. J Clean Prod 373:133899
Liu N, Wang Y, Bai Q, Liu Y, Wang P, Xue S et al (2022b) Road life-cycle carbon dioxide emissions and emission reduction technologies: a review. J Traffic Transp Eng (English Edition) 9:532–555
Liu Y, Ali A, Chen Y, She X (2023) The effect of transport infrastructure (road, rail, and air) investments on economic growth and environmental pollution and testing the validity of EKC in China, India, Japan, and Russia. Environ Sci Pollut Res 30:32585–32599
Long HY, Liu HY, Li XW, Chen LJ (2020) An evolutionary game theory study for construction and demolition waste recycling considering green development performance under the Chinese Government's reward-penalty mechanism. Int J Environ Res Public Health 17(17):6303
Luan Y, Ma T, Wang S, Ma Y, Xu G, Wu M (2022) Investigating mechanical performance and interface characteristics of cold recycled mixture: promoting sustainable utilization of reclaimed asphalt pavement. J Clean Prod 369:133366
Luo Z, Xiao FP, Hu SW, Yang YS (2013) Probabilistic analysis on fatigue life of rubberized asphalt concrete mixtures containing reclaimed asphalt pavement. Constr Build Mater 41:401–410
Ma MX, Tam VWY, Le KN, Li WG (2020) Challenges in current construction and demolition waste recycling: a China study. Waste Manag 118:610–625
MacLeod D, Ho S, Wirth R, Zanzotto L (2007) Study of crumb rubber materials as paving asphalt modifiers. Can J Civ Eng 34:1276–1288
Mannan UA, Islam MR, Tarefder RA (2015) Effects of recycled asphalt pavements on the fatigue life of asphalt under different strain levels and loading frequencies. Int J Fatigue 78:72–80
Meyer DE, Li M, Ingwersen WW (2020) Analyzing economy-scale solid waste generation using the United States environmentally-extended input-output model. Resour Conserv Recycl 157:104795
Mogawer WS, Austerman AJ, Bonaquist R (2012) Determining the influence of plant type and production parameters on performance of plant-produced reclaimed asphalt pavement mixtures. Transp Res Rec 2268:71–81
Mogawer WS, Booshehrian A, Vahidi S, Austerman AJ (2013) Evaluating the effect of rejuvenators on the degree of blending and performance of high RAP, RAS, and RAP/RAS mixtures. Road Mater Pavement Des 14:193–213
Mohamed AS, Cao ZL, Xu XY, Xiao FP, Abdel-Wahed T (2022) Bonding, rheological, and physiochemical characteristics of reclaimed asphalt rejuvenated by crumb rubber modified binder. J Clean Prod 373:133896
Ng CP, Law TH, Wong SV, Kulanthayan S (2017) Relative improvements in road mobility as compared to improvements in road accessibility and economic growth: a cross-country analysis. Transp Policy 60:24–33
Norin M, Stromvall AM (2004) Leaching of organic contaminants from storage of reclaimed asphalt pavement. Environ Technol 25:323–340
Offenbacker D, Mehta Y (2022) Assessing the life-cycle costs of pavement rehabilitation strategies used in long-term pavement performance program. J Transp Eng Part B-Pavements 148(1):04022002
Oner J, Sengoz B (2015) Utilization of recycled asphalt concrete with warm mix asphalt and cost-benefit analysis. PLoS One 10(1):e116180
Oreto C, Veropalumbo R, Viscione N, Biancardo SA, Russo F (2021) Investigating the environmental impacts and engineering performance of road asphalt pavement mixtures made up of jet grouting waste and reclaimed asphalt pavement. Environ Res 198:111277
Ozer H, Al-Qadi IL, Lambros J, El-Khatib A, Singhvi P, Doll B (2016) Development of the fracture-based flexibility index for asphalt concrete cracking potential using modified semi-circle bending test parameters. Constr Build Mater 115:390–401
Pei J, Guo F, Zhang J, Zhou B, Bi Y, Li R (2021) Review and analysis of energy harvesting technologies in roadway transportation. J Clean Prod 288:125338
Pompigna A, Mauro R (2022) Smart roads: a state of the art of highways innovations in the Smart Age. Eng Sci Technol Int J 25:100986
Pradyumna TA, Mittal A, Jain P (2013) Characterization of reclaimed asphalt pavement (RAP) for use in bituminous road construction. Procedia Soc Behav Sci 104:1149–1157
Pranav S, Lahoti M, Shan X, Yang EH, Muthukumar G (2022) Economic input-output LCA of precast corundum-blended ECC overlay pavement. Resour Conserv Recycl 184:106385
Puccini M, Leandri P, Tasca AL, Pistonesi L, Losa M (2019) Improving the environmental sustainability of low noise pavements: comparative life cycle assessment of reclaimed asphalt and crumb rubber based warm mix technologies. Coatings 9(5):343
Puppala AJ, Hoyos LR, Potturi AK (2011) Resilient moduli response of moderately cement-treated reclaimed asphalt pavement aggregates. J Mater Civ Eng 23:990–998
Qiao YN, Dave E, Parry T, Valle O, Mi LY, Ni GD et al (2019) Life cycle costs analysis of reclaimed asphalt pavement (RAP) under future climate. Sustainability 11(19):5414
Rafiq W, Napiah M, Habib NZ, Sutanto MH, Alaloul WS, Khan MI et al (2021) Modeling and design optimization of reclaimed asphalt pavement containing crude palm oil using response surface methodology. Constr Build Mater 291:123288
Rahman MA, Imteaz MA, Arulrajah A, Piratheepan J, Disfani MM (2015) Recycled construction and demolition materials in permeable pavement systems: geotechnical and hydraulic characteristics. J Clean Prod 90:183–194
Rodriguez A, Laio A (2014) Clustering by fast search and find of density peaks. Science 344:1492–1496
Rodríguez-Fernández I, Lastra-González P, Indacoechea-Vega I, Castro-Fresno D (2019) Technical feasibility for the replacement of high rates of natural aggregates in asphalt mixtures. Int J Pavement Eng 22(8):940–949
Roja KL, Masad E, Vajipeyajula B, Yiming W, Khalid E, Shunmugasamy VC (2020) Chemical and multi-scale material properties of recycled and blended asphalt binders. Constr Build Mater 261:119689
Roja KL, Masad E, Mogawer W (2021) Performance and blending evaluation of asphalt mixtures containing reclaimed asphalt pavement. Road Mater Pavement Des 22:2441–2457
Sabouri M, Kim YR (2014) Development of a failure criterion for asphalt mixtures under different modes of fatigue loading. Transp Res Rec 2447:117–125
Sanchez X, Tighe SL (2019) Steps towards the detection of reclaimed asphalt pavement in superpave mixtures. Road Mater Pavement Des 20:1201–1214
Santero NJ, Masanet E, Horvath A (2011) Life-cycle assessment of pavements. Part I: Critical review. Resour Conserv Recycl 55:801–809
Sarah Mariam A, Ransinchung GDRN (2020) Laboratory research on reclaimed asphalt pavement-inclusive cementitious mixtures. ACI Mater J 117:193
Sha A, Liu Z, Jiang W, Qi L, Hu L, Jiao W et al (2021) Advances and development trends in eco-friendly pavements. J Road Eng 1:1–42
Shao-peng W, Xiao-ming H, Yong-li Z (2002) The development of recycling agent for asphalt pavement. J Wuhan Univ Technol-Mater Sci Ed 17:63–65
Shen DH, Du JC (2005) Application of gray relational analysis to evaluate HMA with reclaimed building materials. J Mater Civ Eng 17:400–406
Shi C, Meyer C, Behnood A (2008) Utilization of copper slag in cement and concrete. Resour Conserv Recycl 52:1115–1120
Shirodkar P, Mehta Y, Nolan A, Sonpal K, Norton A, Tomlinson C et al (2011) A study to determine the degree of partial blending of reclaimed asphalt pavement (RAP) binder for high RAP hot mix asphalt. Constr Build Mater 25:150–155
Shu X, Huang BS (2014) Recycling of waste tire rubber in asphalt and portland cement concrete: an overview. Constr Build Mater 67:217–224
Shu X, Huang B, Vukosavljevic D (2008) Laboratory evaluation of fatigue characteristics of recycled asphalt mixture. Constr Build Mater 22:1323–1330
Shu X, Huang BS, Shrum ED, Jia XY (2012) Laboratory evaluation of moisture susceptibility of foamed warm mix asphalt containing high percentages of RAP. Constr Build Mater 35:125–130
Silva H, Oliveira JRM, Jesus CMG (2012) Are totally recycled hot mix asphalts a sustainable alternative for road paving? Resour Conserv Recycl 60:38–48
Singh S, Ransinchung GD, Kumar P (2017) An economical processing technique to improve RAP inclusive concrete properties. Constr Build Mater 148:734–747
Sivilevicius H, Braziunas J, Prentkovskis O (2017) Technologies and principles of hot recycling and investigation of preheated reclaimed asphalt pavement batching process in an asphalt mixing plant. Applied Sciences-Basel 7:20
Song W, Huang B, Shu X (2018) Influence of warm-mix asphalt technology and rejuvenator on performance of asphalt mixtures containing 50% reclaimed asphalt pavement. J Clean Prod 192:191–198
Su J-F, Qiu J, Schlangen E (2013) Stability investigation of self-healing microcapsules containing rejuvenator for bitumen. Polym Degrad Stab 98:1205–1215
Sudarsanan N, Kim YR (2022) A critical review of the fatigue life prediction of asphalt mixtures and pavements. J Traffic Transp Eng (English Edition) 9:808–835
Sun LC, Wang QW, Zhang JJ (2017) Inter-industrial carbon emission transfers in China: economic effect and optimization strategy. Ecol Econ 132:55–62
Sun Y, Zheng L, Cheng Y, Chi F, Liu K, Zhu T (2023) Research on maintenance equipment and maintenance technology of steel fiber modified asphalt pavement with microwave heating. Case Stud Constr Mater 18:e01965
Thakur JK, Han J, Pokharel SK, Parsons RL (2012) Performance of geocell-reinforced recycled asphalt pavement (RAP) bases over weak subgrade under cyclic plate loading. Geotext Geomembr 35:14–24
Townsend TG, Ingwersen WW, Niblick B, Jain P, Wally J (2019) CDDPath: a method for quantifying the loss and recovery of construction and demolition debris in the United States. Waste Manag 84:302–309
Tran NP, Nguyen TN, Ngo TD (2022) The role of organic polymer modifiers in cementitious systems towards durable and resilient infrastructures: a systematic review. Constr Build Mater 360:129562
Umer A, Hewage K, Haider H, Sadiq R (2017) Sustainability evaluation framework for pavement technologies: an integrated life cycle economic and environmental trade-off analysis. Transp Res Part D-Transp Environ 53:88–101
Vignisdottir HR, Ebrahimi B, Booto GK, O'Born R, Brattebø H, Wallbaum H et al (2019) A review of environmental impacts of winter road maintenance. Cold Reg Sci Technol 158:143–153
Vislavicius K, Sivilevicius H (2013) Effect of reclaimed asphalt pavement gradation variation on the homogeneity of recycled hot-mix asphalt. Arch Civil Mech Eng 13:345–353
Waltman L, van Eck NJ, Noyons ECM (2010) A unified approach to mapping and clustering of bibliometric networks. J Informet 4:629–635
Wang C, Lim MK, Zhang X, Zhao L, Lee PT-W (2020) Railway and road infrastructure in the Belt and Road Initiative countries: estimating the impact of transport infrastructure on economic growth. Transp Res A Policy Pract 134:288–307
Wang FS, Xie J, Wu SP, Li JS, Barbieri DM, Zhang L (2021) Life cycle energy consumption by roads and associated interpretative analysis of sustainable policies. Renew Sustain Energy Rev 141:110823
Wang L, Wei J, Wu W, Zhang X, Xu X, Yan X (2022) Technical development and long-term performance observations of long-life asphalt pavement: a case study of Shandong Province. J Road Eng 2:369–389
Wei M, Wu S, Zhu L, Li N, Yang C (2021) Environmental impact on VOCs emission of a recycled asphalt mixture with a high percentage of RAP. Materials 14
Williams B, Willis J (2022) Asphalt pavement industry survey on recycled materials and warm-mix asphalt usage 2020 Information Series 138 11th Annual Survey
Willis J, Williams B (2022) Asphalt pavement industry survey on recycled materials and warm-mix asphalt usage 2021 Information Series 138 12th Annual Survey
Wu SP, Xue YJ, Ye QS, Chen YC (2007) Utilization of steel slag as aggregates for stone mastic asphalt (SMA) mixtures. Build Environ 42:2580–2585
Wu M, Xu GJ, Luan YC, Zhu YJ, Ma T, Zhang WG (2022) Molecular dynamics simulation on cohesion and adhesion properties of the emulsified cold recycled mixtures. Constr Build Mater 333:127403
Xiang C, Wang Y, Liu H (2017) A scientometrics review on nonpoint source pollution research. Ecol Eng 99:400–408
Xiao FP, Amirkhanian S, Juang CH (2007) Rutting resistance of rubberized asphalt concrete pavements containing reclaimed asphalt pavement mixtures. J Mater Civ Eng 19:475–483
Xiao F, Su N, Yao S, Amirkhanian S, Wang J (2019) Performance grades, environmental and economic investigations of reclaimed asphalt pavement materials. J Clean Prod 211:1299–1312
Xiao F, Xu L, Zhao Z, Hou X (2023) Recent applications and developments of reclaimed asphalt pavement in China, 2010–2021. Sustain Mater Technol 37:e00697
CAS Google Scholar
Xiao FP, Yao SL, Wang JG, Li XH, Amirkhanian S (2018) A literature review on cold recycling technology of asphalt pavement. Constr Build Mater 180:579–604
Xie ZX, Tran N, Taylor A, Julian G, West R, Welch J (2017) Evaluation of foamed warm mix asphalt with reclaimed asphalt pavement: field and laboratory experiments. Road Mater Pavement Des 18:328–352
Xing C, Li M, Liu L, Lu R, Liu N, Wu W et al (2023) A comprehensive review on the blending condition between virgin and RAP asphalt binders in hot recycled asphalt mixtures: mechanisms, evaluation methods, and influencing factors. J Clean Prod 398:136515
Xu B, Ding R, Yang Z, Sun Y, Zhang J, Lu K et al (2023) Investigation on performance of mineral-oil-based rejuvenating agent for aged high viscosity modified asphalt of porous asphalt pavement. J Clean Prod 395:136285
Yao LY, Leng Z, Lan JT, Chen RQ, Jiang JW (2022) Environmental and economic assessment of collective recycling waste plastic and reclaimed asphalt pavement into pavement construction: a case study in Hong Kong. J Clean Prod 336:130405
Yao Y, Yang J, Gao J, Zheng M, Xu J, Zhang W et al (2023) Strategy for improving the effect of hot in-place recycling of asphalt pavement. Constr Build Mater 366:130054
Yousefi A, Behnood A, Nowruzi A, Haghshenas H (2021) Performance evaluation of asphalt mixtures containing warm mix asphalt (WMA) additives and reclaimed asphalt pavement (RAP). Constr Build Mater 268:121200
Yu XK, Zaumanis M, dos Santos S, Poulikakos LD (2014) Rheological, microscopic, and chemical characterization of the rejuvenating effect on asphalt binders. Fuel 135:162–171
Yu B, Wang SY, Gu XY (2018) Estimation and uncertainty analysis of energy consumption and CO 2 emission of asphalt pavement maintenance. J Clean Prod 189:326–333
Yuan HP (2017) Barriers and countermeasures for managing construction and demolition waste: a case of Shenzhen in China. J Clean Prod 157:84–93
Zaumanis M, Mallick RB (2015) Review of very high-content reclaimed asphalt use in plant-produced pavements: state of the art. Int J Pavement Eng 16:39–55
Zaumanis M, Mallick RB, Frank R (2013) Evaluation of rejuvenator's effectiveness with conventional mix testing for 100% reclaimed asphalt pavement mixtures. Transp Res Rec:17–25
Zaumanis M, Mallick RB, Frank R (2014a) 100% recycled hot mix asphalt: a review and analysis. Resour Conserv Recycl 92:230–245
Zaumanis M, Mallick RB, Poulikakos L, Frank R (2014b) Influence of six rejuvenators on the performance properties of reclaimed asphalt pavement (RAP) binder and 100% recycled asphalt mixtures. Constr Build Mater 71:538–550
Zhang J, Guo C, Chen T, Zhang W, Yao K, Fan C et al (2021) Evaluation on the mechanical performance of recycled asphalt mixtures incorporated with high percentage of RAP and self-developed rejuvenators. Constr Build Mater 269:121337
Zhang Y, Wang J, Deng H, Zhang D, Wang Y (2023) Developing a multidimensional assessment framework for clean technology transfer potential and its application on the belt and road initiative countries. J Clean Prod 401:136769
Zhao S, Huang B, Shu X, Woods M (2013) Comparative evaluation of warm mix asphalt containing high percentages of reclaimed asphalt pavement. Constr Build Mater 44:92–100
Zhao S, Huang BS, Shu X, Woods ME (2016) Quantitative evaluation of blending and diffusion in high RAP and RAS mixtures. Mater Des 89:1161–1170
Zheng XW, Xu WY, Xu HP, Wu SX, Cao K (2022) Research on the ability of bio-rejuvenators to disaggregate oxidized asphaltene nanoclusters in aged asphalt. Acs Omega 7:21736–21749
Download references
This work was supported by the National Natural Science Foundation of China (No. 51778515 and No. 71961137010), the Technological Innovation Major Project of Hubei Province (2019AEE023), the Key R&D Program of Hubei Province (2020BCB064), and the State Key Laboratory of Silicate Materials for Architectures (Wuhan University of Technology, No. SYSJJ2019-20).
Author information
Authors and affiliations.
State Key Laboratory of Silicate Materials for Architectures, Wuhan University of Technology, Wuhan, 430070, China
Qi Jiang, Wei Liu & Shaopeng Wu
You can also search for this author in PubMed Google Scholar
Contributions
All authors contributed to the study’s conception and design. Visualization and supervision were performed by Wei Liu and Shaopeng Wu. Review and editing were performed by Qi Jiang and Wei Liu. Project administration was performed by Shaopeng Wu. The first draft of the manuscript was written by Qi Jiang, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Correspondence to Qi Jiang .
Ethics declarations
Ethics approval.
Not applicable.
Consent to participate
All authors agreed to participate in this study.
Consent for publication
All authors agree to publish.
Conflict of interest
The authors declare no conflict of interest.
Additional information
Responsible Editor: Philippe Garrigues
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
Reprints and permissions
About this article
Jiang, Q., Liu, W. & Wu, S. Technological advances and challenges of reclaimed asphalt pavement (RAP) application in road engineering—a bibliometric analysis from 2000 to 2022. Environ Sci Pollut Res (2024). https://doi.org/10.1007/s11356-024-33635-w
Download citation
Received : 16 August 2023
Accepted : 06 May 2024
Published : 11 May 2024
DOI : https://doi.org/10.1007/s11356-024-33635-w
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
- Reclaimed asphalt pavement
- Road engineering
- Visual analysis
- Knowledge structure. SWOT analysis
- Find a journal
- Publish with us
- Track your research
- - Google Chrome
Intended for healthcare professionals
- Access provided by Google Indexer
- My email alerts
- BMA member login
- Username * Password * Forgot your log in details? Need to activate BMA Member Log In Log in via OpenAthens Log in via your institution
Search form
- Advanced search
- Search responses
- Search blogs
- Epidural analgesia...
Epidural analgesia during labour and severe maternal morbidity: population based study
Linked editorial.
Unlocking maternal health: labour epidurals and severe morbidity
- Related content
- Peer review
- Rachel J Kearns , consultant anaesthetist 1 2 ,
- Aizhan Kyzayeva , research associate 2 ,
- Lucy O E Halliday , doctoral student 2 ,
- Deborah A Lawlor , professor of epidemiology 3 4 ,
- Martin Shaw , principal clinical physicist 2 5 ,
- Scott M Nelson , Muirhead chair of obstetrics and gynaecology 2
- 1 Department of Anaesthesia, Glasgow Royal Infirmary, Glasgow, UK
- 2 School of Medicine, University of Glasgow, Glasgow Royal Infirmary, Glasgow, G31 2ER, UK
- 3 MRC Integrative Epidemiology Unit at the University of Bristol, Bristol, UK
- 4 Population Health Science, University of Bristol, Bristol, UK
- 5 Department of Medical Physics and Bioengineering, NHS Greater Glasgow and Clyde, Glasgow, UK
- Correspondence to: R J Kearns rachel.kearns{at}glasgow.ac.uk (or @rjharrison79 on X)
- Accepted 10 April 2024
Objectives To determine the effect of labour epidural on severe maternal morbidity (SMM) and to explore whether this effect might be greater in women with a medical indication for epidural analgesia during labour, or with preterm labour.
Design Population based study.
Setting All NHS hospitals in Scotland.
Participants 567 216 women in labour at 24+0 to 42+6 weeks’ gestation between 1 January 2007 and 31 December 2019, delivering vaginally or through unplanned caesarean section.
Main outcome measures The primary outcome was SMM, defined as the presence of ≥1 of 21 conditions used by the US Centers for Disease Control and Prevention (CDC) as criteria for SMM, or a critical care admission, with either occurring at any point from date of delivery to 42 days post partum (described as SMM). Secondary outcomes included a composite of ≥1 of the 21 CDC conditions and critical care admission (SMM plus critical care admission), and respiratory morbidity.
Results Of the 567 216 women, 125 024 (22.0%) had epidural analgesia during labour. SMM occurred in 2412 women (4.3 per 1000 births, 95% confidence interval (CI) 4.1 to 4.4). Epidural analgesia was associated with a reduction in SMM (adjusted relative risk 0.65, 95% CI 0.50 to 0.85), SMM plus critical care admission (0.46, 0.29 to 0.73), and respiratory morbidity (0.42, 0.16 to 1.15), although the last of these was underpowered and had wide confidence intervals. Greater risk reductions in SMM were detected among women with a medical indication for epidural analgesia (0.50, 0.34 to 0.72) compared with those with no such indication (0.67, 0.43 to 1.03; P<0.001 for difference). More marked reductions in SMM were seen in women delivering preterm (0.53, 0.37 to 0.76) compared with those delivering at term or post term (1.09, 0.98 to 1.21; P<0.001 for difference). The observed reduced risk of SMM with epidural analgesia was increasingly noticeable as gestational age at birth decreased in the whole cohort, and in women with a medical indication for epidural analgesia.
Conclusion Epidural analgesia during labour was associated with a 35% reduction in SMM, and showed a more pronounced effect in women with medical indications for epidural analgesia and with preterm births. Expanding access to epidural analgesia for all women during labour, and particularly for those at greatest risk, could improve maternal health.
Introduction
The rising incidence of severe maternal morbidity (SMM) constitutes a pressing global issue, compromising the wellbeing of mothers and their children, and resulting in potentially devastating short term and long term consequences. 1 2 SMM is defined by the US Centers for Disease Control and Prevention (CDC) as encompassing 21 indicative conditions or procedures, such as myocardial infarction, eclampsia, and hysterectomy occurring during admission to hospital for delivery. 3 In the UK, the incidence of SMM almost doubled between 2009 and 2018, from 0.9% to 1.7% of deliveries, likely reflecting the trend of mothers being older, more obese, and with increasing comorbidities, along with a rising incidence of previous caesarean delivery. 4 SMM can be conceptualised as an indicator of increased risk for maternal mortality, providing crucial opportunities to identify and implement interventions to improve the health of mothers and their offspring. 5
Epidural analgesia is commonly advised for safety reasons in pregnant women considered at higher risk of SMM, such as those with multiple births, morbid obesity (body mass index (BMI) ≥40), or certain comorbidities, owing to its advantageous physiological effects and capacity to provide expedient anaesthesia if required in an emergency. 6 Women with these factors can be considered as having a medical indication for epidural analgesia during labour. Women giving birth preterm also carry a higher risk of SMM, although epidural analgesia is seldom recommended for preterm labour alone. 7 Despite the assumed benefits of epidural analgesia during labour to prevent SMM, the evidence base for this is limited. We identified just two observational studies that attempted to delineate the association between epidural analgesia during labour and SMM. 8 9 One, a US study (n=574 525), indicated a 14% risk reduction in SMM in women who received epidural analgesia, but it only included vaginal births and excluded the six week postnatal period, during which about 15% of SMM events occur. 8 10 The other study, from France (n=4550), reported a 47% decreased risk of severe postpartum haemorrhage in women with epidural analgesia who gave birth vaginally, but it did not assess other constituents of SMM. 9 Neither of these studies explored whether the association differed between women with a medical indication and those without, or between women who delivered preterm and those who did not. In these two studies from countries with private healthcare systems, the use of epidural analgesia was 47% 8 and 78%, 9 respectively, whereas in the UK, the use of epidural analgesia during labour is around 22-30%, despite healthcare being free at the point of access. 11 12
Notwithstanding that clinicians may advise mothers with medical indications about epidural analgesia during labour, the final decision is up to the woman. The lack of robust evidence on whether benefits exist beyond the provision of epidural analgesia might affect the discussions clinicians have with women and their decisions. Women from minority ethnic groups and areas of socioeconomic deprivation are at higher risk of maternal morbidity and mortality, and they are more likely to have medical indications for epidural analgesia, but are less likely to have one. 13 14 15 Stronger evidence on the effects of epidural analgesia might contribute to reducing these inequalities. The importance of improving this evidence base is highlighted by the priority setting exercises undertaken by the James Lind Alliance, which identified the effect of epidural analgesia on obstetric outcomes as a research priority. 16 The James Lind Alliance brings patients, carers, and clinicians together to identify research priorities.
In this population based cohort analysis of all births in Scotland over a 13 year period, we estimated the causal effect of the use of epidural analgesia during labour on SMM in all mothers, except those undergoing planned caesarean section delivery. Additionally, we explored whether this effect was more pronounced among pregnant women who according to clinical guidelines are at increased risk of SMM (ie, women with a medical indication for epidural analgesia during labour), and in those with preterm labour.
Our methods are reported in accordance with Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidance. 17
Data sources and study population
We linked six Scotland-wide administrative databases: the Scottish Morbidity Record-2 (SMR02), the Scottish Morbidity Record-1 (SMR01), the Scottish Birth Record, the National Records of Scotland, the Scottish Stillbirth Infant Death Survey, and the Scottish Intensive Care Society Audit Group. The SMR02 documents all obstetric inpatient and day case admissions during pregnancy and the postnatal period and includes maternal and infant characteristics. The SMR02 is subject to regular quality assurance checks, with data more than 99% complete since the late 1970s. 18 19 The SMR01 records all non-obstetric inpatient and day case admissions according to ICD-9 and ICD-10 (international classification of diseases, ninth revision and 10th revision, respectively) codes and UK NHS OPCS-4 (Office of Population Censuses and Surveys classification of interventions and procedures). 20 21 All neonatal care is recorded in the Scottish Birth Record. The National Records of Scotland registers all births, stillbirths, and infant deaths, and the Scottish Stillbirth Infant Death Survey collects additional information from the relevant coordinator of the survey (obstetrician, paediatrician, or midwife) at each hospital. The database of the Scottish Intensive Care Society Audit Group records admission data for all Scottish intensive care and high dependency units, with regular data validation. 22
Inclusion and exclusion criteria
We analysed all women in labour in Scotland between 1 January 2007 and 31 December 2019 with gestation between 24+0 and 42+6 weeks. Births were excluded after this period to remove any potential confounding influence of the covid-19 pandemic. We also excluded births when mode of delivery, child identity, or data for analgesia during labour were not recorded (n=38 705, 5.5% of all 697 981 pregnancies considered); see supplementary eFigure 1), as well as births by elective caesarean section as these women knew their mode of delivery in advance and would not experience labour, and therefore by definition could not have chosen to have epidural analgesia (n=92 060, 13.2%; see supplementary eFigure 1).
Epidural analgesia
We defined epidural analgesia during labour as conventional lumbar epidural sited at any time during labour. This definition is consistent with standard medical practices in the UK, where epidural drugs are generally administered only after labour has commenced. We were unable to identify use of combined spinal epidural (spinal injection plus insertion of an epidural catheter), as SMR02 classifies the procedure as spinal anaesthesia. Combined spinal epidural is used infrequently in Scotland, representing only 1% of epidural use during labour. 23 Women recorded as having no epidural could have delivered without additional analgesia or anaesthesia or have required spinal or general anaesthesia for operative delivery, reflecting the unpredictability of labour outcomes and the resultant different potential pathways care may take. Since recording of anaesthetic intervention is hierarchical, we could not identify if women who had a spinal or general anaesthetic also had epidural analgesia at an earlier point. Conversion of epidural analgesia to spinal or general anaesthesia occurs in around 5% of women. 24
The primary outcome was SMM, defined as a composite outcome of ≥1 of 21 conditions according to the US CDC criteria for SMM or a critical care admission, with either occurring at any point from the date of delivery to 42 days post partum (described as SMM). In keeping with other published data, we incorporated critical care admission as an SMM indicator because the CDC’s definition does not cover all SMM events (eg, asthma attack, status epilepticus). 4 We identified conditions using ICD-9, ICD-10, and OPCS codes from SMR01, SMR02, and Scottish Intensive Care Society Audit Group datasets (see supplementary eTable 1 for table of codes). 3 The CDC’s definition of SMM has a sensitivity of 77% and specificity of 99% in identifying SMM compared with medical records. 25
Secondary outcomes aimed to capture more severe morbidity and included ≥1 of the 21 CDC conditions when that condition resulted in admission for critical care (described as SMM plus critical care), and respiratory morbidity (ventilation, tracheostomy, acute respiratory distress syndrome, or respiratory complications of anaesthesia), as diagnosed from the date of delivery to 42 days post partum (see supplementary eTable 1).
Minor modifications were made to the CDC SMM criteria to accommodate data recording practices in Scotland (see supplementary eTable 1). In line with other UK studies, 4 26 we found that the UK definition for postpartum haemorrhage (≥500 mL blood loss) resulted in over-reporting of major obstetric haemorrhage (ICD-10 code O72), and therefore we included postpartum haemorrhage only if it occurred in association with a critical care admission, indicating a clinically significant haemorrhage event. Alternative metrics such as volume of blood loss and blood transfusion are not reliably recorded in SMR02. Similar to a previous Scottish study, we found the incidence of sepsis had increased exponentially from 2012 (see supplementary eFigure 2). 4 This might reflect different coding practices and changes in guidance with the publication of the 2012 Surviving Sepsis recommendations resulting in increased awareness of the condition. 27 28 Because sepsis is defined as the presence of an infection and evidence of acute organ dysfunction, we included it only if associated with admission to a critical care unit.
Given that in our analyses, as in any risk analyses, we censored at the first SMM condition, the difference between the primary outcome and the first secondary outcome is illustrated by considering a mother with eclampsia diagnosed on the day of delivery and acute heart failure diagnosed on postnatal day 22. In the primary analysis, that woman would be censored on the day of delivery. In contrast, a woman with eclampsia diagnosed on the day of delivery who experienced heart failure resulting in critical care admission at 22 days postnatally when heart failure was diagnosed, would be censored at postnatal day 22. Conversely, a woman with the same conditions at the same time points but who was not admitted to critical care for either would not be considered at risk for the secondary outcome of SMM plus critical care admission (and would contribute to the comparator group—no SMM plus critical care).
Confounders and other variables used in analyses
To determine confounding variables before analyses, we used the established definition of a confounder—something that is a known or plausible reason for having both epidural analgesia during labour and SMM, and we considered all potential plausible pathways between these variables. 29 We included these confounders (irrespective of whether they were available in our data) in directed acyclic graphs drawn using the R package “DAGGitty,” 30 to highlight sources of unmeasured confounding and how these might be captured by other measured confounders on the same confounding path (see supplementary eFigures 3a and 3b). We included socioeconomic status and ethnicity as these factors are increasingly recognised as influencing poor maternal outcomes and epidural analgesia use during labour. 13 14 15 Ethnicity was defined using NHS Scotland 2011 census categories. 31 As we did not have information on individual socioeconomic status, we used residential area deprivation according to the Scottish index for multiple deprivation as a proxy; the first 10% of deprivation denoting the most deprived areas and the last 10% the least deprived. 32 Pre-existing comorbidities that plausibly influence the use of epidural analgesia and SMM were defined for each mother by calculating a Bateman index score, an extensively validated, weighted, risk prediction tool including 20 conditions plus maternal age that is specific to obstetric patients and more accurately predicts SMM than other generic comorbidity indices (see supplementary eTable 2) 33 To avoid conflating comorbid conditions with the outcome of SMM, we applied strict criteria, restricting these diagnoses to the period between 180 days before the estimated date of conception (as described in the original paper by Bateman et al) 33 and the day before delivery. This approach ensured the validity of our findings by accurately reflecting the impact of comorbidities on risk of SMM. Using ICD-9 and ICD-10 codes from SMR02, we obtained information on maternal height, weight, and smoking status plus obstetric indices of previous caesarean section, parity, and induction of labour. Gestational age at birth was based on ultrasound assessment in the first half of pregnancy. Smoking status at booking was defined as current, former, or never. Birth location was categorised into obstetric unit, freestanding midwifery unit, or home birth. Obstetric units were defined as hospitals with on-site obstetric and anaesthetic services, inclusive of epidural analgesia provision, or midwifery led units co-located with an obstetric unit. Freestanding midwifery units were defined as midwifery led units without direct access to obstetric or anaesthetic services. 34
In exploratory analyses we assessed whether associations differed by the presence of a medical indication for epidural analgesia and by gestational age. We classified births as preterm if they occurred before 37 weeks’ gestation and as term or post term if they occurred at ≥37+0 weeks. Births were further classified using World Health Organization (WHO) criteria as extremely preterm (<28 weeks), very preterm (28 to <32 weeks), and moderate to late preterm (≥32 to 36+6 weeks), and by whether labour occurred spontaneously or was commenced iatrogenically. 35
We defined medical indications for epidural analgesia as any of serious cardiovascular or respiratory disease (congestive heart failure, congenital heart disease, pulmonary hypertension, ischaemic heart disease, asthma); pre-eclampsia; previous caesarean section; breech presentation; multiple pregnancy; and morbid obesity (BMI ≥40), diagnosed before the date of delivery and with no contraindication to epidural insertion (see supplementary eTable 3). 6 36 37 38 39 40 41 These indications are easily identified by obstetric, anaesthesia, and midwifery staff, reflect criteria that drive common decision making processes, and are in widespread use in clinical practice. These conditions were included if recorded up to the day pre-delivery to ensure they occurred before the decision to have an epidural and any episodes of SMM.
Statistical analysis
As this was a whole population study, we did not perform sample size calculations. We report baseline characteristics by epidural status. Continuous variables are expressed as medians with interquartile range (IQR), and categorical variables as counts and percentages. For group comparison, we used standardised differences.
To adjust for confounders, we used multivariable Poisson regression models with cluster robust sandwich estimators under the generalised estimation equation framework (see supplementary eFigures 3a and 3b). These models were chosen in place of log-binomial models to avoid problems with convergence. The robust estimator was used to correct the inflated variance found from the standard Poisson model, and to account for more than one birth in some women. 42 We also assessed a zero inflated Poisson model using a single zero inflation parameter applied to all observations to account for any excess of zeros in the model. This indicated no excess of zeros (P>0.9), further supporting the use of a multivariable Poisson regression model with cluster robust errors. In the modelling of risk analyses, we censored at the first SMM condition (ie, a mother with two SMM conditions was only counted once in the analysis). These models were used to determine adjusted relative risks and absolute risks. As we a priori assumed that outcomes might differ depending on gestational age, we included this as an interaction and adjusted for all of the other previously defined confounders. To explore potential residual confounding from confounders that we did not consider because evidence was lacking to suggest they would affect epidural use and SMM, we calculated an E-value. 43 The E-value was defined as the minimum strength of association that one confounder or several unmeasured confounders would need to have with both epidural analgesia and SMM, conditional on the confounders we adjusted for, to fully explain a specific exposure-outcome association. This was calculated using the EValue package (version 4.1.3).
Exploratory subgroup analyses
We repeated the same adjusted Poison regression modelling cluster robust sandwich estimators as described for the main analyses in three sets of subgroup analyses: Women with a medical indication and those without a medical indication, women delivering pre-term (<37 completed weeks of gestation) and those delivering at term or post term (≥37 completed weeks), and women with a medical indication and delivering preterm and those with no medical indication and delivering at term or post term.
In each of these analyses we tested statistical evidence for a difference between the two related subgroups by comparing a model with an interaction term (eg, interaction term between epidural analgesia during labour and medical indication—yes v no) using a likelihood ratio test comparing these two models. As analyses between subgroups are often under-powered, we considered a P value <0.01 to provide statistical evidence of a difference.
As our definition of medical indication for epidural analgesia included some components of the Bateman index score and BMI, we removed Bateman index score and maternal height and weight as confounding variables in the models of subgroup analyses that included medical indication (see supplementary eFigure 3b). Finally, to further model the effect of epidural analgesia on women with different underlying risk profiles for SMM, we analysed the association between epidural analgesia and SMM in women with and without an indication for epidural throughout the continuum of gestational ages using robust Poisson regression with non-linear splines.
Additional analyses
Given that epidural analgesia is only available to women delivering in an obstetric unit, we repeated the analyses restricted to births occurring within an obstetric unit (n=541 389, 95.4% of eligible women) and compared the results to our main analyses. We also provided additional subgroup analyses using WHO criteria of preterm births, and by iatrogenic or spontaneous preterm birth. 35
Dealing with missing confounder data
All eligible women (see supplementary eFigure 1) had complete data on epidural analgesia and outcome. Missing data on confounders varied, with the least for maternal age (0 missing) and most for maternal ethnicity (n=222 213, 39.2%) and illicit drug use (n=179 284, 31.6%) ( table 1 ). In total, 257 713 (45.4%) of eligible participants had missing data on ≥1 confounders. We imputed missing data for confounders using multiple imputations through chained equations to form 10 imputed datasets employing a predictive mean matching methodology. 44 Ten iterations assured data output stability, and 10 imputations guaranteed the accuracy of pooled variable effect size estimates.
Maternal and neonatal characteristics of pregnant women after exclusion of data missing for epidural analgesia during labour. Values are number (percentage) unless stated otherwise
- View inline
We also presented results from non-imputed, complete case analyses (n=309 503) and compared these with our main imputed analyses. In accordance with data regulation guidelines, we redacted any outcome or variable with five or fewer values, or any data that could be used to derive these redacted values.
Patient and public involvement
This study used anonymised data from national registries, focusing on the analysis of existing information without necessitating new direct contact with participants. Despite the inherent limitations of our approach, including the lack of allocated funding for direct patient involvement, we recognised the importance of incorporating public perspectives into our research. While direct involvement in designing the research question, the outcome measures, and study implementation was not feasible, our motivation was strongly influenced by discussions with members of the public and specific concerns highlighted by patients about maternal morbidity rates. These conversations, along with a priority setting exercise by the James Lind Alliance on the impact of epidural analgesia during labour, shaped our research focus. 16 Although formal patient and public involvement was not integrated into the study’s design, we engaged with the public by inviting a patient to review our manuscript, whose insights contributed to refining our presentation and interpretation of findings.
Study population and baseline characteristics
After exclusions, 567 216 women presented in labour in Scotland between 1 January 2007 and 31 December 2019 ( table 1 , see supplementary eFigure 1), of whom 39 601 (7.0%) delivered prematurely. Epidural analgesia was administered to 125 024 (22.0%) women. Of the 77 439 women with a medical indication for treatment, epidural analgesia was administered to 19 061 (24.6%) (see supplementary eFigure 1). Mothers who received epidural analgesia during labour were more likely to be primiparous, be from a less deprived socioeconomic group, be a former or non-smoker, be undergoing labour induction, give birth in an obstetric unit, and have a multiple birth, ≥1 comorbidities, a higher birthweight baby, and operative delivery ( table 1 ). SMM occurred in 2412 women (0.43%) and was more commonly observed in those with a medical indication for epidural analgesia (819/77 439, 1.06%) and in women delivering preterm (581/39 601, 1.47%) ( table 2 and supplementary eTable 4).
Observed events and adjusted relative risks for all outcomes for whole cohort
Temporal trends in SMM
The overall incidence of SMM (irrespective of epidural analgesia status) did not change annually during the study period (relative risk per year 1.00 (95% confidence interval (CI) 0.99 to 1.02, P=0.7) (see supplementary eTables 5 and 6).
Association between epidural analgesia and SMM and related outcomes
Epidural analgesia during labour was associated with a reduction in SMM (adjusted relative risk 0.65, 95% CI 0.50 to 0.85), SMM plus critical care admission (0.46, 0.29 to 0.73), and respiratory morbidity (0.42, 0.16 to 1.15), although the last of these had limited power with wide confidence intervals ( table 2 ).
In subgroup analyses, epidural analgesia was associated with a greater risk reduction in SMM in women with a medical indication for epidural analgesia (0.50, 0.34 to 0.72) versus those without a medical indication (0.67, 0.43 to 1.03); likelihood ratio of difference between subgroups, P<0.001 ( table 3 ). Similarly, we found a greater risk reduction in SMM in women receiving epidural analgesia and delivering prematurely (0.53, 0.37 to 0.76) compared with women delivering at term or post term (1.09, 0.98 to 1.21); likelihood ratio of difference between subgroups, P<0.001, and in women with a medical indication and delivering prematurely (0.36, 0.24 to 0.53) compared with women with no medical indication and delivering at term or post term (1.14, 0.99 to 1.31); likelihood ratio of difference between subgroups, P<0.001 ( table 3 ). The reduced risk of SMM with epidural analgesia seen in the whole cohort and in women with a medical indication for epidural analgesia was more pronounced as gestational age at birth decreased ( fig 1 ).
Comparison of outcomes between women with and without a medical indication for epidural analgesia during labour and those delivering preterm compared with at term or post term

Time varying adjusted absolute risks for severe maternal morbidity (%) in relation to gestational age (in weeks) for whole cohort, women with a medical indication for epidural analgesia, and women with no medical indication for epidural analgesia. Shading represents 95% confidence intervals
- Download figure
- Open in new tab
- Download powerpoint
Robustness of results and sensitivity analysis
E-values suggest our findings are not likely to be solely due to residual confounding (see supplementary eTable 7). Consistent results were observed in analyses limited to births in obstetric units with 24 hour access to obstetric and anaesthetic services (see supplementary eTables 8 and 9). Epidural analgesia was associated with reduced risk of SMM across all categories of preterm birth: extremely preterm (<28 weeks) gestations (0.36, 0.21 to 0.62), very preterm (28 to <32 weeks) gestations (0.48, 0.32 to 0.72), and moderate to late preterm (≥32 to 37 weeks) gestations (0.71, 0.56 to 0.88) (see supplementary eTable 10 ) . This effect was irrespective of whether the reason for the preterm birth was spontaneous or iatrogenic (see supplementary eTable 10). Similar results were seen in both complete case and unimputed datasets ( table 2 , table 3 , and supplementary eTable 11).
In this population based cohort study encompassing 567 216 births in Scotland, epidural analgesia during labour was associated with a 35% risk reduction in SMM and 54% risk reduction in SMM plus critical care admission across all births. These benefits were more pronounced in women with a medical indication for epidural analgesia compared with those without an indication, and in those who delivered preterm compared with those who did not deliver preterm. Women with a higher pre-existing morbidity risk, stemming from either medical or obstetric conditions, spontaneous preterm delivery, or conditions necessitating iatrogenic preterm delivery, face increased risks of adverse events related to their chronic comorbidities, diseases related to preterm birth, haemorrhage, and surgical complications. 4 45 46 47 Our results suggest that these risks might be effectively mitigated by use of epidural analgesia.
Comparison with other studies
Our findings enhance the limited existing literature, 8 9 and respond to a research priority identified by patients and clinical providers. 16 Given that mode of birth is unknown when the decision to use labour epidural analgesia is made, and that around 15% of SMM events will occur in the postnatal period, 10 our study provided a more accurate portrayal of the clinical situation than in the previous US study, which did not include postnatal SMM. 8 As few known modifiable risk factors for SMM exist, and as the incidence of SMM continues to rise, with this increase contributing to the global plateauing of maternal mortality, our findings provide a means to reduce SMM and maternal mortality. 1 4 45 That a large portion of women in whom epidural analgesia would generally be considered medically indicated did not receive one highlights a potential area for intervention.
The latest UK Mothers and Babies: Reducing Risk through Audits and Confidential Enquiries report underlines the uneven distribution of maternal morbidity and mortality, with deaths in women from black ethnic groups four times higher than in women from white ethnic groups, and the mortality risk twofold higher in women from the most deprived areas compared with least deprived areas. 13 Recent UK based studies have shown that women from ethnic minority groups and socioeconomically deprived areas are less likely to receive epidural analgesia, although the underlying reasons remain unclear. 14 15
Policy implications
Misinformation and misconceptions about epidural analgesia, particularly the effect on delivery mode and neonatal wellbeing, might contribute to inequities in epidural use during labour. 48 Existing research, including a Cochrane review of 40 randomised controlled trials and two Scottish population based studies, found that epidural analgesia was not causally linked to an increased risk of operative births and did not adversely affect neonatal or long term childhood outcomes, but these studies did not examine SMM or mortality. 11 49 50 Although a randomised controlled trial would be ideal for confirming our results, the global prevalence of epidural analgesia during labour, its established safety, and the urgency of this research make a strong case for applying our results in clinical practice. Our study offers valuable insights that can potentially reduce inequalities in maternal healthcare by providing robust evidence for individualised, person centred, and informed decision making. To maximise this effect, it is crucial to develop strategies that ensure women from diverse backgrounds, including those in preterm labour, have access to comprehensive information and support about the use of epidural analgesia.
The mechanism by which epidural analgesia could diminish SMM is likely multifaceted, involving closer medical oversight and haemodynamic monitoring, established intravenous access, fluid administration, blunting of physiological stress responses to labour, avoidance of the need for spinal or general anaesthesia for caesarean section, and faster escalation to definitive obstetric interventions. In essence, using epidural analgesia during labour alters the care pathway to one that enhances the capacity to manage adverse events. From these data it is not possible to separate the direct influence of epidural analgesia from the accompanying comprehensive care package. In the UK, implementing epidural analgesia inherently includes this bundle of enhanced care, which could be particularly advantageous for women at heightened risk of SMM.
Strengths and limitations of this study
Our study was undertaken in a large, unselected population cohort of linked mother-infant data over a 13 year period reflecting contemporary obstetric and anaesthetic practices. We adjusted for confounding variables that were defined before analyses started, used imputation for missing confounder data, and showed consistency between the confounder imputed and complete case analyses. The E-value suggested that bias due to unknown confounders was unlikely to have made a major contribution to our results, and additional sensitivity analyses support the robustness of our findings. We had too few cases of respiratory morbidity to provide precise estimates, highlighting the need for larger studies to explore this outcome. As other forms of anaesthesia may be used in more urgent clinical scenarios, such as major haemorrhage, this could have resulted in more favourable results in the epidural analgesia group. Nevertheless, our analysis aimed to reflect the divergent management pathways and outcomes depending on womens’ choice about epidural analgesia during labour. For instance, a woman with a functioning epidural is potentially more likely to undergo an assisted vaginal delivery than a caesarean section. In line with other UK based studies, we only accounted for postpartum haemorrhage when it necessitated critical care admission, potentially underestimating this morbidity. As a result, our findings might have been attenuated towards the null and strengthens our confidence in the effect seen between epidural analgesia and SMM. Our study excluded elective caesarean births, acknowledging that women undergo this procedure before labour starts and therefore by definition will not receive epidural analgesia during labour. While this analysis was not within our study’s scope, we recognise the importance of investigating anaesthetic choices in elective caesarean deliveries in future research, given the different risk profiles. We used widely validated area deprivation indices to indicate socioeconomic status. 32 However, we acknowledge that this may not always reflect individual socioeconomic positions (eg, well educated or wealthy women living in an area with a high deprivation score). As the population of Scotland is predominantly white, our results might not be generalisable to more diverse populations; however, the similarity of our results to those of a US study with an ethnically diverse population increases confidence in our findings. 8 We lacked data on systemic opioid use and maternal haemodynamics, both of which would have been valuable in elucidating the mechanisms by which epidural analgesia during labour could reduce the risk of SMM. Additionally, we did not have information on individual care providers and factors influencing maternal decision making about epidural analgesia. These aspects are crucial for understanding and dealing with potential barriers to the adoption of epidural analgesia during labour.
Conclusions
Our analysis of 567 216 births in Scotland indicates that epidural analgesia during labour is associated with a 35% risk reduction in SMM in all women. This effect was more pronounced in specific groups, showing a 50% risk reduction in women with predefined risk factors, and a 47% reduction in those delivering prematurely. These findings substantiate the current practice of recommending epidural analgesia during labour to women with known risk factors, underscores the importance of ensuring equitable access to such treatment, and highlights the importance of supporting women from diverse backgrounds to be able to make informed decisions relating to epidural analgesia during labour.
What is already known on this topic
Severe maternal morbidity (SMM) is a potentially life threatening outcome of pregnancy
Epidural analgesia during labour may reduce SMM, although evidence is limited
Assessing the effect of epidural analgesia during labour on obstetric outcomes is a research priority for women and healthcare providers
What this study adds
This study showed a reduced risk of SMM in women who received epidural analgesia during labour, with the greatest effects seen in those with a medical indication for epidural analgesia or delivering preterm
Encouraging the adoption of, and enhancing accessibility to, epidural analgesia for women in these higher risk categories could be instrumental in improving maternal health outcomes
Ethics statements
Ethical approval.
The Public Benefit and Privacy Panel for Health and Social Care (HSC-PBPP) of NHS Scotland provided ethical approval for the linkage (ref 1920-0097) and the NHS Greater Glasgow and Clyde Research and Development department approved the study (ref GN20PH059). The NHS Scotland electronic Data Research and Innovation Service linked and deidentified data before analysis.
Data availability statement
Depersonalised study data may be made available on request to accredited researchers who submit a proposal that is approved by NHS Scotland’s electronic Data Research and Innovation Service.
Acknowledgments
We would like to acknowledge the support of the eDRIS team (Public Health Scotland) for obtaining approvals, providing and linking data, and use of the secure analytical platform within the National Safe Haven.
Contributors: MS and SNM are joint senior authors. RJK, MS, and SMN conceived and designed the study. All authors acquired, analysed, or interpreted the data. RJK, MS, and SMN drafted the initial manuscript. All authors critically revised the manuscript for important intellectual content. RJK, MS, AK, and LOEH did the statistical analyses. RJK, MS, DAL, and SMN obtained funding. AK and LOEH provided administrative, technical, or material support. MS, DAL, and SMN supervised the study, obtained regulatory approval, and provided advice on analyses. RJK, AK, MS, and SMN had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. They are the guarantors. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding: This work was supported by an NHS Research Scotland senior researcher fellowship (RJK). DAL’s contribution is supported by the UK Medical Research Council (MC_UU_00032/05) and British Heart Foundation (CH/F/20/90003 and AA/18/1/34219). None of the funders had any role in the design, data analyses, or interpretation of results. The views expressed in this publication are those of the author(s) and not necessarily those of the UK NHS, or any funders or institutions acknowledged.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: support from NHS Research Scotland, the UK Medical Research Council, and British Heart Foundation; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work. Outside of the submitted work, RJK is a board member and research lead for Regional Anaesthesia UK and sits on the research council of the National Institute of Academic Anaesthesia Research Council. RJK has declared funding from NHS National Research Scotland (administered by NHS Greater Glasgow and Clyde), Wellbeing of Women, and the Chief Scientist Office (for research unrelated to this work in the past three years). SMN has participated in advisory boards and received speakers or consultancy fees from Access Fertility, Beckman Coulter, Ferring, Finox, Merck, MSD, Roche Diagnostics, and The Fertility Partnership. SMN has declared funding from the Chief Scientist Office, Wellbeing of Women, and National Institute of and Care Health Research (NIHR), for research unrelated to this work in the past three years. All funds for these grants go to and are managed and audited by the University of Glasgow. DAL has declared funding from the NIHR, Diabetes UK, and US National Institute of Research, for research unrelated to this work in the past three years. All funds for these grants go to and are managed and audited by the University of Bristol. DAL is a member of the UK Biobank strategic oversight committee, chair of the scientific advisory board for the Bradford Health Research Institute public health ActEarly programme, and chair of the NIHR-British Heart Foundation partnership working group on maternal cardiovascular health. She does not receive any payment for these activities. The authors declare no other relationships or activities that could appear to have influenced the submitted work.
Transparency: The lead author (RJK) affirms that the manuscript is an honest, accurate, and transparent account of the study being reported, that no important aspects of the study have been omitted, and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Dissemination to participants and related patient and public communities: To maximise the impact of our findings, we will employ a multifaceted dissemination strategy, targeting both academic and public audiences. Our plan includes leveraging social media platforms such as X (formerly Twitter) and Facebook to engage with the public, healthcare professionals, and policy makers. We will collaborate with patient advocacy groups (eg, the Maternal Mental Health Alliance ( https://maternalmentalhealthalliance.org/ ) and professional societies such as the Royal College of Obstetricians and Gynaecologists and Obstetric Anaesthetists’ Association to ensure our research reaches a wide audience and is presented in an accessible format, including lay summaries and infographics. Press releases will be distributed to both national and international media outlets, and findings will be presented at national and international conferences to foster academic and clinical discussion. We aim to facilitate a feedback loop by encouraging commentary and discussion through our social media channels, allowing us to gauge public and professional responses to our findings. This feedback will be invaluable for guiding future research directions and policy recommendations, ensuring our work remains aligned with patient needs and priorities.
Provenance and peer review: Not commissioned; externally peer reviewed.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/ .
- Geller SE ,
- Garland CE ,
- MacDonald EJ ,
- Cranfield K ,
- Victory G ,
- ↵ Centers for Disease Control and Prevention. Severe maternal morbidity in the United States. 2019. https://www.cdc.gov/reproductivehealth/maternalinfanthealth/severematernalmorbidity.html . Accessed 10 August 2022.
- Masterson JA ,
- Adamestam I ,
- Pattinson R ,
- WHO Working Group on Maternal Mortality and Morbidity Classifications
- ↵ Practice Guidelines for Obstetric Anaesthesia: An Updated Report by the American Society of Anesthesiologists Task Force on Obstetric Anaesthesia and the Society for Obstetric Anaesthesia and Perinatology . Anesthesiol 2016 ; 124 : 270 - 300 . OpenUrl CrossRef PubMed
- El Ayadi AM ,
- Jelliffe-Pawlowski L
- Guglielminotti J ,
- Friedman AM ,
- Chihuri S ,
- Driessen M ,
- Bouvier-Colle MH ,
- Khoshnood B ,
- Rudigoz RC ,
- Deneux-Tharaux C ,
- Pithagore6 Group
- Kuklina EV ,
- Barfield W ,
- Kearns RJ ,
- Gromski PS ,
- Iliodromiti S ,
- Lawlor DA ,
- ↵ NHS patient survey programme. 2019 survey of women’s experiences of maternity care. https://www.cqc.org.uk/sites/default/files/20200128_mat19_statisticalrelease.pdf . Accessed 18 July 2022.
- Bamber JH ,
- Goldacre R ,
- Halliday L ,
- Kyzayeva A ,
- Nelson SM ,
- ↵ James Lind Alliance. Anaesthesia and Perioperative Care Top 10. 2015. https://www.jla.nihr.ac.uk/priority-setting-partnerships/anaesthesia-and-perioperative-care/top-10-priorities/ . Accessed 15 June 2022.
- von Elm E ,
- Altman DG ,
- Pocock SJ ,
- Gøtzsche PC ,
- Vandenbroucke JP ,
- STROBE Initiative
- ↵ NSS Information and Intelligence. Data Quality Assurance Assessment of SMR02 (Maternity Inpatient and Day Case) Data; Scotland 2017-2018. Isdscotland.org. 2019. https://www.isdscotland.org/Products-and-Services/Data-Quality/docs/20191023-Assessment-of-SMR02-Data-Scotland-2017-2018.pdf . Accessed 14 June 2022.
- Crossley JA ,
- ↵ World Health Organization. The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines: Geneva: WHO; 1992. https://apps.who.int/iris/handle/10665/37958 . Accessed 20 July 2022.
- ↵ UK National Health Service Operating Procedure Codes Supplement. OPCS-4.10. 2022. https://digital.nhs.uk/data-and-information/information-standards/information-standards-and-data-collections-including-extractions/publications-and-notifications/standards-and-collections/dapb0084-opcs-classification-of-interventions-and-procedures . Accessed 20 July 2022.
- ↵ Scottish Intensive Care Society Audit Group. Annual report: audit of critical care in Scotland 2022. https://publichealthscotland.scot/media/21021/full-report.pdf. Accessed 22 November 2023).
- ↵ Vedagiri Sai R, Rappai G, Johnstone C. Survey of obstetric epidural anaesthetic practises in Scotland [Abstract]. Presented at the Obstetric Anaesthetists’ Association Annual Meeting, Bournemouth, 2013: 43.
- Halpern SH ,
- Soliman A ,
- Ioscovich A
- McNulty J ,
- Kurinczuk JJ ,
- Dellinger RP ,
- Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup
- Tidswell R ,
- Brealey D ,
- van der Zander B ,
- Gilthorpe MS ,
- Liśkiewicz M ,
- ↵ Scotland Home ISD. Data dictionary A-Z. https://www.ndc.scot.nhs.uk/Dictionary-A-Z/Definitions/index.asp?Search=E&ID=243&Title=Ethnic%20Group . Accessed 15 June 2022.
- ↵ Scottish Government. Scottish index of multiple deprivation 2020: introductory booklet. https://www.gov /scot/publications/scottish-index-multiple-deprivation-2020/. Accessed 15 June 2022.
- Bateman BT ,
- Hernandez-Diaz S ,
- Brocklehurst P ,
- Hollowell J ,
- Birthplace in England Collaborative Group
- ↵ World Health Organization. Preterm birth. https://www.who.int/news-room/fact-sheets/detail/preterm-birth . Accessed 12 May 2023.
- American College of Obstetricians and Gynecologists
- VanderWeele TJ ,
- Kontopantelis E ,
- Sperrin M ,
- Morelli R ,
- Di Mascio D ,
- Grobman WA ,
- Eunice Kennedy Shriver National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network ,
- Eunice Kennedy Shriver National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network
- D’Souza RS ,
- D’Souza S ,
- Anim-Somuah M ,
IMAGES
VIDEO
COMMENTS
A conclusion in a research paper is the final section where you summarize and wrap up your research, presenting the key findings and insights derived from your study. The research paper conclusion is not the place to introduce new information or data that was not discussed in the main body of the paper.
Having summed up your key arguments or findings, the conclusion ends by considering the broader implications of your research. This means expressing the key takeaways, practical or theoretical, from your paper—often in the form of a call for action or suggestions for future research. ... Writing a Research Paper Conclusion | Step-by-Step ...
The conclusion is intended to help the reader understand why your research should matter to them after they have finished reading the paper. A conclusion is not merely a summary of the main topics covered or a re-statement of your research problem, but a synthesis of key points derived from the findings of your study and, if applicable, where you recommend new areas for future research.
Begin with a clear statement of the principal findings. This will reinforce the main take-away for the reader and set up the rest of the discussion. Explain why the outcomes of your study are important to the reader. Discuss the implications of your findings realistically based on previous literature, highlighting both the strengths and ...
Step 1: Answer your research question. Step 2: Summarize and reflect on your research. Step 3: Make future recommendations. Step 4: Emphasize your contributions to your field. Step 5: Wrap up your thesis or dissertation. Full conclusion example. Conclusion checklist. Other interesting articles.
Research Paper Conclusion. Definition: A research paper conclusion is the final section of a research paper that summarizes the key findings, significance, and implications of the research. It is the writer's opportunity to synthesize the information presented in the paper, draw conclusions, and make recommendations for future research or ...
Results vs. discussion vs. conclusion. Your results section should objectively report your findings, presenting only brief observations in relation to each question, hypothesis, or theme. It should not speculate about the meaning of the results or attempt to answer your main research question.
Step 1: Restate the problem. Always begin by restating the research problem in the conclusion of a research paper. This serves to remind the reader of your hypothesis and refresh them on the main point of the paper. When restating the problem, take care to avoid using exactly the same words you employed earlier in the paper.
Begin your conclusion by restating your thesis statement in a way that is slightly different from the wording used in the introduction. Avoid presenting new information or evidence in your conclusion. Just summarize the main points and arguments of your essay and keep this part as concise as possible. Remember that you've already covered the ...
The results section should state the findings of the research arranged in a logical sequence without bias or interpretation. A section describing results should be particularly detailed if your paper includes data generated from your own research. ... In this model, it is helpful to provide a brief conclusion that ties each of the findings ...
These conclusions might arise from a comparison between your results and the findings of other studies. They will, almost certainly, be developed with reference to the aim and objectives of the research. While there will be no debate over the results, the conclusions could well be contentious.
Peer-reviewed: Research findings are often subject to a rigorous peer-review process, in which experts in the field review the research methods, data analysis, and conclusions of the study. This helps to ensure the validity and reliability of the findings.
Research Summary. Definition: A research summary is a brief and concise overview of a research project or study that highlights its key findings, main points, and conclusions. It typically includes a description of the research problem, the research methods used, the results obtained, and the implications or significance of the findings.
You should: Discuss your conclusions in order of most to least important. Compare your results with those from other studies: Are they consistent? If not, discuss possible reasons for the difference. Mention any inconclusive results and explain them as best you can. You may suggest additional experiments needed to clarify your results.
A conclusion must be more extensive and encompassing compared to a particular finding and, in the same vein, various findings may be integrated into a single conclusion (Baron, 2008). ... This strategy is useful in writing a conclusion of research for scientific papers as well as experiments (Writing Tutorial Services, Indiana University, n.d.).
The discussion section is often considered the most important part of your research paper because it: Most effectively demonstrates your ability as a researcher to think critically about an issue, to develop creative solutions to problems based upon a logical synthesis of the findings, and to formulate a deeper, more profound understanding of the research problem under investigation;
The function of your paper's conclusion is to restate the main argument. It reminds the reader of the strengths of your main argument (s) and reiterates the most important evidence supporting those argument (s). Make sure, however, that your conclusion is not simply a repetitive summary of the findings because this reduces the impact of the ...
A conclusion is the final paragraph of a research paper and serves to help the reader understand why your research should matter to them. The conclusion of a conclusion should: Restate your topic and why it is important. Restate your thesis/claim. Address opposing viewpoints and explain why readers should align with your position.
In the conclusion: This study examined elementary schoolchildren's preferences among four types of play with new peer acquaintances. 2. Summarize the findings/argument. Your research paper conclusion should also revisit the evidence, findings, and limitations of your research, but as an overview, not in detail.
Conclusion, on the other hand, gives a summarized deductive or inductive explanation and interpretation (usually influenced by the research's orientation or point of view) of the main findings.
1.3 Conclusion. A conclusion is a judgment or interpretation of the findings based on the evidence collected during the evaluation. It is typically expressed in terms of what the findings mean or what can be inferred from them. Conclusions should be logical, evidence-based, and free from personal bias or opinion.
These findings are notable given that prior research has focused primarily on a single brain imaging modality, limiting the nature and scope of conclusions drawn about the role of diet and ...
Table of contents. What not to include in your discussion section. Step 1: Summarize your key findings. Step 2: Give your interpretations. Step 3: Discuss the implications. Step 4: Acknowledge the limitations. Step 5: Share your recommendations. Discussion section example. Other interesting articles.
Conclusions . Interventions were successful in reducing depressive symptoms, even though treatment fidelity was decreased due to the COVID-19 pandemic. ... There is, however, a profound research gap concerning the effectiveness of psychotherapy for the difficult-to-reach group of home-living vulnerable older adults with care needs and ...
This article reports the findings of a survey from Clinical Scientists (Physical Sciences modality) about their experiences with their regulator, and their perception of the quality and safety of that regulation. ... Conclusions. The Clinical Scientist (Physical Sciences) professional registrants rated the performance of their regulator more ...
A ccording to recent research, pedestrians are at a greater risk of being struck by electric or hybrid cars than those powered by petrol or diesel. The study, which underwent peer review and was ...
This research will aid in formulating design guidelines tailored for various stakeholders such as architectural designers involved in high-rise residential timber building developments. ... Key findings included (1) the average space efficiency within the examined cases was recorded at 83%, exhibiting variances ranging from 70% to 93% across ...
Reclaimed asphalt pavement (RAP) is a valuable material that can be recycled and reused in road engineering to reduce environmental impact, resource utilization, and economic costs. However, the application of RAP in road engineering presents both opportunities and challenges. This study visually analyzes the knowledge background, research status, and latest knowledge structure of literature ...
Our findings enhance the limited existing literature,8 9 and respond to a research priority identified by patients and clinical providers.16 Given that mode of birth is unknown when the decision to use labour epidural analgesia is made, and that around 15% of SMM events will occur in the postnatal period,10 our study provided a more accurate ...